Comparison of external radiation therapy vs radical
advertisement

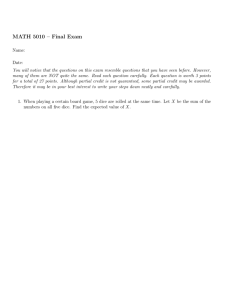
Prostate Cancer and Prostatic Diseases (2004) 7, 343–349 & 2004 Nature Publishing Group All rights reserved 1365-7852/04 $30.00 www.nature.com/pcan Comparison of external radiation therapy vs radical prostatectomy in lymph node positive prostate cancer patients R Kuefer1, BG Volkmer1, M Loeffler1, RL Shen2, L Kempf3, AS Merseburger4, JE Gschwend1, RE Hautmann1, HM Sandler3,6 & MA Rubin5,6* 1 Department of Urology, University of Ulm, Ulm, Germany; 2Department of Pathology, University of Michigan, School of Medicine, Ann Arbor, Michigan, USA; 3Department of Radio-Oncology, University of Michigan, School of Medicine, Ann Arbor, Michigan, USA; 4Department of Urology, University of Tuebingen, Tuebingen, Germany; and 5 Department of Pathology, Brigham & Women’s Hospital, Boston, Massachusetts, USA Introduction: Treatment options for lymph node positive prostate cancer are limited. We retrospectively compared patients who underwent external radiotherapy (ERT) to patients treated by radical prostatectomy (RPX). Materials and Methods: A total of 102 lymph node positive patients from the RPX series at Ulm University were evaluated. In all, 76 patients received adjuvant androgen withdrawal as part of their primary treatment. In the ERT group, 44 patients were treated at the University of Michigan using a fractionated regimen. Of these, 21 patients received early adjuvant hormonal therapy. Patients with neoadjuvant therapy before RPX or ERT were excluded. Results: In the RPX group, PSA nadir (nadirp0.2 vs 40.2 ng/ml) showed a strong association with outcome. In the ERT group, pretreatment PSA was an independent predictor of outcome (P ¼ 0.04) and patients with adjuvant hormonal therapy had a significant longer recurrence-free interval compared to patients without adjuvant therapy (P ¼ 0.004). Comparing only patients with adjuvant hormonal treatment after cancer-specific therapy, the ERT-treated patients had a borderline longer PSA recurrence-free survival time compared to the RPX-treated patients (P ¼ 0.05). Conclusions: In case of positive lymph nodes, RPX and ERT might be considered and need to be explained to the patient. For future treatment decisions, the presented findings and a potential survival benefit need to be evaluated in a larger prospective setting. Prostate Cancer and Prostatic Diseases (2004) 7, 343–349. doi:10.1038/sj.pcan.4500751 Published online 7 September 2004 Keywords: external beam radiation therapy; radical prostatectomy; lymph node positive; outcome Introduction Prostate cancer is a leading cause of male cancer-related deaths in the United States.1 Currently, there is no *Correspondence: MA Rubin, Pathology, Brigham & Women’s Hospital, 75 Francis Street, Boston, MA 02115, USA. E-mail: marubin@partners.org 6 These authors contributed equally to this work. Received 7 April 2004; revised 26 May 2004; accepted 21 June 2004; published online 7 September 2004 standard approach for treating clinically confined and locally advanced prostate cancer. Patients and clinicians deliberate between radical prostatectomy, radiation therapy, and watchful waiting. One recent study provides evidence that men with clinically localized prostate cancer may benefit from radical prostatectomy when compared to watchful waiting due to reduced cancerspecific death and development of metastatic disease in the surgical cohort.2 For men with locally advanced prostate cancer disease (ie, localized prostate cancer with Radiation or surgery in advanced prostate cancer R Kuefer et al 344 spread to pelvic or regional lymph nodes but no evidence of distant metastatic disease), one may anticipate that treatment decision is easier as it is documented that patients receiving no therapy at all will have a very poor prognosis.3–5 Yet, only limited comparative data are available concerning different therapeutic options.6 The goal of the current study was to compare external radiation therapy (ERT) and radical prostatectomy (RPX) in the setting of locally advanced prostate cancer using biochemical failure as the endpoint. Material and methods Patient population At the University of Ulm, Germany, more than 1400 patients underwent RPX since 1984. A total of 177 patients had RPX despite the identification of metastatic disease to pelvic lymph nodes during the course of surgery or metastatic spread was identified on the final review of pathology following surgery. Extended lymphadenectomy was carried out and all cases were staged using the TNM classification.7 Histopathology was re-evaluated by the study pathologist (MAR), who assigned a Gleason score.8 Patients were grouped according to PSA nadir with a cutoff at 0.2 ng/ ml, those with a PSA o0.2 ng/ml were considered as cases with best local control of tumor. Progression was defined as either an elevation of the PSA level (increase of 40.2 ng/ml compared to PSA nadir) or clinical detectable progress. Follow-up was carried out according to a standardized protocol (physical examination and PSA every 3 months for 2 y after RPX, then twice a year; chest X-ray and bone scan once a year or if suspected). Patients who had received neoadjuvant treatment were excluded. There were 102 men treated by RPX, who fell in this group. At the University of Michigan, USA, 62 patients received ERT for lymph node positive prostate cancer between 1986 and 2001. For analysis, the following clinical parameters were required: clinical TNM classification, biopsy Gleason score, pretreatment PSA levels, type of adjuvant therapy, treatment duration and total dose of radiation, and standardized follow-up including evaluation of post-treatment PSA levels. In 45 patients (72.6%), attempted radical prostatectomy was abrogated due to histologically confirmed lymph node metastases. The other 27.4% were diagnosed by enlarged lymph nodes without resection, potentially resulting in a higher tumor burden at time of referral to treatment. ERT was carried out using a fractionated, 3D conformal regimen with an average total dose of 69 Gy (range 45–77 Gy) applied onto the prostate within 54 days (range 32–76 days). Failure was defined according to the ASTRO criteria as three consecutive PSA rises compared to nadir.9 The study population of the ERT group consisted of 44 cases. Detailed demographics are given in Table 1. Table 1 Demographics of the two treatment modalities: radical prostatectomy (RPE) and external radiation therapy (EBRT) Radical prostatectomy Patient cohort Radiation dose (Gy) Radiation duration (days) Clinical T1 Clinical T2 Clinical T3 Clinical T4 T stage not assigned 3 (6.8) Pathological T1 Pathological T2 Pathological T3 Pathological T4 N1 N2 PSA median (ng/ml) Gleason sum 6 7 8 9 10 Gleason score not assigned PSA nadir median (ng/ml) PSA nadir o0.2 PSA nadir X0.2 Adjuvant treatment Hormonal monotherapy Complete suppression Follow-up median (y) Biochemical failure Time till failure median (y) 102 (100%) 2 (2%) 47 (46%) 51 (50%) 2 (2%) 0 (0%) 5 (5%) 90 (88%) 7 (7%) 65 (64%) 37 (36%) 26.1 (3.5–414 range) RPE specimen 4 (4%) 24 (24%) 54 (53%) 18 (18%) 2 (2%) 0.0 64 38 76 54 22 1.9 60 0.6 N1 ¼ one affected lymph node; N2 ¼ two or more positive lymph nodes. Prostate Cancer and Prostatic Diseases (0.0–3.1 range) (62.7%) (37.3%) (75%) (53%) (22%) (0.1–12.4 range) (59%) (0.1–10.7 range) Radiation therapy 44 (100%) Mean 69 (45–77 range) Mean 54 (32–76 range) 2 (5%) 18 (41%) 17 (39%) 4 (9%) 23 (52%) 21 (48%) 19.9 (2.9–3100 range) Biopsy 5 (11%) 19 (43%) 9 (21%) 2 (5%) 0 (0%) 9 (21%) 0.1 (0.0–6.6 range) 21 9 12 2.1 27 1.5 (48%) (21%) (27%) (0.5–14.1 range) (61%) (0.5–7.5 range) Radiation or surgery in advanced prostate cancer R Kuefer et al Data analysis Statistical analysis was performed by a bio-statistician (RLS) applying standard approaches such as the T-test to test for significant difference between the study populations and the Kaplan–Meier analysis to estimate survival. Univariate, unmatched comparisons of survival were performed using the log rank test. The Wald test was used for Cox hazards regression analysis in a multivariate model. Results Analysis of the RPX study population All 102 patients of the RPX group underwent surgery with the intention of a surgical cure. The majority of cases had microscopic proven metastases identified in the review of the permanent pathology sections after surgery. Average age at surgery was 64.7 y (range 49.3– 79.1 y). The median PSA level before surgery was 26.1 ng/ml (range 3.5–414 ng/ml). Two (2%) cases were classified as clinical T1 tumors, 47 (46%) cases as T2, 51 (50%) as T3 and two (2%) cases as clinical T4 tumors. Pathologic evaluation demonstrated that tumor classification was underestimated by the clinical T stage as most of the cases proved to be in the pathology report pT3 (90 patients; 88%). Only five (5%) patients were pT2 and seven (7%) cases T4. In all, 64% of the patients had one positive lymph node after final review of the pathology. All tumors were Gleason score X6. In 64 (62.7%) patients, PSA after surgery dropped o0.2ng/ml, in 38 (37.3%) patients nadir was X0.2 ng/ml. A total of 76 (74.5%) patients received early adjuvant hormonal treatment, 54 patients as monotherapy and 22 patients complete androgen withdrawal. Mean time of follow-up was 2.9 y (range 0.1–12.4 y; 40 (39%) follow-up 43 y). Of the 102 patients, 60 experienced biochemical failure. Median time till failure was 0.6 y (mean 1.5 y; range 0.1–10.7 y). All patients experiencing local or distant recurrence had prior biochemical relapse. Detailed clinical data are given in Table 1 and a graphical presentation of the PSA recurrence-free survival of the 102 RPX cases is given in Figure 1a. To test for associations between clinical parameters and outcome in the RPX group, univariate Cox regression analyses were performed. None of the clinical parameters including age at diagnosis, clinical or pathological tumor stage, lymph node burden, Gleason sum, WHO tumor grade of the prostatectomy specimen, preoperative PSA (numeric value, categorized or logarithmic value) or type of adjuvant hormone treatment demonstrated a statistically significant association with outcome defined as biochemical failure. The only parameter with significant association with outcome was PSA nadir following surgery (Po0.0001, 95% confidence interval (CI) 1.7–4.9) (Figure 1b). The best multivariate model for the RPX group eliminated in a stepwise backward procedure all of the clinical parameters mentioned above, calculating a P-value of o0.0001 for PSA nadir (CI 1.7–5.0; hazard risk 2.9). There was no statistically significant difference in recurrence-free survival time based on type of adjuvant treatment (log rank P ¼ 0.46). Only if stratified for PSA nadir, those patients reaching a nadir of PSAo0.2 ng/ml and receiving complete hormonal withdrawal had a longer time of recurrence-free survival compared to those patients receiving mono-therapy (log rank P ¼ 0.03). In the group of patients with a nadir PSAX0.2 ng/ml, there was no association between type of treatment and recurrence-free survival (log rank P ¼ 0.3). 345 Analysis of the ERT study population Since 1986, 44 patients were treated by ERT for lymph node positive prostate cancer at the University of Michigan. Median PSA level before radiotherapy was 19.9 ng/ml (range 2.9–3100 ng/ml). Two (4.5%) patients had clinical stage T1, 18 (40.9%) patients T2, 17 (38.6%) T3 and four (9.1%) patients T4. Three (6.8%) patients were not assigned a clinical T stage. In all, 52.3% of the patients had one positive lymph node. Five (11.4%) cases had a Gleason sum of 6. A total of 30 (68.2%) patients had a Gleason score of X7 (Gleason ¼ 7, 43.2%; Gleason ¼ 8, Figure 1 (a) Kaplan–Meier analysis showing the recurrence-free survival for the group of patients with lymph node positive disease treated by radical prostatectomy. (b) Patients treated by prostatectomy stratified for postoperative prostate-specific antigen nadir o0.2 ng/ml vs X0.2 ng/ml (log rank Po0.0001). Prostate Cancer and Prostatic Diseases Radiation or surgery in advanced prostate cancer R Kuefer et al 346 20.5%; Gleason ¼ 9, 4.5%). For nine biopsies, a Gleason score was not available for analysis. Median nadir was a PSA of 0.1 ng/ml (0.0–8.8 ng/ml). In all, 21 (47.8%) patients received adjuvant treatment, nine (20.5%) patients monotherapy and 12 (27.3%) patients complete androgen deprivation. Median follow-up time was 2.1 y (range 0.5–14.1 y; mean 3.2 y; 15 (34%) follow-up 43 y). Of the 44 patients, 27 (61.4%) had biochemical failure. Median time to failure was 1.5 y (range 0.5–7.5 y). A graphical presentation of the recurrence-free survival data of the 44 ERT treated cases is given in Figure 2a. Of all clinical parameters, tumor stage (Cox regression P ¼ 0.005, CI 1.4–7.4) and pretreatment PSA (P ¼ 0.007, CI 95% 1.3–4.3) had a strong association with outcome on the univariate level. In the ERT group, there is a significant higher percentage of patients with freedom from recurrence if adjuvantly treated by any type of early hormonal withdrawal (P ¼ 0.004) (Figure 2b). There was statistically no difference if treated with monotherapy or complete hormonal withdrawal (log rank P ¼ 0.38). The multivariate model calculated a P-value of 0.001 for pretreatment PSA if categorized into three groups PSAo10 ng/ml, PSA410 and o20 ng/ml and PSA420 ng/ml (CI 2.2–19.6). In this setting, adjuvant hormonal therapy had the strongest association with PSA recurrence-free survival in patients treated with ERT (Po0.001; CI 0.01–0.2). Comparison of the two treatment modalities: RPX and ERT For comparison of the two treatment options, we first looked at patients who had received some kind of adjuvant hormonal therapy. With this approach, it is taken into consideration that adjuvant treatment had a significant influence on outcome in the ERT group. In the RPX group, independent of nadir, there was no strong association between type of adjuvant hormone therapy and outcome as described above. The RPX group consisted of 76 patients. In all, 45 patients experienced biochemical failure during follow-up; median follow-up was 1.6 y (mean 3.1 y; range 0.1–12.4 y). The ERT group consisted of 21 cases of which seven had PSA relapse during follow-up; median follow-up was 2.3 y (mean 3.3 y; range 0.5–10.6 y). There was no significant difference in the pretreatment clinical parameters between these two groups including tumor stage (T-test P ¼ 0.6), lymph node burden (P ¼ 0.7) and PSA (P ¼ 0.06). As demonstrated in Figure 3a, the Kaplan–Meier survival curve revealed a borderline significant difference in PSA recurrence-free survival rate between these two groups (log rank P ¼ 0.053). Interestingly, the ERT group reached a plateau at about 50% PSA recurrencefree survival, starting at a follow-up time of 4 y. In contrast to that, in the RPX group, the survival curve of the patients receiving some sort of adjuvant hormonal therapy, does not reach a plateau up to 12 y after RPX. Complete hormonal withdrawal has, in both treatment groups, some, but not a statistically significant, benefit compared to monotherapy (RPX log rank P ¼ 0.36; ERT log rank P ¼ 0.38). As demonstrated in Figure 3b, when comparing only patients with complete hormonal withdrawal after cancer-specific therapy, there is no difference in PSA recurrence-free survival between the RPX and the ERT group (log rank P ¼ 0.37). In this comparison, all patients independent of nadir were included in the RPX group, as postsurgical nadir cannot be used as a parameter to preselect patients for RPX. Discussion Currently for men diagnosed with clinically localized and locally advanced prostate cancer, there is no definitive single ‘best’ treatment option. Some guidelines have been developed to evaluate men on watchful waiting protocols.10 A recent study provides evidence that in clinically localized prostate cancer, radical prostatectomy may reduce the cancer-specific but not the overall mortality compared to watchful waiting.2 At first glance, the debate regarding treatment seems easier in locally advanced disease, as it is known that patients with node positive disease, receiving no therapy will die due to prostate cancer within a short period of time.11 But in these cases, the question is what type of therapy is of most long-term benefit to the majority of patients? Figure 2 (a) Kaplan–Meier analysis showing the recurrence-free survival for the group of patients with lymph node positive disease treated by ERT. (b) Freedom from recurrence of patients after radiation stratified for type of adjuvant hormonal treatment. Patients receiving no adjuvant hormonal therapy vs patients with adjuvant androgen withdrawal (log rank P ¼ 0.014). Prostate Cancer and Prostatic Diseases Radiation or surgery in advanced prostate cancer R Kuefer et al 347 Figure 3 (a) Kaplan–Meier analysis comparing the recurrence-free survival of patients treated by radical prostatectomy vs patients who underwent external radiation therapy. Both groups received adjuvant hormonal treatment either by monotherapy or complete hormonal withdrawal (log rank P ¼ 0.05). (b) Comparison of the recurrence-free survival of patients who received complete hormonal withdrawal after radical prostatectomy or ERT. Radiation therapy as an option in the treatment for prostate cancer goes back to the 1960 s. Technical advances and application of field techniques have helped reduce complications and only in the minority of cases do patients report moderate urinary and bowel symptoms.12,13 In prostate cancer, the gross disease requires radiation doses of at least 70 Gy applied in a fractionated regimen. The median dose in this study was 69 Gy and thus is quite low. Such low doses are likely suboptimal for treatment. In fact, there is evidence that increased doses are associated with reduced risk of biochemical failure, distant metastasis and even overall survival.14–16 Controversy exists if there is a benefit to irradiation of the pelvic lymph nodes with a total dose of about 45 Gy. A study conducted by the RTOG failed to show a benefit in treating lymph nodes and prostate compared to prostate alone in prostate cancer A2 and B tumors.17 This observation is supported by another study including lymph node positive prostate cancer patients.18 No clear benefit is described in the literature from prophylactic pelvic nodal irradiation compared to prostate-only radiation. Yet, according to the RTOG 9413 study, there is a benefit of whole pelvic radiotherapy if combined with neoadjuvant and concurrent hormonal therapy compared to radiotherapy of the prostate-only with any type of hormonal withdrawal.19 Radical prostatectomy combined with adjuvant hormonal therapy is considered a valuable treatment option in high-risk prostate cancer patients.20 In the presence of positive lymph nodes, it has been demonstrated that immediate antiandrogen therapy reduces the risk of recurrence and improves survival compared to observation.21 Surgery often is stopped once positive lymph nodes are discovered during lymphadenectomy. Still some benefit through surgery and adjuvant hormonal treatment in these advanced cases is reported.5,11,22 In fact, there is evidence that radical prostatectomy with early adjuvant androgen deprivation provides a significant advantage compared to androgen suppression alone as goes for overall and disease-specific survival.23 Presently, less advanced cases are diagnosed due to increasing awareness of the population and the merit of PSA as a screening tool. On the other hand, a recent series from Europe shows minute lymph node metas- tases in about 40% of all cases including cases with a low pathological tumor stage. In this study, examination of iliac lymph nodes from the external and internal region was examined.24 These findings suggest that at least some published outcome results after RPX had a significant number of cases with lymph node positive disease, included as pN0 disease. A critical issue in comparing the results of two treatment modalities in this or any study is the choice of exclusion criteria and the definition of outcome. In this study, all patients with any kind of neoadjuvant treatment have been excluded. For patients treated with RPX, neoadjuvant hormonal therapy is still considered controversial and not generally recommended.25,26 For patients treated with ERT, neoadjuvant therapy is promising to have an influence even on disease-free and overall survival.27 Adjuvant treatment has been grouped the RPX and the ERT patients into three categories, no adjuvant treatment, monotherapy and complete androgen deprivation. Although it has been suggested in previous studies that early adjuvant androgen deprivation is beneficial for patients with node positive disease treated by RPX,21,28,29 surprisingly a considerable number of patients did not receive adjuvant hormonal therapy. The same is true for the ERT group. In accordance with the findings in this study and supported by in vitro and in vivo experiments,30 early adjuvant hormonal treatment has been shown to be beneficial in bulky tumors.31–34 Crucial for comparison of the results is the choice of endpoint. In the current series, there have not been enough disease-specific deaths, that is, three in the ERT group, for comparative statistical analysis. This points out the importance of even longer follow-up times. The endpoint was defined as biochemical failure measured by PSA. For all interpretations in this setting, it has to be kept in mind that the most common, but still different definitions of failure, have been applied for the two treatment options. It cannot be ruled out that the differences seen might be only related to the calculation of PSA failure or the expected kinetics after specific therapy. For radiation therapy, there is significant controversy about definition of the appropriate nadir. It is known that after radiation therapy, PSA levels decline Prostate Cancer and Prostatic Diseases Radiation or surgery in advanced prostate cancer R Kuefer et al 348 over a period of several years. It is unclear if the time till nadir is associated with risk of biochemical failure but, in one study, it was demonstrated that a nadir of less than 1 ng/ml is an independent predictor of biochemical outcome.35 In the current study, we applied to the ERT group the ASTRO criteria,9 although variations in results due to different criteria and potential improvements of the ASTRO criteria have been described.36,37 For the RPX group, biochemical failure was defined as a PSA increase over 0.2 ng/ml compared to nadir. For comparison with the ERT group, those patients not reaching undetectable PSA levels after RPX were not excluded, although these cases obviously represent unsatisfactory surgical control and might be defined as failures at day zero in other studies. So not surprisingly, there was a strong association between nadir and biochemical failure in the RPX group. This is a post-treatment parameter and thus cannot be taken into consideration for treatment decision. Analysis of the RPX group demonstrated that an optimal surgical result is mandatory for an additional significant positive effect of adjuvant hormonal deprivation. As described in detail above, patients treated by ERT and adjuvant hormonal therapy had statistically a borderline significant better outcome than patients after RPX and adjuvant hormonal therapy. This difference diminishes if best surgical condition was achieved reflected by a PSA nadir of o0.2 ng/ml. In this case, patients treated by RPX and receiving some adjuvant hormonal treatment do as well as patients treated by ERT and adjuvant hormonal treatment (log rank 0.47). Obviously, there is no possibility to predict a PSA nadir of o0.2 ng/ml after RPX. Therefore, we believe that the rationale for the comparison between these two treatment groups of men with locally advanced prostate cancer is appropriate. On the other hand, analysis demonstrated that a patient reaching a PSA nadir of o0.2 ng/ml and receiving complete hormonal withdrawal has almost a 80% chance not to experience biochemical failure within 10 y after surgery (data not shown). Furthermore, one may state that patients treated by RPX and not reaching a PSA nadir of o0.2 ng/ml will need some other sort of adjuvant therapy as hormonal withdrawal does not seem to have a major influence. In this group, ERT might be a very good option of adjuvant treatment after RPX.38 Our data also suggest that in patients treated with ERT, adjuvant therapy by the means of hormonal withdrawal, is beneficial. The different mechanisms represented by radiotherapy and hormonal deprivation concerning control or killing of malignant cells suggest a rationale for their combined use. In the RPX group, it is demonstrated that long-term success primarily depends on a perfect local control and thus surgical success. In this setting, hormonal therapy shows an additive effect on PSA recurrence-free survival. Conclusions Acknowledging the fact that morbidity and mortality of both treatment options, RPX and ERT, have been significantly decreasing due to technical improvements, both therapy modalities have to be considered and explained to the patient in case of positive lymph nodes. Prostate Cancer and Prostatic Diseases If a PSA nadir of o0.2 ng/ml is not reached after RPX, additional therapy (ie ERT) is indicated as hormonal withdrawal is not sufficient. Acknowledgements This study was supported by the Specialized Program of Research Excellence for Prostate Cancer (S.P.O.R.E.) NCI Grant no. P50CA69568. References 1 Jemal A et al. Cancer statistics, 2002. CA Cancer J Clin 2002; 52: 23–47. 2 Holmberg L et al. A randomized trial comparing radical prostatectomy with watchful waiting in early prostate cancer. N Engl J Med 2002; 347: 781–789. 3 Davidson PJ et al. Progression in untreated carcinoma of the prostate metastatic to regional lymph nodes (stage t0 to 4,N1 to 3.M0,D1). European Organization for Research and Treatment of Cancer Genitourinary Group. J Urol 1995; 154: 2118–2122. 4 Seay TM, Blute ML, Zincke H. Long-term outcome in patients with pTxN+adenocarcinoma of prostate treated with radical prostatectomy and early androgen ablation. J Urol 1998; 159: 357–364. 5 Zwergel U et al. Lymph node positive prostate cancer: long-term survival data after radical prostatectomy. J Urol 2004; 171: 1128–1131. 6 Pollack A, Horwitz EM, Movsas B. Treatment of prostate cancer with regional lymph node (N1) metastasis. Semin Radiat Oncol 2003; 13: 121–129. 7 Fleming ID, Cancer AJCo, (U.S.) NCI. AJCC Cancer Staging Manual, 5th ed., Philadelphia: Lippincott-Raven, 1997. 8 Gleason DF. Classification of prostatic carcinomas. Cancer Chemother Rep 1966; 50: 125–128. 9 American Society for Therapeutic Radiology aOCP. Consensus Statement: Guidlines for PSA following radiation therapy. Int J Radiat Oncol Biol Phys 1997; 37: 1035–1041. 10 Choo R et al. Feasibility study: watchful waiting for localized low to intermediate grade prostate carcinoma with selective delayed intervention based on prostate specific antigen, histological and/or clinical progression. J Urol 2002; 167: 1664–1669. 11 Seay TM, Blute MC, Zincke H. Radical prostatectomy and early adjuvant hormonal therapy for pTxN+ adenocarcinoma of the prostate. Urology 1997; 50: 833–837. 12 Sandler HM et al. Three dimensional conformal radiotherapy for the treatment of prostate cancer: low risk of chronic rectal morbidity observed in a large series of patients. Int J Radiat Oncol Biol Phys 1995; 33: 797–801. 13 Fukunaga-Johnson N et al. Results of 3D conformal radiotherapy in the treatment of localized prostate cancer. Int J Radiat Oncol Biol Phys 1997; 38: 311–317. 14 Michalski JM et al. Preliminary report of toxicity following 3D radiation therapy for prostate cancer on 3DOG/RTOG 9406. Int J Radiat Oncol Biol Phys 2000; 46: 391–402. 15 Ryu JK et al. Interim report of toxicity from 3D conformal radiation therapy (3D-CRT) for prostate cancer on 3DOG/RTOG 9406, level III (79.2 gy). Int J Radiat Oncol Biol Phys 2002; 54: 1036–1046. 16 Jacob R et al. The relationship of increasing radiotherapy dose to reduced distant metastases and mortality in men with prostate cancer. Cancer 2004; 100: 538–543. 17 Asbell SO et al. Elective pelvic irradiation in stage A2, B carcinoma of the prostate: analysis of RTOG 77-06. Int J Radiat Oncol Biol Phys 1988; 15: 1307–1316. 18 Leibel SA et al. The effects of local and regional treatment on the metastatic outcome in prostatic carcinoma with pelvic Radiation or surgery in advanced prostate cancer R Kuefer et al 19 20 21 22 23 24 25 26 27 28 lymph node involvement. Int J Radiat Oncol Biol Phys 1994; 28: 7–16. Roach III M et al. Phase III trial comparing whole-pelvic vs prostate-only radiotherapy and neoadjuvant vs adjuvant combined androgen suppression: Radiation Therapy Oncology Group 9413. J Clin Oncol 2003; 21: 1904–1911. Vaishampayan U, Hussain M. The evolving role of systemic therapy in high risk prostate cancer: strategies for cure in the 21st century. Crit Rev Oncol Hematol 2002; 42: 179–188. Messing EM et al. Immediate hormonal therapy compared with observation after radical prostatectomy and pelvic lymphadenectomy in men with node-positive prostate cancer. N Engl J Med 1999; 341: 1781–1788. Samson D-J et al. Systematic review and meta-analysis of monotherapy compared with combined androgen blockade for patients with advanced prostate carcinoma. Cancer 2002; 95: 361–376. Ghavamian R et al. Radical retropubic prostatectomy plus orchiectomy vs orchiectomy alone for pTxN+prostate cancer: a matched comparison. J Urol 1999; 161: 1223–1227, discussion 1227–1228. Heidenreich A, Varga Z, Von-Knobloch R. Extended pelvic lymphadenectomy in patients undergoing radical prostatectomy: high incidence of lymph node metastasis. J Urol 2002; 167: 1681–1686. Wieder JA, Soloway MS. Incidence, etiology, location, prevention and treatment of positive surgical margins after radical prostatectomy for prostate cancer. J Urol 1998; 160: 299–315. Gleave ME et al. Long-term neoadjuvant hormone therapy prior to radical prostatectomy: evaluation of risk for biochemical recurrence at 5-year follow-up. Urology 2000; 56: 289–294. Bolla M et al. Improved survival in patients with locally advanced prostate cancer treated with radiotherapy and goserelin. N Engl J Med 1997; 337: 295–300. Zincke H et al. Stage D1 prostate cancer treated by radical prostatectomy and adjuvant hormonal treatment. Evidence for 29 30 31 32 33 34 35 36 37 38 favorable survival in patients with DNA diploid tumors. Cancer 1992; 70 (1 Suppl): 311–323. Frohmuller HG et al. Survival and quality of life of patients with stage D1 (T1-3 pN1-2 M0) prostate cancer. Radical prostatectomy plus androgen deprivation vs androgen deprivation alone. Eur Urol 1995; 27: 202–206. Zietman AL et al. The effect of androgen deprivation and radiation therapy on an androgen-sensitive murine tumor: an in vitro and in vivo study. Cancer J Sci Am 1997; 3: 31–36. Pilepich MV et al. Phase III radiation therapy oncology group (RTOG) trial 86-10 of androgen deprivation adjuvant to definitive radiotherapy in locally advanced carcinoma of the prostate. Int J Radiat Oncol Biol Phys 2001; 50: 1243–1252. Whittington R et al. The use of combined radiation therapy and hormonal therapy in the management of lymph nodepositive prostate cancer. Int J Radiat Oncol Biol Phys 1997; 39: 673–680. Sands ME, Pollack A, Zagars GK. Influence of radiotherapy on node-positive prostate cancer treated with androgen ablation. Int J Radiat Oncol Biol Phys 1995; 31: 13–19. Zagars GK, Pollack A, von-Eschenbach AC. Addition of radiation therapy to androgen ablation improves outcome for subclinically node-positive prostate cancer. Urology 2001; 58: 233–239. Zelefsky MJ et al. Significance of normal serum prostate-specific antigen in the follow-up period after definitive radiation therapy for prostatic cancer. J Clin Oncol 1995; 13: 459–463. Cherullo EE et al. Variable definitions influence the reporting of biochemical failure rates. Prostate Cancer and Prostatic Disease 2002; 5: 54–58. Taylor JM, Griffith KA, Sandler HM. Definitions of biochemical failure in prostate cancer following radiation therapy. Int J Radiat Oncol Biol Phys 2001; 50: 1212–1219. Kalapurakal JA et al. Biochemical disease-free survival following adjuvant and salvage irradiation after radical prostatectomy. Int J Radiat Oncol Biol Phys 2002; 54: 1047–1054. 349 Prostate Cancer and Prostatic Diseases