Manho Kim and Jae-Kyu Roh Keun-Hwa Jung, Kon Chu, Sang
advertisement

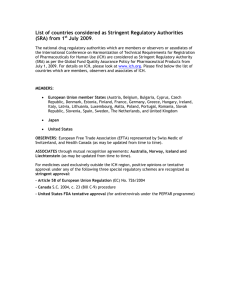
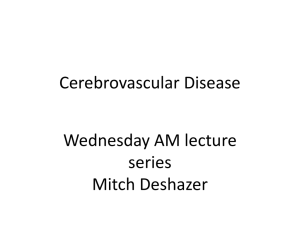
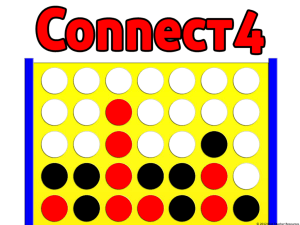
HMG-CoA Reductase Inhibitor, Atorvastatin, Promotes Sensorimotor Recovery, Suppressing Acute Inflammatory Reaction After Experimental Intracerebral Hemorrhage Keun-Hwa Jung, Kon Chu, Sang-Wuk Jeong, So-Young Han, Soon-Tae Lee, Jin-Young Kim, Manho Kim and Jae-Kyu Roh Stroke. 2004;35:1744-1749; originally published online May 27, 2004; doi: 10.1161/01.STR.0000131270.45822.85 Stroke is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 2004 American Heart Association, Inc. All rights reserved. Print ISSN: 0039-2499. Online ISSN: 1524-4628 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://stroke.ahajournals.org/content/35/7/1744 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Stroke can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Stroke is online at: http://stroke.ahajournals.org//subscriptions/ Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013 HMG-CoA Reductase Inhibitor, Atorvastatin, Promotes Sensorimotor Recovery, Suppressing Acute Inflammatory Reaction After Experimental Intracerebral Hemorrhage Keun-Hwa Jung, MD; Kon Chu, MD; Sang-Wuk Jeong, MD; So-Young Han, MS; Soon-Tae Lee, MD; Jin-Young Kim, BS; Manho Kim, MD, PhD; Jae-Kyu Roh, MD, PhD Background and Purpose—Statins have neuroprotective effects on ischemic stroke. They modify the endothelial function, increase blood flow, and inhibit thrombus formation, which are independent of lipid-lowering effects. However, whether statins have a protective effect toward hemorrhagic stroke is yet unknown. To test this possibility, we attempted to determine the effect of atorvastatin on experimental intracerebral hemorrhage (ICH). Methods—ICH was induced using stereotaxic infusion of collagenase into the left basal ganglia in adult rats. Atorvastatin (1 mg/kg or 10 mg/kg) or phosphate-buffered saline was administered for 2 weeks. To monitor the sensorimotor deficits, limb placing and Rotorod tests were performed. Hematoma volume, brain water content, and hemispheric atrophy were analyzed. Immunohistochemical staining for myeloperoxidase (MPO), microglia (OX42), inducible nitric oxide synthase (iNOS), or endothelial nitric oxide synthase (eNOS) was performed. Perihematomal cell death was determined by TUNEL staining. Results—The atorvastatin-treated ICH group showed better performance on Rotorod and limb placing tests when compared with the vehicle-treated group (P⬍0.01). The hematoma volumes between groups were not different, but the brain water content and hemispheric atrophy were reduced in the atorvastatin-treated ICH group. Atorvastatin reduced TUNELpositive cells, iNOS expression, and MPO-positive or OX42-positive cells in the perihematomal regions in a dose-dependent manner, whereas it increased eNOS expression. Conclusion—The present study shows that atorvastatin reduces the perihematomal cell death via antiinflammation, which is associated with sensorimotor recovery after experimental ICH. (Stroke. 2004;35:1744-1749.) Key Words: HMG-CoA reductase inhibitors 䡲 intracerebral hemorrhage 䡲 brain edema 䡲 apoptosis 䡲 inflammation I ntracerebral hemorrhage (ICH) represents 15% of all strokes in Western populations and a higher proportion (20% to 30%) in Asian and black populations.1 The mechanisms by which cellular injury occurs after ICH include mechanical destruction or displacement caused by blood accumulation.2 Inflammation and impairment of cerebral blood flow (CBF) around the blood clot contribute to delayed neuronal death.3,4 The suppression of the inflammatory response has been reported to reduce brain edema and tissue damage and improve functional outcome in experimental ICH.5– 8 Statins, 3-hydroxy-3-methyl-glutaryl-coenzyme A (HMGCoA) reductase inhibitors, have been shown to have many pleiotropic properties on the nervous and vascular systems, independent of cholesterol-lowering effect, and provide neuroprotection with beneficial effects on endothelial function, immunomodulation, and impeding excitotoxic cell injury via antiinflammatory actions and angiogenesis/neurogenesis.9 –22 The putative neuroprotective actions of statins may lead to functional restoration after ICH. However, the effects of statins in the ICH paradigm are not known at present. In the present study, we investigate whether atorvastatin, when administered after ICH, can reduce edema formation, inflammation, and cell death, and subsequently promote neurological recovery in a rat model of ICH. Materials and Methods Induction of Intracerebral Hemorrhage and Atorvastatin Administration Male Sprague-Dawley rats (12 weeks old; Genomics, Seoul, ROK), weighing 200 to 220 grams, were used in this experiment and our protocols were institutionally approved in accordance with NIH Received January 23, 2004; final revision received March 10, 2004; accepted March 29, 2004. From Stroke and Neural Stem Cell Laboratory in Clinical Research Institute (K.-H.J., K.C., S.-Y.H., S.-T.L., J.-Y.K., M.K., J.-K.R.), Department of Neurology, Seoul National University Hospital, Seoul National University, Seoul, South Korea; the Department of Neurology (K.C.), Seoul National Hospital, Seoul, South Korea; and the Department of Neurology (S.-W.J.), Ilsan Paik Hospital, Inje University, Goyang, South Korea. K.-H.J. and K.C. contributed equally to this work. Correspondence to Dr Jae-Kyu Roh, Department of Neurology, Seoul National University Hospital, 28, Yongon-Dong, Chongro-Gu, Seoul, 110-744, South Korea. E-mail rohjk@snu.ac.kr © 2004 American Heart Association, Inc. Stroke is available at http://www.strokeaha.org DOI: 10.1161/01.STR.0000131270.45822.85 1744 Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013 Jung et al Guide for the Care and Use of Laboratory Animals. Experimental groups consisted of rats subjected to ICH (n⫽99) and normal control rats (n⫽27). Experimental ICH was induced by the stereotaxic intrastriatal administration of bacterial collagenase type IV (Sigma), as previously described.23,24 After an intraperitoneal injection of 1% ketamine (30 mg/kg; Sigma) and xylene hydrochloride (4 mg/kg; Sigma), rats were placed in a stereotaxic frame (David Kopf Instruments). A burr hole was made, and a 30-gauge Hamilton syringe needle was inserted through a burr hole into the striatum (location: 3.0 mm left lateral to the midline, 0.2 mm posterior to bregma, 6 mm in depth below the skull). ICH was induced by the administration of 1 L containing 0.23 U of collagenase over 5 minutes. After infusion, craniotomy holes were sealed with bone wax and wounds were sutured. Rectal temperature was maintained at 37⫾0.5°C using a thermistor-controlled heating blanket. Six hours after ICH induction (considering the recovery time from anesthesia), rats were fed atorvastatin (prescription formulation; Pfizer Inc), using 20-mm feeding needles (Popper and Sons Inc), dissolved in phosphate-buffered saline, 1 mg/kg (n⫽21) or 10 mg/kg (n⫽39) daily for 3 days or 14 days (to the rats assigned for the behavioral testing). ICH rats fed vehicle alone served as ICH control group (n⫽39), and normal rats fed vehicle alone (n⫽18) or 10 mg/kg atorvastatin (n⫽9) served as normal control group. Behavioral Testing Behavioral testing was performed weekly for atorvastatin-treated (10 mg/kg) or vehicle-treated ICH group (n⫽9 per group) using the modified limb placing (MLPT) and Rotorod tests,23 which were monitored by blinded investigators for group allocation. Morphometric Measurement of Hematoma Volume and Hemispheric Atrophy At 3 days after ICH, brains from atorvastatin-treated (10 mg/kg) or vehicle-treated ICH rats (n⫽9 per group) were cut coronally through the needle entry site (identifiable on the brain surface), and then serial slices (1-mm thickness) both anterior and posterior to the needle entry site were obtained. Digital photography of the serial slices was taken and hematoma volume was measured using image analyzer program (Image Pro-Plus; Media Cybernetics). The total hematoma volume (mm3) was calculated by summing the clot area in each section and multiplying by the distance between sections.24 At 42 days after ICH, the rats used for behavior test were euthanized to analyze hemispheric atrophy. Three sections through the needle entry site and sites 1.0 mm anterior and 1.0 mm posterior to plane were Nissl-stained. The morphometric analyses involved the area of the striatum, cerebral cortex, and ventricle, as well as the whole hemisphere. The total hemispheric areas of each section were traced and measured using image analyzer. The hemispheric atrophy was expressed as a percentage of contralateral hemispheric area.23 Analysis of Brain Water Content, Histology, and Immunohistochemistry We determined the endpoint of 3 days for experiments on water content, histology, and immunohistochemistry, because inflammatory reaction has been shown to be maximal at 48 to 72 hours after ICH.3 Atorvastatin-treated (1 mg/kg or 10 mg/kg) or vehicle-treated ICH rats and atorvastatin-treated (10 mg/kg) or vehicle-treated normal rats (n⫽9 per group) were euthanized to measure brain water content. The brains were divided into 2 hemispheres along the midline, and the cerebellum and the brain stem were removed. The brain samples were immediately weighed on an electronic analytical balance to obtain the wet weight. The samples were then dried in a gravity oven at 100°C for 24 hours to obtain the dry weight. Water content was expressed as a percentage of wet weight: the formula for calculation was (wet weight⫺dry weight)/(wet weight) ⫻ 100.24 At the same time, atorvastatin-treated (1 mg/kg or 10 mg/kg) or vehicle-treated ICH rats (n⫽9 per group) and vehicle-treated normal rats (n⫽6) were euthanized for histological analysis. We removed the brains and cryopreserved tissue blocks for cryostat sectioning (30 m thickness). Euthanization or immunohistochemistry was Effect of Atorvastatin on ICH 1745 processed as described previously.23,24 Rabbit anti-human myeloperoxidase (MPO) (1:100; DAKO Corporation) and mouse anti-rat OX42 primary antibodies (1:500; Chemicon) were used as markers for neutrophil and microglia, respectively. MPO-positive or OX42positive cells were identified and counted. The iNOS and eNOS immunohistochemistries were performed with anti-iNOS antibody (1:300, mouse monoclonal; Transduction Laboratories) and antieNOS antibody (1:500, rabbit polyclonal; Transduction Laboratories), respectively. FITC-conjugated anti-mouse IgG (1:100; Jackson ImmunoResearch) and Cy3-conjugated anti-rabbit IgG antibodies (1:500; Jackson ImmunoResearch) were used for the secondary antibodies. Western Blot Western blotting was performed on perihematomal tissues dissected out from a 2-mm-thick coronal brain slice cut at the level of the needle insertion. A similar segment was isolated in normal control rats. Western blotting of eNOS (n⫽3 per group) was performed with a rabbit polyclonal eNOS antibody (1:500; Transduction Laboratories) as previously described.25 Using the same membrane, we also performed immunoblotting of -actin with a mouse anti–-actin monoclonal antibody (1:2000; Sigma) to standardize the expression of eNOS. Equal amounts of protein (20 g) for each group were assayed and immunoreactivity was visualized by enhanced chemiluminescence. TUNEL Assay Atorvastatin-treated (1 mg/kg or 10 mg/kg) or vehicle-treated ICH rats (n⫽9 per group) and vehicle-treated normal rats (n⫽6) were euthanized with sodium pentobarbital at 3 days after ICH for TUNEL staining. The TUNEL procedure for in situ detection of DNA fragmentation was performed as previously described.24,26 Only TUNEL-stained cells that showed deep punctate staining with perinuclear chromatin condensation were considered apoptotic and were included for quantitation. Cell density counts were performed on sections counterstained with toluidine blue. Cell Quantification Quantitative analysis of the positively stained cell number was performed in the perihematomal regions of 3 axial sections (1-mm width) staining through the center of the hemorrhagic lesion by 2 independent investigators who were blinded to the group allocation. Total counts in the measured sections were converted into cell densities for comparison between the ICH groups. Statistical Analysis All data in this study are presented as the mean⫾SD. Data were analyzed by unpaired Student t test if they were normally distributed (Kolmogorov-Smirov test, P⬎0.05). Otherwise, we used Mann– Whitney U test and specified the test used. Two-tailed value of P⬍0.05 was considered significant. Results Physiological Parameters All animals survived the surgery. The physiological parameters, including mean arterial blood pressure, blood gases, serum glucose, and body temperatures, were not significantly different in any experimental groups before, during, or after ICH. Atorvastatin Improved the Sensorimotor Deficits After Experimental Rats The atorvastatin-treated (10 mg/kg) ICH group showed a better performance on the MLPT after 21 days and the Rotorod after 14 days compared with the vehicle-treated group, and the effects persisted up to 28 days. At day 28, the Rotorod performance showed 80% improvement of pre- Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013 1746 Stroke July 2004 Figure 1. Modified limb placing test and Rotorod test. Atorvastatin-treated ICH group showed a better performance on the MLPT (A) and the Rotorod (B) compared with the vehicle-treated group;. n⫽9 per group; *P⬍0.05 compared with ICH-only group. trained level, whereas the vehicle-treated ICH group showed 40% (Figure 1; n⫽9 for each group, P⬍0.05, Mann–Whitney U test). The initial body weights and those over the course of 4 weeks were similar. Atorvastatin Reduced Brain Water Content and Long-Term Hemispheric Atrophy The hematoma volume was 19.16⫾1.99 mm3 in the vehicletreated ICH group and 18.83⫾1.58 mm3 in the atorvastatintreated group by 3 days (Figure 2A; n⫽9 for each group, P⫽0.66, Student t test). Brain water contents of the lesioned hemisphere were reduced in atorvastatin-treated ICH group with dose-dependency (Figure 2B; n⫽9 for each group, P⬍0.05, Mann–Whitney U test). Brain water contents of the nonlesioned hemisphere were not different. Hemispheric area analysis showed an atrophy of lesioned hemisphere in both vehicle-treated and atorvastatin-treated ICH groups (Figure 2C; n⫽9 for each group). However, the atorvastatin-treated ICH group showed lesser hemispheric and striatal atrophy than the vehicle-treated group (15.00⫾2.16% versus 24.52⫾4.79% and 15.50⫾2.38% versus 27.00⫾3.91%, respectively; P⬍0.05, Mann–Whitney U test), whereas cortical atrophy was not different between both groups (5.75⫾2.06% versus 6.75⫾2.50%; P⫽0.46). Atorvastatin Decreased TUNEL-Positive Cells in the Perihematomal Regions After 3 days, a high density of TUNEL-positive stained cells was present within the hemorrhage as well as in the surrounding periphery (Figure 3). Counterstaining with toluidine blue revealed that the TUNEL-positive cells were not leukocytes. TUNEL-positive cells in atorvastatin-treated groups were significantly decreased by 42% (10 mg/kg) and 24% (1 mg/kg) compared with vehicle-treated group (n⫽9 for each group, P⬍0.05, Student t test). Figure 2. Hematoma volume, brain water content, and hemispheric atrophy. Hematoma volume was not different between vehicle-treated and atorvastatin-treated ICH groups (A). Brain water content was reduced in the lesioned hemisphere (B), and hemispheric and striatal atrophy of lesioned side were reduced in the atorvastatintreated ICH group (C); n⫽9 per group for each experiment; bars represent mean⫾SD; *P⬍0.05 compared with vehicle-treated group. Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013 Jung et al Effect of Atorvastatin on ICH 1747 Figure 3. Perihematomal cell death. More abundant TUNEL-positive cells were observed in the perihematomal region of vehicle-treated ICH group (A) than atorvastatin-treated group (B). Quantitative analysis showed less TUNEL-positive cells in the atorvastatin-treated ICH group in a dose-dependent manner (C); n⫽9 per group; scale bar⫽50 m. Bars represent mean⫾SD. *P⬍0.05 compared with ICH-only group. Atorvastatin Decreased iNOS Expression and MPO-Positive or OX42-Positive Cells Atorvastatin Increased eNOS Expression in the Perihematomal Regions iNOS immunoreactivity was increased in the perihematomal regions, but it was attenuated by ⬇50% in the atorvastatintreated (10 mg/kg) ICH group (Figure 4A and 4B). A significant infiltration of MPO-positive or OX42-positive cells adjacent to the hematoma was also detected 3 days after ICH (Figure 4C to 4F). Quantitative analysis (Figure 4G and 4H) showed 36% reduction in MPO⫹ and 42% in OX42⫹ cells in the atorvastatin-treated (10 mg/kg) ICH group compared with the vehicle-treated group, whereas it showed a minimal reduction in the atorvastatin-treated (1 mg/kg) ICH group. The eNOS expression in the perihematomal regions was increased in the atorvastatin-treated (10 mg/kg) ICH group compared with the vehicle-treated group (Figure 5). In addition, a 2-fold increase in eNOS protein was detected by Western blotting after 3 days of 10 mg/kg treatment, whereas the increase was minimal after 1 mg/kg treatment (Figure 5C). Discussion In the present study, atorvastatin, when administered to collagenase-induced ICH model, reduced hemispheric water content and perihematomal cell death, decreased iNOS Figure 4. Immunohistochemistry for iNOS, MPO, and OX42 in the perihematomal region. Immunohistochemistry for iNOS in vehicle-treated ICH rats showed an increment of iNOS expression around the blood clot (A), whereas this increment was attenuated in atorvastatin-treated ICH rats (B). MPO⫹ neutrophils (C, D) and OX42⫹ (E, F) microglias were clustered around the blood clot. The numbers of MPO⫹ and OX42⫹ cells were decreased by atorvastatin treatment. Quantitative analysis (G, H) shows a dose-dependent reduction in MPO⫹ and in OX42⫹ cells; n⫽9 per group; magnification ⫻100; bars represent mean⫾SD; *P⬍0.05 compared with vehicle-treated ICH group. Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013 1748 Stroke July 2004 Figure 5. Immunohistochemistry and Western blotting for eNOS expression in the ICH brain. Atorvastatin-treated (10 mg/kg) ICH rats (B) show the increased eNOS expression in the perihematomal regions compared with vehicle-treated rats (A). Arrows indicate the increased expression of eNOS in the vessel. Magnification ⫻200. Western blot of eNOS in the ICH brain shows a dose-dependent eNOS expression by atorvastatin treatment. The bands of -actin in the lower panel are shown for internal standards. n indicates normal control; v, vehicle; 1, 1 mg/kg atorvastatin; 10, 10 mg/kg atorvastatin. expression, decreased infiltration of leukocytes and microglia, and increased eNOS expression in the perihematomal regions while concomitantly improving the functional outcome and decreasing the long-term hemispheric atrophy. Our data provide initial evidence that statin exerts protection against ICH via modulation of inflammation. Despite the similar hematoma volumes between groups, the neurological deficit after ICH was significantly ameliorated by atorvastatin. These findings suggest that sensorimotor deficits after ICH are not simply attributed to the mechanical destruction by the hematoma, supporting that inflammatory response, brain edema, or impairment of CBF around the blood clot might also contribute to functional impairment.2,3 Cell necrosis, perihematomal cell apoptosis, and axonal loss lead to brain atrophy after ICH, which progresses up to 3 months.2– 4 In the present study, atorvastatin treatment for 14 days (targeting a period of active inflammation or cell death after ICH) reduced a brain atrophy when measured at 42 days, and this was associated with attenuation of apoptosis. Apoptosis after ICH begins at 24 hours, peaks at 3 days, and continues at least 4 weeks.27 The perihematomal ischemia and inflammatory responses have been suggested to mediate the apoptosis.3,27 Therefore, the modulation of inflammation and preservation of CBF by atorvastatin might help ameliorate the cell death after ICH, giving the reduction in hemispheric atrophy and the functional improvement. However, it remains to be established if the injection of bacterial collagenase by itself causes an inflammatory response and worsened accompanying cerebral edema. Further studies using autologous blood-injected ICH models are needed. Toxic blood components can induce an inflammatory response in and around the hematoma.4 Infiltrating inflammatory cells or activated microglia enhance the production of proinflammatory cytokines, cyclooxygenase-2, and iNOS, presumably inducing the signal pathway to mediate the apoptosis.27,28 Inhibition of these inflammatory substances has been reported to reduce a brain edema and tissue damage and improve functional outcome in experimental ICH.5– 8 Statins cause a dose-dependent inhibition of multiple steps of leukocyte recruitment and migration into the central nervous system, either directly by suppressing cell surface receptors and adhesion molecules on nervous or vascular tissues or indirectly by binding to leukocyte function-associated antigen.29 –31 Statins can also suppress the proinflammatory mediators such as TNF-␣, IFN-␥, and iNOS.9,32 Recent data have demonstrated that statins act beneficially in numerous inflammatory conditions such as cardiac transplantation (in humans)18 and experimental autoimmune encephalomyelitis (in mice).20 –22 In our experiment, attenuation of inflammatory response by atorvastatin might mediate decreasing brain edema and cell death. Statins have also been shown to enhance CBF in experimental stroke.14 –16 Statins upregulate eNOS in ischemic stroke12–15 and experimental subarachnoid hemorrhage.11 Enhancement of CBF and neuroprotective effects of statins are completely absent in eNOS-deficient mice,15 indicating that enhanced eNOS activity by statins is the predominant mechanism by which these agents protect against cerebral injury. In our experiment, eNOS was upregulated in the perihematomal regions. Thus, atorvastatin might attenuate the ischemic neuronal injury in the perihematomal ischemic penumbra by enhancing CBF. To clarify other pleiotropic effects of statin including neurogenesis and angiogenesis, further investigations are needed. The patients with ischemic stroke often undergo hemorrhagic stroke. Up to 30% of all ischemic strokes develop hemorrhagic transformations, and thrombolytic therapy of ischemic stroke can lead to serious complications of ICH. Therefore, in practice, it is important to identify agents that are safe and efficacious in treating both ischemic and hemorrhagic stroke. Taken together with the pleiotropic effects of statin in acute ischemic stroke, statin might be a useful agent in these complex conditions. Acknowledgments This study was supported by the 21st Century Frontier Research Fund of Ministry of Science & Technology (M102KL01000102K1201-01310), Republic of Korea. References 1. Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344: 1450 –1460. 2. Del Bigio MR, Yan HJ, Buist R, Peeling J. Experimental intracerebral hemorrhage in rats. Magnetic resonance imaging and histopathological correlates. Stroke. 1996;27:2312–2319. 3. Xue M, Del Bigio MR. Intracerebral injection of autologous whole blood in rats: time course of inflammation and cell death. Neurosci Lett. 2000;283:230 –232. Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013 Jung et al 4. Gong C, Hoff JT, Keep RF. Acute inflammatory reaction following experimental intracerebral hemorrhage in rat. Brain Res. 2000;871: 57– 65. 5. Mayne M, Fotheringham J, Yan HJ, Power C, Del Bigio MR, Peeling J, Geiger JD. Adenosine A2A receptor activation reduces proinflammatory events and decreases cell death following intracerebral hemorrhage. Ann Neurol. 2001;49:727–735. 6. Mayne M, Ni W, Yan HJ, Xue M, Johnston JB, Del Bigio MR, Peeling J, Power C. Antisense oligodeoxynucleotides inhibition of tumor necrosis factor-alpha expression is neuroprotective after intracerebral hemorrhage. Stroke. 2001;32:240 –248. 7. Peeling J, Yan HJ, Corbett D, Xue M, Del Bigio MR. Effect of FK-506 on inflammation and behavioral outcome following intracerebral hemorrhage in rat. Exp Neurol. 2001;167:341–347. 8. Power C, Henry S, Del Bigio MR, Larsen PH, Corbett D, Imai Y, Yong VW, Peeling J. Intracerebral hemorrhage induces macrophage activation and matrix metalloproteinases. Ann Neurol. 2003;53: 731–742. 9. Vaughan CJ, Murphy MB, Buckley BM. Statins do more than just lower cholesterol. Lancet. 1996;348:1079 –1082. 10. Laufs U, LaFata V, Plutzky J, Liao JK. Upregulation of endothelial nitric oxide synthase by HMG CoA reductase inhibitors. Circulation. 1998;97:1129 –1135. 11. McGirt MJ, Lynch JR, Parra A, Sheng H, Pearlstein RD, Laskowitz DT, Pelligrino DA, Warner DS. Simvastatin increases endothelial nitric oxide synthase and ameliorates cerebral vasospasm resulting from subarachnoid hemorrhage. Stroke. 2002;33:2950 –2256. 12. Laufs U, Gertz K, Huang P, Nickenig G, Bohm M, Dirnagl U, Endres M. Atorvastatin upregulates type III nitric oxide synthase in thrombocytes, decreases platelet activation, and protects from cerebral ischemia in normocholesterolemic mice. Stroke. 2000;31:2437–2449. 13. Miwa Y, Ozaki, Namiki MD, Hirase T, Inoue N, Hirata K, Yokoyama M. Kawashima S, Yamashita T. HMG-CoA reductase inhibitor has protective effects against stroke events in stroke-prone spontaneously hypertensive rats. Stroke. 2003;34:157–163. 14. Hanjani-Amin S, Stagliano NE, Yamada M, Huang PL, Liao JK, Moskowitz MA. Mevastatin, an HMG-CoA reductase inhibitor, reduces stroke damage and upregulates endothelial nitric oxide synthase in mice. Stroke. 2001;32:980 –986. 15. Endres M, Laufs U, Huang Z, Nakamura T, Huang P, Moskowitz MA, Liao JK. Stroke protection by 3-hydroxy-3-methylglutaryl (HMG)-CoA reductase inhibitors mediated by endothelial nitric oxide synthase. Proc Natl Acad Sci U S A. 1998;95:8880 – 8885. 16. Vaughan CJ, Delanty N. Neuroprotective properties of statins in cerebral ischemia and stroke. Stroke. 1999;30:1969 –1973. 17. Chen J, Zhang ZG, Li Y, Wang Y, Wang L, Jiang H, Zhang C, Lu M, Katakowski M, Feldkamp CS, Chopp M. Statins induce angiogenesis, neurogenesis, and synaptogenesis after stroke. Ann Neurol. 2003;53: 743–751. 18. Kobashigawa JA, Katznelson S, Laks H, Johnson JA, Yeatman L, Wang XM, Chia D, Terasaki PI, Sabad A, Cogert GA, Trosian K, 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. Effect of Atorvastatin on ICH 1749 Hamilton MA, Moriguchi JD, Kawata N, Hage A, Drinkwater DC, Stevenson LW. Effect of pravastatin on outcomes after cardiac transplantation. N Engl J Med. 1995;333:621– 627. Pahan K, Sheikh FG, Namboodiri AM, Singh I. Lovastatin and phenylacetate inhibit the induction of nitric oxide synthase and cytokines in rat primary astrocytes, microglia, and macrophages. J Clin Invest. 1997;100:2671–2679. Stanislaus R, Pahan K, Singh AK, Singh I. Amelioration of experimental allergic encephalomyelitis in Lewis rats by lovastatin. Neurosci Lett. 1999;269:71–74. Stanislaus R, Singh AK, Singh I. Lovastatin treatment decreases mononuclear cell infiltration into the CNS of Lewis rats with experimental allergic encephalomyelitis. J Neurosci Res. 2001;66:155–162. Stanislaus R, Gilg AG, Singh AK, Singh I. Immunomodulation of experimental autoimmune encephalomyelitis in the Lewis rats by Lovastatin. Neurosci Lett. 2002;333:167–170. Jeong SW, Chu K, Jung KH, Kim SU, Kim M, Roh JK. Human neural stem cell transplantation promotes functional recovery in rats with experimental intracerebral hemorrhage. Stroke. 2003;34:2258 –2263. Song EC, Chu K, Jeong SW, Jung KH, Kim SH, Yoon BW. Hyperglycemia exacerbates brain edema and perihematomal cell death after intracerebral hemorrhage. Stroke. 2003;34:2215–2220. Ohashi Y, Kawashima S, Hirata K, Yamashita T, Ishida T, Inoue N, Sakoda T, Kurihara H, Yazaki Y, Yokoyama M. Hypotension and reduced nitric oxide-elicited vasorelaxation in transgenic mice overexpressing endothelial nitric oxide synthase. J Clin Invest. 1998;102: 2061–2071. Chopp M, Li Y. Apoptosis in focal cerebral ischemia. Acta Neurochir. 1996;66:21–26. Matsushita K, Meng W, Wang X, Asahi M, Asahi K, Moskowitz MA, Lo EH. Evidence for apoptosis after intracerebral hemorrhage in rat striatum. J Cereb Blood Flow Metab. 2000;20:396 – 404. Nogawa S, Forster C, Zhang F, Nagayama M, Ross ME, Iadecola C. Interaction between inducible nitric oxide synthase and cyclooxygenase-2 after cerebral ischemia. Proc Natl Acad Sci U S A. 1998;95:10966–10971. Youssef S, Stuve O, Patarroyo JC, Ruiz PJ, Radosevich JL, Hur EM, Bravo M, Mitchell DJ, Sobel RA, Steinman L, Zamvil SS. The HMG-CoA reductase inhibitor, atorvastatin, promotes a Th2 bias and reverses paralysis in central nervous system autoimmune disease. Nature. 2002;420:78 – 84. Weitz-Schmidt G, Welzenbach K, Brinkmann V, Kamata T, Kallen J, Bruns C, Cottens S, Takada Y, Hommel U. Statins selectively inhibit leukocyte function antigen-1 by binding to a novel regulatory integrin site. Nat Med. 2001;7:687– 692. Romano M, Diomede L, Sironi M, Massimiliano L, Sottocorno M, Polentarutti N, Guglielmotti A, Albani D, Bruno A, Fruscella P, Salmona M, Vecchi A, Pinza M, Mantovani A. Inhibition of monocyte chemotactic protein-1 synthesis by statins. Lab Invest. 2000;80: 1095–1100. Huang KC, Chen CW, Chen JC, Lin WW. HMG-CoA reductase inhibitors inhibit inducible nitric oxide synthase gene expression in macrophages. J Biomed Sci. 2003;10:396 – 405. Downloaded from http://stroke.ahajournals.org/ by guest on February 23, 2013