Five valuable functions of blocking capacitors in stimulators
advertisement

Five valuable functions of blocking capacitors in stimulators
X. Liu1, A. Demostheous1, and N. Donaldson2
Department of Electronic and Electrical Engineering, University College London, UK
2
Department of Medical Physics and Bioengineering, University College London, UK
1
Abstract
Blocking capacitors, (known as coupling capacitors in some literatures), are extensively used in neural
stimulators. Usually, a blocking capacitor is connected in series with a stimulation electrodes and the other end
of the capacitor goes to the stimulation circuitry which supplies the current. Known for the “pass AC, block DC”
characteristic, blocking capacitors are important for safety in chronically implanted stimulators. They have five
functions: they help to correct charge imbalance; they prevent direct current passing under fault conditions; they
limit maximum net charge and charge per phase; they provide larger electromotive force for discharging and
therefore faster passive discharge; and finally they automatically adjust the resting potential of the electrode to
accommodate more charge injection. For high-intensity stimulation, the blocking capacitors are large in volume,
which means that designers would like to avoid their use for applications with many channels. Various
approaches have been proposed for their elimination, but some of them come at the expense of reduced safety.
The authors believe that the blocking capacitor should not be eliminated from the stimulator output stage design
unless the alternative passes a stringent safety analysis.
1
Introduction
Fig. 1 shows part of a subcutaneous stimulator: on a
substrate there is a thick-film circuit with an
integrated stimulator and 12 blocking capacitors. The
size of the blocking capacitor is decided by the
stimulation intensity. For example, to restore leg
movement, stimulus pulses up to 8 mA and 1 ms was
specified. According to
C=
It
,
V
(1)
4 μF blocking capacitors are required, in order to limit
the voltage drop across the capacitor to 2 V. Larger
voltage drop leads to smaller blocking capacitor, but
results in higher supply voltage and lower power
efficiency. There is an uncomfortable compromise
between inefficiency and size. Nevertheless blocking
capacitors remain popular because of the valuable
functions they perform. These are reviewed in the
next section.
2
Functions of blocking
capacitors
The functions of blocking capacitors in stimulators
ones are all related to safety.
A.
Help to correct charge imbalance
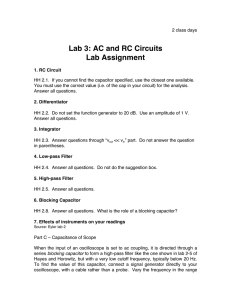
Fig. 2 shows three commonly used stimulator output
stage configurations, each employing a blockingcapacitor: (a) dual supplies with both active phases,
(b) single supply with both active phases, and (c)
single supply with active cathodic phase and passive
anodic phase. Both configurations in Figs 2(a) and
2(b) are (ideally) designed to be charge-balanced to
avoid charge accumulation. However, achieving
exactly zero net charge after each stimulation cycle is
not possible due to mismatch in the current source and
sink drivers for Fig. 2(a) or due to timing errors for
Fig. 2(b) or due to leakage from adjacent stimulus
sites for Fig. 2(a). The difference of cathodic charge
from the anodic charge, the net charge, is accumulated
stimulator circuitry
5cm
Pad
blocking capacitor
Figure 1 Part of a subcutaneous nerve root stimulator
made in a thick-film technology. There are 12 discrete
blocking capacitors in series with the outputs. The rest
of stimulator is integrated: the chip is under the black
silicone “glob-top”. Pads outside the seal rectangle are
for cable connections. Clearly the blocking capacitors
occupy much more space than the integrated circuit: a
disparity that would increase with more channels.
Figure 2 Conventional stimulator output stage configurations with blocking capacitor: (a) Dual supplies with
active cathodic and active anodic phases, (b) Singe supply with active cathodic and active anodic phases, (c)
Single supply with active cathodic phase and passive anodic phase.
on the blocking capacitor. By having an extra switch,
S3, to periodically discharge the capacitor-coupled
load passively in a third phase (after the cathodic
phase and the anodic phase), the charge imbalance is
corrected.
It is possible to use the voltage across the blocking
capacitor to drive the anodic current through the
electrode, in a passive anodic phase, as shown in Fig.
1(c). Passive discharge during the anodic phase can
also achieve good charge balance. The blocking
capacitor and the electrode-electrolyte impedance can
be lumped into a simple R-C model, giving a time
constant for discharge. Note, however, that it may not
be necessary to discharge for many time constants
because a non-zero mean voltage on the blocking
capacitor may be acceptable.
B.
Prevent prolonged DC current
Due to the “pass AC, block DC” characteristic of
capacitors, if connected in series with the stimulation
load, they prevent prolonged direct current passing
through the electrodes and tissue. Prolonged DC
might be caused by a software fault, semiconductor
failures, cable failures, etc [1]. In these situations,
low-leakage blocking capacitors are the last line of
defense against tissue damage.
C.
Limit maximum net charge and
charge per phase
It is not only direct current that may harm the
biological tissue. Even if the mean current is zero,
excessive charge density or charge per phase injected
to electrode-electrolyte interface will be dangerous
[2]. Each electrode material has a maximum charge
density which, if exceeded, will allow irreversible
reactions that generate toxic products. The maximum
charge per phase is the product of the maximum
charge density and the electrode surface area.
For a given power supply VDD, the worst-case charge
density that a blocking capacitor C would allow is
VDD·C/A, where A is the electrode area. If this is less
that the maximal allowable charge density for the
electrode material, the electrode can not be overcharged by the stimulator.
D.
Provide larger electromotive force
(emf) for discharging
After charging in the cathodic phase, the blocking
capacitor stores energy until the anodic phase. In a
passive anodic phase, voltage across the blocking
capacitor drives the discharge current and the energy
is released. For stimulation electrodes, no matter
whether they are capacitive, such as Tantalum, or
Faradaic, such as Platinum, the electrode itself has an
electrode-electrolyte interface capacitance. The
blocking capacitor is connected in series with this
electrode capacitance and the summed capacitance is
smaller than the electrode capacitance alone. Thus the
voltage across the summed capacitance will be higher
than the voltage across the electrode capacitance
alone, though the injected charge is the same with or
without a blocking capacitor.
At the beginning of the passive anodic phase, the
voltage across the summed capacitance is given by
Vstart =
I stim ⋅ tch arg e
C
(2)
where Istim is the stimulus current in the previous
cathodic phase, tcharge is the duration of the cathodic
phase and C is the summed capacitance if a blocking
capacitor is present or the electrode capacitance only
if the blocking capacitor is absent.
Due to the passive discharge in the anodic phase, for a
discharging time of tdischarge, the voltage across the
capacitor becomes
Vt = Vstart ⋅ e
−
t disch arg e
RC
(3)
The charge that has been neutralized in the time of
tdischarge is
Qneutralized = Qstart − Qt = C ⋅ (Vstart − Vt ) (4)
Substitute (2) and (3) into (4),
Qneutralized = I stim ⋅ tch arg e (1 − e
−
t disch arg e
RC
)
(5)
According to this equation, smaller capacitance will
result in more charge being neutralized (discharged)
within a given time.
Since a series-connected
blocking capacitor results in a smaller summed
capacitance than the electrode capacitance alone, the
presence of a blocking capacitor provides larger
electromotive force to discharge the load.
E.
4
Adjust the resting potential of the
electrode to accommodate more
charge injection
The amount of charge which a stimulation electrode
can safely inject is limited by the breakdown voltage
of electrode-electrolyte interface. The voltage at
stimulation electrode can be measured by referring to
a reference electrode.
If Ф is the potential of the stimulation electrode with
respect to a reference electrode in the same
electrolyte, Фmax is the most positive allowable value
of Ф, Фmin is the most negative allowable value. Фmin
~ Фmax defines the water window of the chosen
electrode which, if exceeded, will cause gassing to
occur. For Platinum, Фmax is 1200 mV RHE and Фmin
is -800 mV RHE [3].
If Ф1 is the electrode potential before the beginning of
a pulse, Ce is the interface capacitance at the interface,
and Q is the injectable charge, then for stimulation
anode and cathode, respectively,
Qanodic _ max = ∫
φmax
φ1
Qcathodic _ max = − ∫
Ce dφ
φ1
φmin
Ce dφ
direction as to bias the electrode positively. New Ф1
“slides back” [3] from previous Ф1 to some more
positive Фs. Hydrogen evolution now ceases, and the
electrode works over the new, greater potential range
Фs - Фmin which allows higher charge injection while
still maintain safety at electrode-electrolyte interface.
If one continues to raise the charge per pulse, Фs
eventually reaches Фmax, no further “slide back” is
possible, and the electrode begins to evolve both
oxygen and hydrogen. Similar mechanism, known as
“slide forward” applies to the capacitor-coupled
anode. Thus the blocking capacitor can actively “slide
back” and “slide forward” the resting potential of the
electrode in order to accommodate more charge
injection.
Conclusions
In this paper, we present five important functions of
blocking capacitors in neural stimulators. Some or all
of these functions may be important in ensuring safety
for devices that must be safe for years of use in the
body. In some applications, especially those with
many electrodes, the size of blocking capacitors can
be disadvantageous or actually prohibitive. Designers
who wish to avoid blocking capacitors should bear in
mind what functions will be lost and analyse their
alternative solutions thoroughly to ensure that safety
is maintained. Designs with blocking capacitors are
relatively simple because of their unique safety
functions.
Acknowledgement
We would like to thank EPSRC with Grant
EP/F009593/1 and European Commission under
project IMANE for the financial assistance.
(6)
References
(7)
[1] X. Liu, A. Demosthenous, and N. Donaldson,
"Implantable Stimulator Failures: Causes,
Outcomes, and Solutions," in Proc. 29th Ann. Int.
Conf. IEEE Engineering in Medicine and
Biology Society, pp. 5786-5789, 2007.
[2] D. B. McCreery, W. F. Agnew, T. G. H. Yuen,
and L. Bullara, "Charge density and charge per
phase as cofactors in neural injury induced by
electrical stimulation," IEEE Trans. Biomed.
Eng., vol. 37, no. 10, pp. 996-1001, 1990.
[3] N. D. N. Donaldson and P. E. K. Donaldson,
"When are actively balanced biphasic ('Lilly')
stimulating pulses necessary in a neurological
prosthesis? I Historical background; Pt resting
potential; Q studies.," Med. Biol. Eng. Comput.,
vol. 24, no. 1, pp. 41-49, 1986.
It has been found that there are many influences on
the resting potential of the electrode, such as
dissolved gas, pH value, etc. A variation of the
environment will results the resting potential drift to a
new value which increases or reduces the maximum
allowable charge in a single phase.
When a capacitor-coupled Platinum cathode is used to
inject negative-going stimulating pulses, the potential
range available in delivering the first pulse is Ф1 Фmin. If the charge per pulse which produces this
potential change is exceeded and Ф taken below Фmin,
the electrode will evolve a little hydrogen at the peak
of each negative excursion. The net transfer of charge
corresponding to this hydrogen will alter the mean
voltage across the serial blocking capacitor in such a