A comparison between amplitude sorting and phase
advertisement

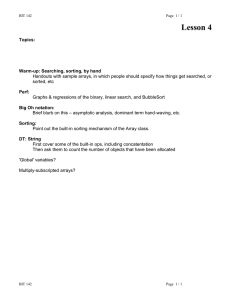
A comparison between amplitude sorting and phase-angle sorting using external respiratory measurement for 4D CT Wei Lu, Parag J. Parikh, James P. Hubenschmidt, Jeffrey D. Bradley, and Daniel A. Lowa兲 Department of Radiation Oncology, Washington University School of Medicine, St. Louis, Missouri 63110 共Received 19 September 2005; revised 21 May 2006; accepted for publication 13 June 2006; published 27 July 2006兲 Respiratory motion can cause significant dose delivery errors in conformal radiation therapy for thoracic and upper abdominal tumors. Four-dimensional computed tomography 共4D CT兲 has been proposed to provide the image data necessary to model tumor motion and consequently reduce these errors. The purpose of this work was to compare 4D CT reconstruction methods using amplitude sorting and phase angle sorting. A 16-slice CT scanner was operated in ciné mode to acquire 25 scans consecutively at each couch position through the thorax. The patient underwent synchronized external respiratory measurements. The scans were sorted into 12 phases based, respectively, on the amplitude and direction 共inhalation or exhalation兲 or on the phase angle 共0 – 360° 兲 of the external respiratory signal. With the assumption that lung motion is largely proportional to the measured respiratory amplitude, the variation in amplitude corresponds to the variation in motion for each phase. A smaller variation in amplitude would associate with an improved reconstructed image. Air content, defined as the amount of air within the lungs, bronchi, and trachea in a 16-slice CT segment and used by our group as a surrogate for internal motion, was correlated to the respiratory amplitude and phase angle throughout the lungs. For the 35 patients who underwent quiet breathing, images 共similar to those used for treatment planning兲 and animations 共used to display respiratory motion兲 generated using amplitude sorting displayed fewer reconstruction artifacts than those generated using phase angle sorting. The variations in respiratory amplitude were significantly smaller 共P ⬍ 0.001兲 with amplitude sorting than those with phase angle sorting. The subdivision of the breathing cycle into more 共finer兲 phases improved the consistency in respiratory amplitude for amplitude sorting, but not for phase angle sorting. For 33 of the 35 patients, the air content showed significantly improved 共P ⬍ 0.001兲 correlation with the respiratory amplitude than with the phase angle, suggesting a stronger relationship between internal motion and amplitude. Overall, amplitude sorting performed better than phase angle sorting for 33 of the 35 patients and equally well for two patients who were immobilized with a stereotactic body frame and an abdominal compression plate. © 2006 American Association of Physicists in Medicine. 关DOI: 10.1118/1.2219772兴 Key words: 4D CT, respiratory motion, radiotherapy, phase, amplitude I. INTRODUCTION Four-dimensional computed tomography 共4D CT兲 has been proposed as an imaging technique to support improving the accuracy of radiation therapy delivery in the presence of respiratory motion.1–8 A 4D CT dataset consists of a set of 3D images reconstructed at selected phases of the respiratory cycle, e.g., at the end of exhalation 共EE兲, middle inhalation 共MI兲, end of inhalation 共EI兲, and middle exhalation 共ME兲. CT scans are typically sorted into different respiratory phases based on either the amplitude or the phase angle of a respiratory trace, which is usually obtained with a synchronized external respiratory measurement. 共Phase angle is defined here as the fraction of time between user-specified phases of breathing, typically renormalized between the canonical angles of 0° to 360°. The term “phase” when used alone is reserved to describe a portion of the breathing cycle such as the end of inhalation.兲 Many groups have attempted to generate 4D CT datasets by using the phase angle as a sorting criterion.1–6,8 However, the respiratory cycle is often insuffi2964 Med. Phys. 33 „8…, August 2006 ciently reproducible so that using phase-angle sorting causes large inconsistencies in the image reconstruction. For respiration-gated radiotherapy, Vedam et al.9 stated that amplitude gating is better than phase angle gating because the amplitude is more accurately related to the target position. For the two patients shown in Vedam et al.,9 amplitude gating was determined to be more effective than phase angle gating for one patient and as effective for the other, who had more reproducible breathing. For 4D CT, Rietzel et al.10 qualitatively examined amplitude sorting and phase angle sorting for two patients. Phase angle sorting worked well for the first patient who had more reproducible breathing. For the second patient, it was found that phase angle did a poor job of representing respiratory motion. To highlight this, Rietzel et al.10 showed that when replacing phase angle sorting by amplitude sorting, a reconstruction artifact at the diaphragm was clearly reduced. It was not clear from the manuscript whether their amplitude sorting approach separated scans based on the direction of respiration, e.g., inhalation 0094-2405/2006/33„8…/2964/11/$23.00 © 2006 Am. Assoc. Phys. Med. 2964 2965 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT and exhalation. Recently, Fitzpatrick et al. presented a method to extract displacement 共amplitude兲 binned 共sorted兲 4D CT data from prospectively phase-binned image sets with small phase intervals.11 They showed, in this one-patient study, that the reconstructed image quality was improved with amplitude sorting 共separating inhalation from exhalation for middle phases兲. We have developed a 4D CT technique which sorts scans based on the amplitude and direction 共inhalation or exhalation兲 of tidal breathing.7,12,13 The breathing direction is included to allow consideration of hysteresis 共the difference between the inhalation and exhalation trajectories兲 in image reconstruction.13,14 A quantitative study demonstrated that 4D datasets reconstructed using this technique were both accurate and precise.13 In this work we compare, using both qualitative and quantitative tools, the effectiveness of amplitude sorting and phase-angle sorting in 4D CT during quiet, natural breathing, for 35 patients. II. METHODS AND MATERIALS A. CT image acquisition with synchronized external respiratory measurements A brief description of the 4D CT process and internal air content analysis is provided as follows:7,13 Transverse slices are acquired with a 16-slice CT scanner 共Brilliance 16, Philips Medical Systems, Cleveland, OH兲 operated in ciné mode 共couch stationary during scanning兲. The scanned thickness was 24 mm per couch position using 16 1.5 mm thick slices. Each scan 共360° rotation兲 required 0.42 s to acquire followed by a 0.30 s dead time. The CT scanner repeatedly acquired and reconstructed 25 scans at each couch position for 18 s. To keep the patient dose low, only a quarter of the clinical mAs 共40 mAs兲 was used in the imaging process. The dose per study was estimated to be about 8 cGy based on ion chamber measurements. The data are acquired contiguously in space, but there is a pause of approximately 4 s between two adjacent couch acquisitions. This process is conducted while the patient undergoes synchronized external respiratory measurements. The synchronization is provided by a digital 共TTL兲 signal 共“X-Ray On” signal兲 from the CT scanner that indicates when an acquisition starts. Two respiratory measurements—tidal volume from quantitative spirometry and a digital voltage signal from a wraparound differential pressure sensor 共“pneumo bellows”兲—are simultaneously acquired 共Fig. 1兲. The spirometry system measures the air flow into the lungs and has been shown to be a useful, verifiable physiologic measurement.13 The bellows system consists of an accordionlike cylindrical bellows that is strapped around the patient’s abdomen. The pressure within the bellows decreases as the patient inhales and consequently as the patient’s abdomen distends and their abdominal circumference increases, with the opposite happening as the patient exhales. This pressure change is measured by a remote pressure sensor that provides a direct-current voltage signal to an analogto-digital converter. Custom-written data acquisition software 共Labview, National Instruments, Dallas, TX兲 is used to Medical Physics, Vol. 33, No. 8, August 2006 2965 FIG. 1. System setup for 4D CT scan and acquisitions of two respiratory measurements: tidal volume from quantitative spirometry and a digital voltage signal from a wraparound differential pressure sensor “bellows.” Custom-written software is run on the workstation to acquire and display these signals 共bottom panel兲 as well as the “x-ray on” signal 共top panel兲. acquire the “X-Ray On” signal from the CT scanner, the spirometer readings 共via a serial interface兲, and the bellows signal 共Fig. 1兲. The spirometer signal has significant baseline level drift caused by the instruments,12,13,15 while the bellows pressure signal does not have such instrumental drift and is considered a drift-free measurement.16–18 However, the bellows signal was affected by sensor placement and patient positioning. To diminish the affect of these nonphysiologic circumstances on the relationship between the bellows signal and internal motion, the bellows signal 共in V兲 was converted into a pseudo tidal volume signal 共in ml兲 by multiplying the average ratio between a drift-corrected spirometer-measured tidal volume and bellows signal during the scan session. The drift correction along with a time offset correction was determined by maximizing a cross-correlation function between the two measurements during 18 s 共time required for each couch acquisition兲 segments as reported earlier.12 This generated a pseudo tidal volume measurement, which will be shortened as tidal volume thereafter and used as the respiratory metric. In this paper, the respiratory amplitude or amplitude refers to the tidal volume value. The internal air content analysis provides a measure of how much air volume is within the CT volume in a single couch position.19 The air content is determined by the Hounsfield values in segmented air-containing tissues 共lungs, trachea, bronchi兲.13 In a previous study, we showed that the internal air content correlated with tissue motion in the lung with a residual of less than 1 mm for 12 patients, and it provided quantitative evaluations for the 4D CT process.13 In this study, the internal air content was used as a surrogate for internal motion and as an independent measurement for comparing the two sorting approaches. A total of 39 sets of 4D CT data for 35 patients were acquired while the patients underwent quiet, natural breathing. Among the 35 patients, 19 had lung cancer, while 16 were treated with radiation therapy for upper-abdomen cancers. Three of the patients were scanned more than once. Four of the patients had stage I non-small-cell lung cancer and were treated with stereotactic body radiation therapy 2966 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT 共SBRT兲,20,21 in which an Elekta stereotactic body frame 共SBF, Elekta Inc., Norcross, GA兲 was used to immobilize the patient and an optional abdominal compression plate was used to reduce the motion of the tumor if it was 5 mm or more measured on a “short” 4D CT scan around the tumor region. phases. To determine the phase angle, first the peak and valley points in every breath were identified from the tidal volume trace with a semiautomatic method.22 Let t1, t2, and t3 be the times at the first peak, the following valley, and the second peak, respectively. The phases at these three points were defined as 0°, 180°, and 360°. The phase angle of a point at ti was linearly interpolated in time as B. 4D CT reconstruction using amplitude sorting We have developed a 4D CT reconstruction technique based on the amplitude and direction 共inhalation or exhalation兲 of tidal breathing.7,12,13 The direction was determined using a semi-automatic peak and valley detection method.22 A breath consisted of two branches: exhalation 共a peak to the following valley兲 and inhalation 共the valley to next peak兲. A composite three-dimensional 共3D兲 image can be reconstructed at an arbitrary tidal volume during inhalation or exhalation. For example, to reconstruct at 300 ml during inhalation, we select at each couch position the inhalation scan whose center tidal volume is nearest to 300 ml, repeating the process throughout all couch positions to generate the 3D image dataset. The selection of tidal volumes used for reconstruction was not arbitrary. Two of the 3D images were reconstructed at end inhalation and end exhalation. However, there existed no adequate definition for these two phases for sessions with multiple breaths, so one was developed to support these imaging studies. Because breathing was inherently irreproducible, the tidal volume for each inhalation and exhalation varied. Reconstructing a composite 3D image at a selected tidal volume required there to be CT scans acquired near that tidal volume. The practical definition of exhalation/inhalation became the smallest/largest tidal volume for which a 3D image could be reconstructed within 5% error 共in terms of the difference between mean tidal volume for selected scans to the desired tidal volume兲. We used v1 and v95 tidal volumes for EE and EI, respectively, where vx was the percentile tidal volume.13,23 For example, the 95th percentile tidal volume, v95, was the tidal volume at which the patient had that tidal volume or less 95% of the time during the scanning session. Using percentiles has the advantage over percentages in that it takes into consideration the relative time a patient reached a tidal amplitude level so that it is much less affected by the few extreme breaths 共very deep inhalation or exhalation兲 often seen during the entire scan session. For this study, we reconstructed 4D CT datasets at six inhalation phases and six exhalation phases. The six phases had the same amplitude levels for inhalation and exhalation: v1 and v95 were the lowest and highest levels, and the other four levels were evenly spaced between v1 and v95. Using these definitions, v1 inhalation corresponded to start of inhalation 共SI兲, v95 inhalation EI, v95 exhalation start of exhalation 共SE兲, v1 exhalation EE, and 共v95 + v1兲 / 2 MI or ME. C. 4D CT reconstruction using phase-angle sorting We adopted a phase-angle sorting technique used by others3,5,6 to reconstruct 4D CT datasets at 12 respiratory Medical Physics, Vol. 33, No. 8, August 2006 2966 i = ti − t1 ⫻ 180 ° , t2 − t1 if t1 ⱕ ti ⱕ t2 , 共1兲 ti − t2 i = 180 ° + ⫻ 180 ° , t3 − t2 if t2 ⬍ ti ⱕ t3 . This process was repeated for each breath. For example, using this method, the phase angle 210° corresponded to SI, phase angle 270° MI, phase angles 0° and 360° EI, phase angle 30° SE, phase angle 90° ME, and phase angle 180° EE. For reconstruction, scans whose center phase angle is closest to the user-specified phase angle were collected to produce a composite 3D image dataset. This was done for the 12 phases evenly spaced between 0° and 360° of a respiratory cycle. D. Variations in tidal volume for each respiratory phase with amplitude sorting and phase-angle sorting An assumption of the variation analysis was that, for quiet respiration, lung motion was largely proportional to the externally measured respiratory amplitude.13,24 Under this assumption, smaller variation in tidal volume would suggest smaller residual motion or an improved reconstructed image for a specific respiratory phase. The variations 共quantified by the standard deviation, s.d.兲 in tidal volume for each phase were computed and compared between amplitude sorting and phase-angle sorting. This was done for 共1兲 the entire scan session 共500– 1000 s兲 for the 12 respiratory phases, 共2兲 all scans that were used in the reconstruction for the 12 3D composite images, and 共3兲 the entire scan session for 8, 12, 24, and 48 respiratory phases. E. Correlating air content with respiratory amplitude and phase angle As described in Sec. II A, the internal air content was used as a surrogate for internal motion and as an independent measurement for comparison of the two sorting metrics 共amplitude and phase angle兲. A smaller fitting residual 共root mean squared error兲 between a metric and the air content suggested a stronger relationship of the metric with internal motion. We found that air content showed a strong linear relationship with respiratory amplitude at each couch position within the lung.12,13 We observed that the air content showed a quadratic relationship with phase angle at each couch position within the lung. The residuals of a linear fitting between air content and respiratory amplitude were compared to those of a quadratic fitting between air content and phase angle throughout couch positions within the lung. 2967 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT 2967 TABLE I. Patient breathing characteristics. T and sdT are the mean and s.d. of breathing period, v and sdv are the mean and s.d. of peak to peak tidal volume amplitude. Patient no. Dataset no. Cancer site 1 2 2 3 3 4 6 6 6 10 13 14 19 20 22 23 24 25 27 28 30 33 34 5 7 8 9 11 12 15 16 17 18 21 26 29 31 32 35 Mean 1 2 3 4 5 6 8 9 10 14 17 18 23 24 26 27 28 29 31 32 34 37 38 7 11 12 13 15 16 19 20 21 22 25 30 33 35 36 39 Lung Lung Lung Lunga Lunga Lung Lunga Lunga Lunga Lung Lung Lung Lungb Lungb Lung Lung Lung Lung Lung Lung Lung Lung Lung Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen T 共s兲 4.5 3.1 2.8 2.7 3.0 4.7 7.6 8.6 7.5 3.0 2.4 3.2 4.5 3.5 3.6 5.1 3.3 3.8 3.4 4.0 2.6 4.2 7.6 8.6 3.5 4.7 6.9 4.2 3.9 4.9 3.9 4.5 4.5 4.7 3.8 3.9 4.8 3.1 9.2 4.6 sdT 共s兲 1.1 0.7 0.5 0.3 0.2 0.8 1.1 1.2 0.8 0.5 0.7 0.5 0.8 0.3 0.5 2.5 0.3 1.8 0.3 0.5 0.5 0.6 1.2 1.5 0.6 0.7 1.4 0.4 0.7 1.4 1.3 1.8 1.0 0.5 0.3 0.5 0.7 0.6 2.4 0.9 v 共ml兲 sdv 共ml兲 680.3 532.2 527.2 377.1 346.4 343.9 731.2 649.1 566.4 415.6 263.2 734.5 745.0 424.1 314.7 379.2 136.7 436.0 612.1 448.4 373.1 529.8 1197.8 1073.7 479.4 707.8 531.3 565.4 506.9 496.7 518.5 595.2 745.0 459.5 323.9 643.0 430.0 348.8 1560.2 557.7 141.9 129.4 73.9 37.8 33.0 75.4 87.1 142.0 73.3 44.6 63.6 124.4 89.0 36.1 34.2 209.1 16.4 109.1 58.2 37.6 93.5 76.6 209.4 244.4 55.7 100.6 64.4 65.7 93.4 181.5 123.8 141.1 116.2 72.3 37.8 182.3 141.0 48.0 365.1 103.3 a Patients underwent SBRT in a SBF with an abdominal compression plate. Patients underwent SBRT in a SBF without abdominal compression plate. b III. RESULTS A. Characterization of patient breathing period and amplitude In each of the 39 patient data sets, the respiratory trace demonstrated variations in period and amplitude from breath to breath and from patient to patient. Table I lists the mean and s.d. of breathing period and peak to peak amplitude for each patient data set. Data sets 2 and 3, 4 and 5, and 8, 9, and 10 were multiple scan sessions from three lung cancer patients. Data set 28 represented a lung-cancer patient with only the left lung operating and had the smallest peak to peak Medical Physics, Vol. 33, No. 8, August 2006 FIG. 2. Samples of the internal air content, tidal volume 共amplitude兲, and phase angle for a couch position in the middle of lung and intercepting the diaphragm 共patient data set 21兲. The data points indicate the tidal volume and phase angle for each scan, respectively. Phase angles of 0° or 360° corresponded to end of inhalation 共EI兲, 180° was the end of exhalation 共EE兲, 90° was the mid-exhalation 共ME兲, and 270° was mid-inhalation 共MI兲. amplitude. The mean breathing period ranged from 2.4 to 9.2 s with an average of 4.6 s. The s.d. in the period ranged from 0.2 to 2.5 s, or from 6.7% to 49.0% as a ratio over the mean period. The mean peak to peak amplitude ranged from 263.2 ml 共excluding data set 28兲 to 1560.2 ml, with an average of 557.7 ml. The s.d. in the amplitude ranged from 33.0 ml 共excluding data set 28兲 to 365.1 ml, or from 8.4% to 55.1% as a ratio over the mean amplitude. There was no significant difference in any of these variables between patients with lung cancers and patients with upper-abdomen cancers 共all P ⬎ 0.05兲. Data set 21, with large variations, and data set 5, with smallest variations 共as a ratio of the mean兲 in breathing period and amplitude, were selected as example patients. B. Phase angle calculation Figure 2 shows samples of the internal air content, tidal volume 共amplitude兲, and calculated phase angle for data set 21 at a couch position near the middle of the lung and intercepting the diaphragm. The phase angle was calculated with Eq. 共1兲 on the tidal volume trace. Notice that due to the asymmetrical inhalation and exhalation in time 共t2 − t1 ⫽ t3 − t2兲, the calculated phase angle for one cycle 共0 ° – 360° 兲 consisted of two line segments with a transition point at 180° 共EE兲. Also the slopes of the two line segments varied from breath to breath. C. Images reconstructed using amplitude sorting and phase-angle sorting Figure 3 compares sagittal lung images reconstructed using amplitude sorting and phase-angle sorting. A sagittal view is chosen because motions in the craniocaudal and anteroposterior directions are generally larger than motions in 2968 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT 2968 FIG. 3. Images reconstructed using amplitude sorting 共top row兲 and phaseangle sorting 共bottom row兲. 共a兲 A patient 共data set 21兲 with relatively irreproducible breathing. 共b兲 A patient 共data set 5兲 with relatively reproducible breathing. From left to right in each row: end exhalation, middle inhalation, end inhalation, and middle exhalation. Arrows indicate significant reconstruction artifacts. the lateral direction in the lung, so errors in reconstruction are more easily detected. Images for 4 of the 12 respiratory phases are shown: EE, MI, EI, and ME. For patient data set 21 关Fig. 3共a兲兴, the tumor is observable near the diaphragm apex. Images generated using amplitude sorting display smoother lung-diaphragm boundaries and minimal reconstruction artifacts. Images generated using phase-angle sorting, however, display distorted lung-diaphragm boundaries at all four phases. The vessel in the middle of the lung appears broken in the ME image with phase-angle sorting. For patient data set 5 关Fig. 3共b兲兴, images generated using both sorting approaches display similarly smooth lung-diaphragm boundaries and minimal reconstruction artifacts for all four phases except for ME, where one reconstruction artifact is visible with phase-angle sorting. Animations of the lung motion during a respiratory cycle were generated with images at all 12 phases. Animations for amplitude sorting were observed to show smoother lung motion, less tissue jumping motion, and less distortion at the lung-diaphragm boundary than those for phase-angle sorting. Similar results were observed for all 35 patients. In summary, amplitude sorting provided better images and animations, as compared to phase-angle sorting. D. Variations in tidal volume with amplitude sorting and phase-angle sorting 1. A visual comparison Figure 4 shows the variation in tidal volume for two breathing samples for MI and EI 共patient data set 21兲. The period of the patient’s breathing varies appreciably among breaths in Figs. 4共a兲 and 4共b兲. All data points classified by Medical Physics, Vol. 33, No. 8, August 2006 FIG. 4. Variation in tidal volume with amplitude sorting 关共a兲 and 共c兲兴 and phase-angle sorting 关共b兲 and 共d兲兴 for patient data set 21. Two breathing samples are shown for middle inhalation 关共a兲 and 共b兲兴 and end inhalation 关共c兲 and 共d兲兴. Thicker segments indicate aggregated data points falling into each respiratory phase. amplitude sorting as MI correspond to a consistent intermediate tidal volume close to 共v95 + v1兲 / 2 关Fig. 4共a兲兴. On the other hand, many data points classified by phase-angle sorting as MI clearly do not correspond to a consistent intermediate tidal volume 关Fig. 4共b兲兴. Particularly, data points classified as MI for two long breaths 共545– 555 s and 564– 577 s兲 have very small tidal volumes. In Figs. 4共c兲 and 4共d兲, the peak to peak tidal volume varies appreciably among breaths. Data points from shallow breaths are excluded by amplitude sorting for EI 关Fig. 4共c兲兴 but are classified as EI by phase-angle sorting 关Fig. 4共d兲兴. Basically, phase-angle sorting regards a shallow breath 共⬃300 ml兲 the same as a normal 共⬃700 ml兲 and a deep breath 共⬃1000 ml兲. Clearly, the variation in tidal volume for either respiratory phase is smaller with amplitude sorting than with phase-angle sorting. 2. Entire scan session for 12 respiratory phases Figure 5 shows scatter plots of the tidal volume and phase angle during the entire scan session for the example patients. 2969 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT FIG. 5. Scatter plot of tidal volume and phase angle. 共a兲 A patient 共data set 21兲 with relatively irreproducible breathing. 共b兲 A patient 共data set 5兲 with reproducible breathing. One out of every 10 measured time points is shown for the entire scan session. The tidal volume values are spread out at any single phase angle value, indicating that the amplitude at a phase angle changes considerably from breath to breath. Figure 6 shows the variation 共s.d.兲 in tidal volume at the 12 respiratory phases for amplitude sorting and phase-angle sorting for the entire scan session. For amplitude sorting, the variation in tidal volume is close to a constant for the 12 phases since the range of tidal volume was the same for each phase. The variations at the breathing ends are slightly smaller than those at the middle of breathing. This is because not every breath had data points that covered the entire range of tidal volume at those breathing ends. All patients had a similar shape of the variation curve. For phase-angle sorting, the variation was different at each phase. For both patients shown, the variation is larger at greater tidal volumes 共MI, EI, ME兲 than at lesser tidal volumes 共SI, EE兲, indicating that the patients breathed less reproducibly at greater tidal volumes than at lesser tidal volumes. Also notice that this variation is different at ME 共phase angle 90°兲 from that at MI Medical Physics, Vol. 33, No. 8, August 2006 2969 FIG. 6. Variation in tidal volume at 12 respiratory phases for amplitude sorting and phase-angle sorting. 共a兲 A patient 共data set 21兲 with relatively irreproducible breathing. The mean peak to peak amplitude is 595.2 ml. 共b兲 A patient 共data set 5兲 with reproducible breathing. The mean peak to peak amplitude is 346.4 ml. Variation is taken for all data points in the entire scan session. 共phase angle 270°兲. This change in the variation curve was expected since the spread of tidal volume varied at each phase as shown in Fig. 5. The shape of the tidal volume variation curve was different for each patient. The mean variation for the 12 phases was smaller with amplitude sorting than with phase-angle sorting for both patients. The mean variation in tidal volume was significantly smaller 共P ⬍ 0.001兲 with amplitude sorting than with phase-angle sorting for all patients 共Table II兲. There was no significant difference in the mean variation for amplitude sorting or phaseangle sorting between patients with lung cancer and patients with upper-abdomen cancers 共both P ⬎ 0.05兲. 3. Data points during CT scans used in the reconstruction for the 12 respiratory phases Figure 7 shows the variation in tidal volume of data points during CT scans used in the reconstruction for each of the 12 3D composite images. For phase-angle sorting, every scan 2970 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT 2970 TABLE II. Comparison results. The mean variation in tidal volume, with amplitude sorting 共A兲 and phase angle sorting 共P兲, respectively, for entire scan session 共sdA1 , sdP1兲 and for data points during CT scans used in the reconstruction for each of the 12 3D composite images 共sdA2 , sdP2兲. The mean fitting residuals of air content to amplitude 共resA兲 and to phase angle 共resP兲, respectively. Patient Dataset Cancer no. no. site 1 2 2 3 3 4 6 6 6 10 13 14 19 20 22 23 24 25 27 28 30 33 34 5 7 8 9 11 12 15 16 17 18 21 26 29 31 32 35 Mean 1 2 3 4 5 6 8 9 10 14 17 18 23 24 26 27 28 29 31 32 34 37 38 7 11 12 13 15 16 19 20 21 22 25 30 33 35 36 39 Lung Lung Lung Lunga Lunga Lung Lunga Lunga Lunga Lung Lung Lung Lungb Lungb Lung Lung Lung Lung Lung Lung Lung Lung Lung Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen Abdomen resA 共ml兲 resP 共ml兲 sdA1 共ml兲 11.8 3.9 4.5 4.0 4.2 4.9 5.1 5.6 6.7 2.7 3.6 5.9 4.0 4.3 5.3 5.9 5.3 3.2 3.1 3.9 4.9 3.5 6.1 7.5 4.1 2.3 5.0 4.0 2.6 4.3 3.4 3.9 3.7 4.1 3.1 2.1 3.7 3.3 6.0 4.5 13.3 6.3 6.0 3.3 3.0 4.9 4.5 5.0 4.5 3.8 5.9 8.5 6.4 5.0 6.6 9.4 6.6 5.2 5.0 5.3 5.9 5.2 11.8 10.0 5.0 4.0 6.5 4.3 4.3 5.8 7.3 6.7 4.3 5.3 4.5 5.4 6.2 4.6 12.2 6.1 43.8 38.4 35.2 22.7 18.8 19.9 43.4 40.6 36.3 23.8 18.8 45.5 45.7 29.4 17.5 39.9 17.5 31.9 37.5 24.9 24.4 32.7 79.8 69.5 31.1 45.2 31.1 32.6 35.5 44.2 39.5 41.6 43.6 27.5 20.0 40.3 31.6 21.5 99.1 36.5 sdP1 共ml兲 sdA2 共ml兲 sdP2 共ml兲 106.0 51.5 105.5 46.0 81.1 39.2 40.2 28.8 27.8 30.5 42.3 23.3 79.2 55.0 92.1 50.0 80.6 55.6 41.4 22.1 44.1 20.5 102.2 50.6 100.9 45.0 65.8 35.3 27.6 20.6 191.2 71.0 27.6 20.6 118.7 38.5 72.0 36.3 40.7 26.7 56.5 29.8 68.6 32.7 193.1 80.0 154.6 67.8 65.9 42.1 97.7 52.1 54.5 30.8 54.3 35.2 93.3 39.8 148.8 35.8 120.2 52.9 127.9 61.7 106.0 50.3 65.6 31.0 41.7 22.6 101.0 45.2 98.6 43.1 40.6 21.5 219.7 103.3 87.1 42.2 111.8 99.0 74.6 39.2 30.5 40.0 81.8 96.8 92.9 39.5 43.5 97.6 100.1 68.6 28.5 183.7 28.5 105.6 72.4 42.1 53.1 67.0 193.0 159.8 66.4 99.7 55.5 57.9 94.9 78.1 123.8 130.5 113.9 59.3 43.0 99.2 98.7 40.8 207.2 85.1 a Patients underwent SBRT in a SBF with an abdominal compression plate. Patients underwent SBRT in a SBF without abdominal compression plate. b used in the reconstruction for a respiratory phase belonged to that phase. The shape of the variation curves were, therefore, similar to those in Fig. 6. For amplitude sorting, not all of the scans used in the reconstruction for a specific respiratory phase belonged to that phase. For example, if a patient breathed shallowly at a couch position so that none of the 25 scans fell into the EI phase, an inhalation scan with tidal volume closest to but less than the lower limit of EI would be selected in the reconstruction for the 3D EI image. This Medical Physics, Vol. 33, No. 8, August 2006 FIG. 7. Variation in tidal volume at 12 respiratory phases for amplitude sorting and phase-angle sorting. 共a兲 A patient 共data set 21兲 with relatively irreproducible breathing. 共b兲 A patient 共data set 5兲 with reproducible breathing. Variation is taken for data points used in the reconstruction for each of the 12 3D composite images. would cause a larger tidal volume variation at EI than that in Fig. 6. For both patients, the increased variations at EI and its two neighboring respiratory phases were caused by selecting scans from shallow breaths. The mean variation for the 12 images was smaller with amplitude sorting than with phase-angle sorting for data set 21, and equal for data set 5. The mean variation in tidal volume was significantly smaller 共P ⬍ 0.001兲 with amplitude sorting than with phase-angle sorting for all patients 共Table II兲. There was no significant difference in the mean variation for amplitude sorting or phase angle sorting between patients with lung cancer and patients with upper-abdomen cancers 共both P ⬎ 0.05兲. 4. Entire scan session for 8, 12, 24, and 48 respiratory phases Figure 8 shows the variation in tidal volume during the scan session at 8, 12, 24, and 48 respiratory phases for data set 21 with amplitude sorting and phase-angle sorting, respectively. For amplitude sorting, the variation was reduced 2971 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT 2971 with the use of more 共finer兲 phases because the range of tidal volume within each phase decreased. For phase-angle sorting, the variation was not reduced and the other three variation curves displayed a shape similar to that with 12 phases. This was because that though using more phases reduced the within-breath tidal volume variation, it had no effect on the much larger between-breath variation for each phase. Similar results were obtained for all 39 patient data sets. E. Correlating air content with respiratory amplitude and phase angle FIG. 8. Variation in tidal volume at 8, 12, 24, and 48 respiratory phases for amplitude sorting 共Amp兲 and phase-angle sorting 共Pha兲, respectively, from dataset 21. Variation is taken for all data points in the entire scan session. Figures 9共a兲 and 9共b兲 show the results of fitting air content to tidal volume and phase angle for the 25 scans shown in Fig. 2. The fitting residual is 11.5 ml in air content for amplitude and 29.4 ml for phase angle, out of a total air content variation of 200 ml. Figures 9共c兲 and 9共d兲 display the fitting residuals for all couch positions within the lung. For data set 21, the mean residual for respiratory amplitude is smaller FIG. 9. 共a兲 A linear fit between air content and tidal volume. The fitting residual is 11.5 ml. 共b兲 A quadratic fit between air content and phase angle. The fitting residual is 29.4 ml. Comparison of fitting residuals throughout all couch positions within the lung for 共c兲 a patient 共data set 21兲 with relatively irreproducible breathing and 共d兲 a patient 共data set 5兲 with reproducible breathing. Medical Physics, Vol. 33, No. 8, August 2006 2972 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT than that for phase angle. For data set 5, the mean residual for respiratory amplitude is larger than that for phase angle. Table II shows that for all 35 patients but two of the four SBF patients with abdominal compression plate 共patient 3, data sets 4 and 5; patient 6, data sets 8, 9, and 10; both had lung cancers兲, the mean fitting residual is smaller for amplitude than for phase angle. The mean fitting residual was significantly smaller 共P ⬍ 0.001兲 for amplitude than for phase angle for all patients. This suggests that there is usually a stronger relation between lung motion and respiratory amplitude than that between lung motion and phase angle. There was no significant difference in the mean fitting residual for amplitude or phase angle between patients with lung cancer and patients with upper-abdomen cancers 共both P ⬎ 0.05兲. IV. DISCUSSION AND CONCLUSION The results demonstrate that for all 35 patients, the variation in tidal volume, and by extension that the variation in respiratory motion, was smaller for amplitude sorting than for phase-angle sorting with 12 respiratory phases. For all patients but two SBF patients with abdominal compression plate, the correlation between lung motion and respiratory amplitude was stronger than that between lung motion and phase angle. For all patients, qualitative comparisons demonstrated that images and animations reconstructed by amplitude sorting provided smoother lung-diaphragm boundaries and fewer artifacts than those reconstructed by phaseangle sorting. In summary, for respiration correlated 4D CT in 35 patients who underwent quiet breathing, amplitude sorting performed better than phase-angle sorting for 33 patients and equally well for two patients with more reproducible breathing. Data in the literature, though limited, all reached the same conclusion.9–11 Phase-angle sorting, however, is still more widely used than amplitude sorting for 4D CT. This choice might be due to the ease of access to hardware and software for phase-angle-based electrocardiogram-gated heart imaging. While heart motion is highly reproducible with respect to the cardiac phase angle,25 respiratory motion is far less reproducible with respect to the respiratory phase angle. As shown in both this study and other studies,10,11 phase angles do not 共sufficiently兲 represent respiratory motion for irreproducible breathing, which is the case for most patients who undergo free/quiet breathing. One may argue that an advantage of phase-angle sorting is that a complete phase angle range 共0 ° – 360° 兲 is completely covered with each respiratory cycle; therefore, the time for data acquisition is shortened by requiring data acquisition for only one respiratory cycle at each couch position.6 With this approach, the image reconstruction quality relies greatly on the reproducibility of breathing. It has been reported10,11 that when the respiratory pattern 共period, amplitude, and respiratory trace shape兲 was not sufficiently reproducible, phaseangle sorting resulted in missing images and significant residual motion artifacts. Amplitude sorting clearly reduced the residual motion artifacts in those studies and in the present Medical Physics, Vol. 33, No. 8, August 2006 2972 study. The current ciné protocol acquires images at each couch position while the patient breathes two to six cycles during the 18 s acquisition time. The probability that no image falls into a specific respiratory phase with amplitude sorting is thus reduced, and the error it creates is reduced as well. By using the amplitude sorting and the percentile scheme, the extreme breaths 共very deep inhalation or exhalation兲 are excluded from the 4D CT reconstruction. This improves the consistency in the reconstructed images. Because phase angle does not contain sufficient amplitude information, amplitude monitoring is necessary to detect and ignore imaged data acquired during such extreme breaths. In a study for five patients, breathing coaching using audio instruction resulted in reproducible breathing period, but with increased variability and magnitude of amplitude.26 In the same study, obtaining more controllable breathing amplitudes was attempted using visual feedback.26 In another study for 24 lung cancer patients, however, free breathing was reported to have smaller variations in amplitude and period than audio instruction and audio-visual biofeedback.27 Breathing coaching is usually considered an important component for 4D CT techniques when phase-angle sorting is used.2,3,5,28 Although breathing coaching was not used in our 4D CT technique, the images reconstructed using amplitude sorting showed good quality with minimal reconstruction artifacts even for irregular breathers. Breathing coaching may benefit both amplitude sorting and phase-angle sorting, but several questions on its efficacy and practicability would need further investigation: 共1兲 Does breathing coaching significantly improve the reproducibility of the comprehensive breathing pattern, including the reproducibility of amplitude and period? 共2兲 Does breathing coaching significantly improve the consistency of the relationship between the target motion and the 共external兲 respiratory measurements? 共3兲 What is the percentage of patients who can be trained successfully? 共4兲 Which respiratory feedback measurement should be used for coaching? The results of the amplitude sorting and phase-angle sorting comparisons do not depend on the external respiratory measurement used for the sorting process, provided that it is functionally related to the breathing depth. Some external respiratory measurement systems, such as spirometry, cannot be used independently because their signal drifts with time.12,13,15 Drift corrections are necessary when using such a system for amplitude sorting.7,13,15 The baseline drift usually is not sufficiently large to affect neither phase angle definition nor phase-angle sorting. Other measurements, such as the “bellows,” reflective surface markers 共as used in the Real-Time Position Management, RPM, Varian Medical Systems, Palo Alto, CA兲, or position-sensitive semiconductor detectors, are considered drift-free.16,17,29 A drift-free measurement or a combination of a drift-free measurement and spirometry12,16 is recommended for amplitude-based sorting. Finally, one should be cautious when using an external respiratory measurement to infer internal tumor or tissue motion.12,30,31 With current scanner rotation speeds 共0.3– 0.5 s rotation time兲, 8 to 12 respiratory phases are reconstructed in 4D CT. 2973 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT If the scanner rotation time is shortened and the temporal resolution is improved, it may be feasible to reconstruct images at more 共finer兲 respiratory phases. We have shown that the use of finer respiratory phases may improve the consistency in tidal volume for amplitude sorting, but not for phase-angle sorting. This suggests that amplitude sorting will take advantage of the increased scanner speed relative to phase-angle sorting. For all 35 patients but the two SBF patients with abdominal compression plate 共patients 3 and 6兲, there was a stronger relation between internal air content 共or equivalently lung motion兲 with respiratory amplitude than with phase angle. The compression plate provided more restricted immobilization and limited the respiration amplitude. As a result, a more reproducible breathing pattern was observed for the two patients, such as relatively more consistent tidal volume as a function of phase angle for patient 3 关Fig. 5共b兲兴. On the other hand, patient 3 共data sets 4 and 5兲 had small variations in both the mean breathing period and amplitude 共Table I兲; patient 6 共data sets 8, 9, and 10兲 had medium variations in both 共Table I兲. Small variations in the mean period and amplitude, however, did not necessarily suggest a stronger relation between air content and phase angle. Also note that in this correlation analysis, we introduced a quadratic relationship between phase angle and air content. In the variation analysis, however, phase angle was used directly to infer the tidal amplitude or target position. This might explain why phase angle performed better in the correlation analysis than in the variation analysis 共Table II兲. Nevertheless, phase angle did not correlate as strongly as amplitude to air content for most patients. Data in this paper indicated that there was no significant difference 共all P ⬎ 0.05兲, in the patient breathing characteristics 共mean or s.d. of amplitude, mean or s.d. of period兲, or in the calculated variables 共mean fitting residual, mean variation in tidal volume, for either amplitude or phase angle兲, between patients with lung cancer and patients with upperabdomen cancers. When we examined the respiratory waveforms, we observed arbitrary variations for each patient rather than systematic differences between these two groups of patients. This suggested that for our data the respiration motion was not affected by the type of cancer a patient had. Among patients with lung cancers, the fitting residuals with phase angle 共resP兲 were significantly smaller 共P = 0.04兲 for the four SBRT patients. This implies that using the SBF with the optional compression plate may improve the correlation between internal motion and phase angle. There was no significant difference 共all P ⬎ 0.05兲 in the other variables. A limitation of this work is that true, real-time target 共tumor兲 motion is not available and surrogates 共tidal volume and air content兲 are being used. Reliably tracking tumor motion in 3-D is an ongoing research. Fluoroscopically tracking implanted markers4,14,31–35 may yield the most reliable 3-D tumor position, however, this technique is invasive and has other limitations.14,34 A recent study showed that tumors in the lung can be tracked with a biplane digital radiography unit, while implanted markers were still needed for tumors in Medical Physics, Vol. 33, No. 8, August 2006 2973 the liver and esophagus.35 Fluoroscopically tracking the superior-inferior diaphragm motion has been conducted but is limited by the fact that only 1-D diaphragm motion was measured.9,17,36,37 Our institution is investigating the use of non-ionizing implanted AC electromagnetic transponders 共4D Localization System, Calypso Medical, Seattle, WA兲 for tracking organ motions.38,39 When reliable target motion data are available, we would be able to compare the two sorting approaches in terms of the variation in target motion and correlation with target motion. ACKNOWLEDGMENTS This work was supported in part by National Institute of Health Grant No. R01 CA 096679. The authors thank Joe Repp and Roy Wood for help in collecting some data. a兲 Author to whom correspondence should be addressed. Electronic mail: dlow@radonc.wustl.edu 1 E. C. Ford, G. S. Mageras, E. Yorke, and C. C. Ling, “Respirationcorrelated spiral CT: a method of measuring respiratory-induced anatomic motion for radiation treatment planning,” Med. Phys. 30, 88–97 共2003兲. 2 P. Keall, “4-dimensional computed tomography imaging and treatment planning,” Semin. Radiat. Oncol. 14, 81–90 共2004兲. 3 P. J. Keall, G. Starkschall, H. Shukla, K. M. Forster, V. Ortiz, C. W. Stevens, S. S. Vedam, R. George, T. Guerrero, and R. Mohan, “Acquiring 4D thoracic CT scans using a multislice helical method,” Phys. Med. Biol. 49, 2053–2067 共2004兲. 4 H. Shirato, S. Shimizu, K. Kitamura, T. Nishioka, K. Kagei, S. Hashimoto, H. Aoyama, T. Kunieda, N. Shinohara, H. Dosaka-Akita, and K. Miyasaka, “Four-dimensional treatment planning and fluoroscopic realtime tumor tracking radiotherapy for moving tumor,” Int. J. Radiat. Oncol., Biol., Phys. 48, 435–442 共2000兲. 5 S. S. Vedam, P. J. Keall, V. R. Kini, H. Mostafavi, H. P. Shukla, and R. Mohan, “Acquiring a four-dimensional computed tomography dataset using an external respiratory signal,” Phys. Med. Biol. 48, 45–62 共2003兲. 6 T. Pan, T. Y. Lee, E. Rietzel, and G. T. Chen, “4D-CT imaging of a volume influenced by respiratory motion on multi-slice CT,” Med. Phys. 31, 333–340 共2004兲. 7 D. A. Low, M. Nystrom, E. Kalinin, P. Parikh, J. F. Dempsey, J. D. Bradley, S. Mutic, S. H. Wahab, T. Islam, G. Christensen, D. G. Politte, and B. R. Whiting, “A method for the reconstruction of four-dimensional synchronized CT scans acquired during free breathing,” Med. Phys. 30, 1254–1263 共2003兲. 8 G. S. Mageras, A. Pevsner, E. D. Yorke, K. E. Rosenzweig, E. C. Ford, A. Hertanto, S. M. Larson, D. M. Lovelock, Y. E. Erdi, S. A. Nehmeh, J. L. Humm, and C. C. Ling, “Measurement of lung tumor motion using respiration-correlated, CT,” Int. J. Radiat. Oncol., Biol., Phys. 60, 933– 941 共2004兲. 9 S. S. Vedam, P. J. Keall, V. R. Kini, and R. Mohan, “Determining parameters for respiration-gated radiotherapy,” Med. Phys. 28, 2139–2146 共2001兲. 10 E. Rietzel, T. Pan, and G. T. Chen, “Four-dimensional computed tomography: image formation and clinical protocol,” Med. Phys. 32, 874–889 共2005兲. 11 M. J. Fitzpatrick, G. Starkschall, J. A. Antolak, J. Fu, H. Shukla, P. J. Keall, P. Klahr, and R. Mohan, “Displacement-based binning of timedependent computed tomography image data sets,” Med. Phys. 33, 235– 246 共2006兲. 12 W. Lu, D. A. Low, P. J. Parikh, M. M. Nystrom, I. M. ElNaqa, S. H. Wahab, M. Handoko, D. Fooshee, and J. D. Bradley, “Comparison of spirometry and abdominal height as four-dimensional computed tomography metrics in lung,” Med. Phys. 32, 2351–2357 共2005兲. 13 W. Lu, P. J. Parikh, I. M. El Naqa, M. M. Nystrom, J. P. Hubenschmidt, S. H. Wahab, S. Mutic, A. K. Singh, G. E. Christensen, J. D. Bradley, and D. A. Low, “Quantitation of the reconstruction quality of a fourdimensional computed tomography process for lung cancer patients,” Med. Phys. 32, 890–901 共2005兲. 14 Y. Seppenwoolde, H. Shirato, K. Kitamura, S. Shimizu, M. van Herk, J. 2974 Lu et al.: Amplitude sorting and phase-angle sorting for 4D CT V. Lebesque, and K. Miyasaka, “Precise and real-time measurement of 3D tumor motion in lung due to breathing and heartbeat, measured during radiotherapy,” Int. J. Radiat. Oncol., Biol., Phys. 53, 822–834 共2002兲. 15 T. Zhang, H. Keller, M. J. O’Brien, T. R. Mackie, and B. Paliwal, “Application of the spirometer in respiratory gated radiotherapy,” Med. Phys. 30, 3165–3171 共2003兲. 16 T. Zhang, H. Keller, R. Jeraj, M. J. O’Brien, K. Sheng, T. R. Mackie, and B. Paliwal, “Lung motion tracking with a combined spirometer-laser sensor system,” Med. Phys. 29, 1309–1309 共abstract兲 共2002兲. 17 S. Minohara, T. Kanai, M. Endo, K. Noda, and M. Kanazawa, “Respiratory gated irradiation system for heavy-ion radiotherapy,” Int. J. Radiat. Oncol., Biol., Phys. 47, 1097–1103 共2000兲. 18 H. D. Kubo and B. C. Hill, “Respiration gated radiotherapy treatment: a technical study,” Phys. Med. Biol. 41, 83–91 共1996兲. 19 E. A. Hoffman and E. L. Ritman, “Effect of body orientation on regional lung expansion in dog and sloth,” J. Appl. Physiol. 59, 481–491 共1985兲. 20 R. C. McGarry, L. Papiez, M. Williams, T. Whitford, and R. D. Timmerman, “Stereotactic body radiation therapy of early-stage non-small-cell lung carcinoma: phase I study,” Int. J. Radiat. Oncol., Biol., Phys. 63, 1010–1015 共2005兲. 21 R. Timmerman, L. Papiez, R. McGarry, L. Likes, C. DesRosiers, S. Frost, and M. Williams, “Extracranial stereotactic radioablation: results of a phase I study in medically inoperable stage I non-small cell lung cancer,” Chest 124, 1946–1955 共2003兲. 22 W. Lu, M. M. Nystrom, P. J. Parikh, D. R. Fooshee, J. P. Hubenschmidt, J. D. Bradley, and D. A. Low, “A computerized method for peak and valley detection in respiratory waveforms without flow measurement,” Med. Phys. 33, 2021–2021 共abstract兲 共2006兲. 23 S. H. Wahab, P. J. Parikh, M. M. Nystrom, I. M. ElNaqa, J. P. Hubenschmidt, B. Pierburg, W. Lu, J. D. Bradley, and D. A. Low, “Treatment planning using four dimensional computed tomography,” Proceedings of the 14th International Conference on the Use of Computers in Radiation Therapy, Seoul, Korea 共2004兲. 24 S. S. Vedam, V. R. Kini, P. J. Keall, V. Ramakrishnan, H. Mostafavi, and R. Mohan, “Quantifying the predictability of diaphragm motion during respiration with a noninvasive external marker,” Med. Phys. 30, 505–513 共2003兲. 25 B. Ohnesorge, T. Flohr, C. Becker, A. F. Kopp, U. J. Schoepf, U. Baum, A. Knez, K. Klingenbeck-Regn, and M. F. Reiser, “Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience,” Radiology 217, 564–571 共2000兲. 26 V. R. Kini, S. S. Vedam, P. J. Keall, S. Patil, C. Chen, and R. Mohan, “Patient training in respiratory-gated radiotherapy,” Med. Dosim. 28, 7–11 共2003兲. 27 R. George, S. S. Vedam, T. D. Chung, V. Ramakrishnan, and P. J. Keall, Medical Physics, Vol. 33, No. 8, August 2006 2974 “The application of the sinusoidal model to lung cancer patient respiratory motion,” Med. Phys. 32, 2850–2861 共2005兲. 28 E. M. Leter, F. Cademartiri, P. C. Levendag, T. Flohr, H. Stam, and P. J. Nowak, “Four-dimensional multislice computed tomography for determination of respiratory lung tumor motion in conformal radiotherapy,” Int. J. Radiat. Oncol., Biol., Phys. 62, 888–892 共2005兲. 29 H. D. Kubo, P. M. Len, S. Minohara, and H. Mostafavi, “Breathingsynchronized radiotherapy program at the University of California Davis Cancer Center,” Med. Phys. 27, 346–353 共2000兲. 30 J. D. Hoisak, K. E. Sixel, R. Tirona, P. C. Cheung, and J. P. Pignol, “Correlation of lung tumor motion with external surrogate indicators of respiration,” Int. J. Radiat. Oncol., Biol., Phys. 60, 1298–1306 共2004兲. 31 C. Ozhasoglu and M. J. Murphy, “Issues in respiratory motion compensation during external-beam radiotherapy,” Int. J. Radiat. Oncol., Biol., Phys. 52, 1389–1399 共2002兲. 32 D. P. Gierga, G. T. Chen, J. H. Kung, M. Betke, J. Lombardi, and C. G. Willett, “Quantification of respiration-induced abdominal tumor motion and its impact on IMRT dose distributions,” Int. J. Radiat. Oncol., Biol., Phys. 58, 1584–1595 共2004兲. 33 G. C. Sharp, S. B. Jiang, S. Shimizu, and H. Shirato, “Prediction of respiratory tumour motion for real-time image-guided radiotherapy,” Phys. Med. Biol. 49, 425–440 共2004兲. 34 G. C. Sharp, D. Gierga, and S. B. Jiang, “Reliable real-time tracking in fluoroscopy for image guided radiotherapy,” Med. Phys. 31, 1758–1758 共abstract兲 共2004兲. 35 Y. Tsunashima, T. Sakae, Y. Shioyama, K. Kagei, T. Terunuma, A. Nohtomi, and Y. Akine, “Correlation between the respiratory waveform measured using a respiratory sensor and 3D tumor motion in gated radiotherapy,” Int. J. Radiat. Oncol., Biol., Phys. 60, 951–958 共2004兲. 36 Q. S. Chen, M. S. Weinhous, F. C. Deibel, J. P. Ciezki, and R. M. Macklis, “Fluoroscopic study of tumor motion due to breathing: facilitating precise radiation therapy for lung cancer patients,” Med. Phys. 28, 1850– 1856 共2001兲. 37 G. S. Mageras, E. Yorke, K. Rosenzweig, L. Braban, E. Keatley, E. Ford, S. A. Leibel, and C. C. Ling, “Fluoroscopic evaluation of diaphragmatic motion reduction with a respiratory gated radiotherapy system,” J. Appl. Clin. Med. Phys. 2, 191–200 共2001兲. 38 P. Parikh, J. Hubenschmidt, E. Vertatschitsch, S. Dimmer, J. Wright, and D. Low, “Dynamic accuracy of an implanted wireless AC electromagnetic sensor for guided radiation therapy: implications for real-time tumor position tracking,” Med. Phys. 32, 2112–2112 共abstract兲 共2005兲. 39 D. Low, J. Balter, J. Pouliot, G. Starkschall, K. Forster, L. Dong, E. Vertatschitsch, and J. N. Weight, “Dynamic accuracy of an AC magnetic 4D localization system prototype,” Med. Phys. 31, 1758–1758 共abstract兲 共2004兲.