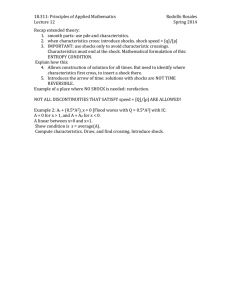
Fransthoracic Ventricular Defibrillatlon with Square-wave Stimuli: ONE-HALF CYCLE, )NE CYCLE, AND MULTICYCLE WAVEFORMS iy John C. Schuder, Ph.D., Harry Stoeckle, M.D., and Alfred M. Dolan, B.S.E.E. Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 • In 1960 Kouwenhoven, Jude, and Knickerbocker1 reported that adequate circulation of the blood could be achieved by means of closed chest cardiac massage. This technique is said to permit the oxygen demands of the myocardium to be satisfied by external means and thereby makes practical the utihzation of transthoracic electric shock for the reversal of ventricular fibrillation. However, Del Guerico et al.,- have observed low cardiac output in three patients undergoing external cardiac massage. Alexander et al.8 reported successful treatment of ventricular tachycardia by transthoracic electric shock in 1961. Their paper was followed by others, particularly from Lown's group *~° which described the successful use of transthoracic shock for terminating a variety of other cardiac arrhythmias. As a result of both these developments, the use of electric shocks applied by means of electrodes held on the surface of the chest has assumed an appreciably increased clinical importance in the treatment of cardiac arrhythmias. With this increased importance and use has come a renewal of interest in evaluating the effectiveness of different types of electric shocks in order to find the most satisfactory waveform. This interest has led to the development of several types of external defibrillators which deliver capacitor discharges. From the University of Missouri School of Medicine, Columbia, Missouri. Supported by a grant from the Life Insurance Medical Research Fund. Presented in part at the Thirty-sixth Scientific Sessions of the American Heart Association, October 25, 1963. Received for publication March 2, 1964. 258 One type, suggested by Kouwenhoven and Knickerbocker,7 uses capacitors charged to opposite polarities which are discharged in turn through a series circuit composed of an inductor and the patient. In another study, Lown and associates4" used a single capacitor which discharged through the chest via a series inductor. Peleska8 has published a detailed experimental study of the factors which cause certain types of capacitor discharges to "damage" the heart, as indicated by the observation that subsequent defibrillation was more difficult. Numerous other investigators have contributed also to our understanding of the use of capacitor discharges in the treatment of ventricular fibrillation.9'12 In addition to the various capacitor discharge systems, the 60 cycles/sec sinusoidal defibrillators described by Guyton and Satterfield13 and by Kouwenhoven's group14 continue to be employed. While the clinical results obtained with the presently utilized methods are most impressive, a systematic experimental evaluation of a wide variety of waveforms appears necessary if the most satisfactory type of shock is to be found. An almost endless variety of waveforms can be generated at low power levels with apparatus commercially available. The present paper describes a very high powered and rather specialized amplifier which accepts the output from the low level generators and makes the same waveforms available at the much higher levels required for transthoracic electric shock. This amplifier is being utilized for a systematic experimental study of the effectiveness of various square waves in the treatment of ventricular fibrillation. Circulation Rtsttrcb, Vol. XV, Stpfmbrr 1964 259 TRANSTHORACIC VENTRICULAR DEFIBRILLATION Methods SPECIAL EQUIPMENT Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 A block diagram of the equipment which is described in greater detail elsewhere,15 is shown in figure 1. The energy is stored in two 1,000 microfarad capacitor banks which are charged to opposite polarities. The stored energy is then released to the experimental animal in controlled fashion by means of two banks of power tubes. Each bank, consisting of 11 type 7094 beam power transmitting tubes, is capable of supplying over 10 amperes of current to the thorax of an animal. The control signals for the banks of power tubes are derived from a modulated radio frequency carrier which is inductively coupled into the high-power blocks and demodulated before being applied to the grids of the power tubes. The top bank of tubes conducts current which passes through the subject in one direction and the bottom bank conducts current which passes through the subject in the opposite direction. If current waveforms of only one polarity are desired, the two capacitor banks are operated in parallel and the two banks of tubes are also used in parallel. This mode of operation yields peak currents in excess of 20 amperes. When used on an animal with chest resistance of 60 ohms, 20 amperes correspond to a power of 24,000 watts. An important feature of the amplifier is that its output impedance is large in comparison to that of the chest. Hence, the amplifier tends to deliver a shock of predetermined current waveform and amplitude despite variations of chest impedance from animal to animal and despite changes of electrode-skin resistance from procedure to procedure on a given animal. In contrast to the results with low impedance sources, the power supplied to the chest increases with increasing chest impedance levels. In order that the amplifier may be used both to induce fibrillation and to terminate it, a manual selector switch (not shown on diagram) in the input circuit of the signal frequency amplifier allows the operator to pick one of three types of shock. The first of these is usually a low current 60 cycles/sec shock for the induction of fibrillation, the second is the waveform under investigation, and the third is a highly effective defibrillatory shock. The amplitudes and durations of each of these signals can be independently adjusted. A two-channel direct-writer is used for recording the slower current and voltage waveforms. Faster waveforms are displayed on a cathode-ray oscilloscope. + HV •2000 V 1000 pf POWER TUBES DEMODULATOR PATIENT ELECTRODES MODULATED AMPLIFIER POWER TUBES DEMODULATOR 1000 pf RADIO FREQUENCY OSCILLATOR SIGNAL FREOUENCY AMPLIFIER FROM LOW-LEVEL SIGNAL GENERATOR - 2000 V • -HV FIGURE 1 Block diagram of high powered amplifier used for transthoradc ventricular defibriUation. CircnUtion Rtsttrcb, Vol. XV, Sipumhtr 1964 SCHUDER, STOECKLE, DOLAN 260 PROCEDURE Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 Six dogs were used in two groups of three animals each to evaluate the effectiveness of any given waveform in the treatment of ventricular fibrillation. The first three animals were anesthetized with pentobarbital sodium injected intravenously at 27.5 mg/kg body weight. Sometimes additional anesthesia, up to 40% of the initial dose, was required during the procedure. The operating tables on which animals lay were equipped with rubber tips on the legs and insulating mats between the animal and the table. These precautions guaranteed that the current flowed between the two electrodes held on the chest and not through alternate paths to ground. The electrocardiograph cables, which were connected to the animals by means of needle electrodes inserted subcutaneously in the limbs, terminated in a junction box and a selector switch was used to choose the desired signal for display on a cathode-ray oscilloscope. The same selector switch served to isolate the animal from the oscilloscope during the actual shock. The first animal was given a low current shock (usually 60 cycles/sec, sinusoidal). Ventricular fibrillation typically followed the first shock; but if it did not, the shock was repeated until ventricular fibrillation occurred. After the onset of ventricular fibrillation, a 30-second waiting period was allowed to elapse before an attempt was made to defibrillate with the waveform under investigation. In the event that the initial attempt to defibrillate failed, a shock of known high effectiveness was utilized to salvage the animal. The 0.5 second and third animals were then treated in identical fashion. This rotational sequence was repeated until each animal had undergone 20 such procedures. If efforts to defibrillate an animal failed after several shocks with the follow-up waveform, external cardiac massage was used and the animal, whether surviving or dead, was replaced by another one for the remainder of the immediate experiment. After 60 procedures had been completed with the first group of animals, the experiment was repeated with the second group of three animals. In this way each waveform under investigation was evaluated on the basis of 120 trials. If defibrillation and an effective cardiac beat were achieved on the initial trial of any given procedure, it was tabulated as a successful defibrillation. Defibrillation at the second or later attempt was tabulated as a failure. Results Figure 2 illustrates the results of a study involving the effectiveness of a defibrillatory shock consisting of a one-half cycle unidirectional square current pulse. Since the family of curves is plotted from 26 points, and each point involves 120 trials, this figure summarizes data on 3,120 fibrillation-defibrillation episodes. Except for the 10-ampere and 50millisecond point, and the 5-ampere and 50millisecond point, both of which appear to be 4 8 16 32 DURATION IN MILLISECONDS 64 128 256 FIGURE 2 Relation between per cent success of ventricular defibrillation and duration of one-half-cycle unidirectional square-wave shocks. Circulation Runrcb, Vol. XV, Stpttmhtr 1964 261 TRANSTHORACIC VENTRICULAR DEFIBRILLATION 100 90 80 i 10 AMPERES/ 70 $60 LLJ § 50 Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 1-40 z o 30 cc UJ20 / 10 - J <6 I I 0 / \ -OR 0.5 J ~| T 10 Amperes 1 1 / 1 | 4 8 1 2 DURATION IN MILLISECONDS 1 16 32 64 128 FIGURE 3 Relation between per cent success of ventricular defibrillation and duration of ten-ampere one-half-cycle unidirectional and of ten-ampere one-cycle bidirectional shocks. abnormally depressed, the data yielded relatively smooth curves of effectiveness as a function of pulse duration. Figures 3 and 4 compare results obtained with one-half cycle unidirectional shocks and those obtained with one-cycle bidirectional shocks. Figure 3 presents the results for 10ampere shocks and figure 4 the results for 5-ampere shocks. In this particular experiment the one-cycle waveform was obtained by closing an electronic switch, and thereby connecting a square wave generator to the 100 90 80 = 70 u. c/)60 no J I 5 AMPERES • LJ l o50 • 5 30 \ - \ 5 AMPERES I £20 Q_ - 10 0 * .05 2 4 8 16 DURATION IN MILLISECONDS 32 . 64 — : — * 128 256 FIGURE 4 Relation between per cent success of ventricular defibrillation and duration of five-ampere one-half-cycle unidirectional and of five-ampere one-cycle bidirectional shocks. CircnUsion Ruttrcb, Vol. XV, Stpumitr 1964 262 SCHUDER, STOECKLE, DOLAN Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 ampHfier for a time period equivalent to one cycle of the square wave. Because the instant of closing the switch was arbitrary, the exact waveform varied from trial to trial. Two of the possible waveforms are illustrated in the figures. An important feature of the onecycle bidirectional shock is that, despite the arbitrary starting point, the net electrical charge transport is zero. As in figure 2, the points corresponding to a 50-millisecond shock duration seem to be abnormally depressed. Figure 5 illustrates the results for multicycle square-wave shocks. Their duration was fixed at 128 milliseconds and their amplitude at 5 amperes for all shocks. The independent variable is the fundamental frequency of the square wave and this is plotted along the abscissa. Since there is a one-to-one correspondence between frequency and the number of cycles in any fixed duration shock, the number of cycles in the shock is also plotted along the abscissa. Discussion Limitations of the frequency response of our apparatus tended to introduce appreciable distortion in one-half cycle unidirectional shocks equal to or less than one millisecond, in one-cycle bidirectional shocks equal to or less than four milliseconds, and in multicycle shocks at frequencies equal to or greater than 250 cycles/sec. Consequently, some distortion in waveform is observed for shocks represented by points at the far left of the curves in figures 2, 3, and 4 and for the point furthest to the right in the curve of figure 5. The 20-ampere curve of figure 2 has a peak effectiveness of almost 100% for a duration of 4 milliseconds. The 10-ampere curve has a similar peak value of effectiveness for a duration of approximately 16 milliseconds. Since the energy in joules introduced into the chest (which is primarily resistive in nature) is given by PRt where 1 is the current in am- 100 90 80 co Seo : ~u U "1 Lr •5 AMPERES 0.128 SEC —*| w 50 40 U a: 30 UJ Q. 10 0.5 I 4 8 2 4 8 16 TOTAL NUMBER OF CYCLES 16 32 64 128 32 256 FREQUENCY IN CYCLES PER SECOND FIGURE 5 Relation between per cent success of ventricular defibrillatum and frequency for 128-millisecond fioe-ampere square-waoe shocks. Circnl^ion Rtsttrcb, Vol. XV, September 1964 263 TRANSTHORACIC VENTRICULAR DEFIBRILLATION Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 peres, R the resistance in ohms, and t the duration in seconds, it is apparent that the most effective 10-ampere shock and the most effective 20-ampere shock have about the same energy content. For a chest resistance of 60 ohms this energy is 96 joules. All the curves of figure 2 demonstrate that for a given amplitude of current there is an optimal duration, and that shocks which are longer than this optimum are less effective. It is our distinct impression that, while shocks with durations less than that corresponding to peak effectiveness usually produce a prompt return to a normal sinus rhythm when defibrillation is achieved, those of greater durations often produce transitory severe arrhythmias. The curves are generally, but not exactly, compatible with the hypothesis that the effectiveness of a shock is a function only of its energy content provided the level of current is above a certain value. Thus in figure 2 if the 20-ampere curve were to be translated horizontally to the right by multiplying its abscissa values by four, it would coincide approximately with the 10-ampere curve over only a limited range. The 5-ampere curve, regardless of energy content, never yields a very high level of effectiveness. Perhaps the most striking feature of the curves of figures 3 and 4 is the apparent broadening of the range of high effectiveness for the bidirectional shocks as compared to the corresponding unidirectional shocks of the same duration and energy content. For both the 5-ampere and the 10-ampere shocks, one finds that the bidirectional waveform continues to be very effective at durations for which the effectiveness of the corresponding unidirectional pulses is noticeably reduced. It is again our impression that the arrhythmias associated with the longer unidirectional pulses are much more severe than those occurring when the bidirectional shocks of the same duration are utilized. It appears that the values of peak effectiveness for given current levels are almost identical for both unidirectional and bidirectional shocks. Since frequency is the independent variable for the curve of figure 5, and shock Cinnlmtiom Research, Vol. XV, September 1964 amplitude and duration are fixed, the energy content is the same for all shocks. While the results indicate very low effectiveness for both extremes of frequency, the curve shows a maximal effectiveness of about 70%. It is interesting that this maximum is similar to that observed for both the most effective 5-ampere one-half-cycle unidirectional shock and the most effective 5-ampere one-cycle bidirectional shock. The rather low effectiveness found at 256 cycles/sec differs from the results observed by Crowley et al.10 for internal defibrillation. Summary A very high powered amplifier for experimental transthoracic ventricular defibrillation has been described. The effectiveness of both one-half-cycle unidirectional and one-cycle bidirectional square waves in terminating ventricular fibrillation first increases, then reaches a maximum and finally decreases as the duration of the shock is increased. With 10- and 20-ampere unidirectional shocks and 10-ampere bidirectional shocks, a maximal effectiveness of substantially 100% was found under the chosen experimental conditions. Five-ampere unidirectional and bidirectional shocks yielded maximal effectiveness of 70%. The effectiveness of a 128-millisecond, 5-ampere, multicycle square-wave shock is a strong function of frequency and has a maximal value of approximately 70%. Acknowledgment The authors express appreciation to James K. West for constructing the apparatus and to Carl F. Ehrlich, Jr., Shan Lin Hou, B. J. McClatchey, and Jerry D. Benedict for extensive assistance with the experimental procedure. References 1. KOUWENHOVEN, W. B., JuDE, J. R., AND KNICKERBOCKER, G. G.: Closed-chest cardiac massage. J. Am. Med. Assoc. 173: 1064, 1960. 2. DEL GUERICO, L. R. M., COOMARASWAMY, R. P., AND STATE, D.: Cardiac output and other hemodynamic variables during external cardiac massage in man. New Engl. J. Med. 269: 1398, 1963. 3. ALEXANDER, S., RLETCER, R., AND LOWN, B.: Use of external electric countershock in the treat- 264 SCHUDER, STOECKLE, DOLAN ment of ventricular tachycardia. J. Am. Med. Assoc. 177: 916, 1961. 4. 5. 6. LOWN, B., NEUMAN, J., AMARASINCHAM, R., AND 11. GURVICH, N. L., AND YUNIEV, G. S.: Restoration BERKOVITS, B. V.: Comparison of alternating current with direct current electroshock across the closed chest Am. J. Cardiol. 10: 223, 1962. of heart rhythm during fibrillation by a condenser discharge. Am. Rev. Soviet Med. 4: 252, 1947. LOWN, B., AMARASINCHAM, R., AND NEUMAN, 12. WECRIA, R., AND WICCERS, C. J.: Factors deter- J.: New method of terminating cardiac arrhythmias. J. Am. Med. Assoc. 182: 548, 1962. LOWN, B., PERLROTH, M. G., KATDBEY, S., ABE, mining the production of ventricular fibrillation by direct currents. Am. J. Physiol. 131: 104, 1940. T., AND HARKEN, D. E.: "Cardioversion" of 13. GUYTON, A. C , AND SATTERFIELD, J.: Factors atrial fibrillation. New Engl. J. Med. 269: 325, 1963. 7. KOUWENHOVEN, concerned in electrical defibrillation of heart particularly through unopened chest. Am. J. Physiol. 167: 81, 1951. W . B . , AND KNICKERBOCKER, Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 G. G.: The development of a portable defibrillator. Trans. Am. Inst. Elec. Engr. part 3. 81: 428, 1962. 8. PELESKA, B.: Cardiac arrhythmias following condenser discharges and their dependence upon strength of current and phase of cardiac cycle. Circulation Res. 13: 21, 1963. 9. MACKAY, R. S., AND LEEDS, S. E.: Physiological effects of condenser discharges with application to tissue stimulation and ventricular defibrillation. IRE Trans. Med. Electron. ME-7: 104, 1960. 10. of regular rhythm in mammalian fibrillating heart. Am. Rev. Soviet Med. 3: 236, 1946. GURVICH, N. L., AND YUNIEV, G. S.: Restoration 14. KOUWENHOVEN, W. B., MlLNOR, W. R., KNICKERBOCKER, G. G., AND CHESNUT, W. R.: Closed chest defibrillation of the heart. Surgery 42: 550, 1957. 15. SCHUDER, J. C , STOECKLE, H., WEST, J. K., AND DOLAN, A. M.: A very high power amplifier for experimental external defibrillation. Proc. 16th Ann. Conf. Engr. Med. Biol. Baltimore, Conference Committee, 5: 40, 1963. 16. COWLET, R. A., TISCHLER, M., ATTAR, S., AND TAMRES, A.: Cardiac defibrillation above 60 cycles with a portable square-wave defibrillator. Surgery 51: 207, 1962. Circuliion RtHtrcb, Vol. XV, Stpttmber 1964 Transthoracic Ventricular Defibrillation with Square-wave Stimuli: One-Half Cycle, One Cycle, and Multicycle Waveforms JOHN C. SCHUDER, HARRY STOECKLE and ALFRED M. DOLAN Downloaded from http://circres.ahajournals.org/ by guest on September 29, 2016 Circ Res. 1964;15:258-264 doi: 10.1161/01.RES.15.3.258 Circulation Research is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231 Copyright © 1964 American Heart Association, Inc. All rights reserved. Print ISSN: 0009-7330. Online ISSN: 1524-4571 The online version of this article, along with updated information and services, is located on the World Wide Web at: http://circres.ahajournals.org/content/15/3/258 Permissions: Requests for permissions to reproduce figures, tables, or portions of articles originally published in Circulation Research can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office. Once the online version of the published article for which permission is being requested is located, click Request Permissions in the middle column of the Web page under Services. Further information about this process is available in the Permissions and Rights Question and Answer document. Reprints: Information about reprints can be found online at: http://www.lww.com/reprints Subscriptions: Information about subscribing to Circulation Research is online at: http://circres.ahajournals.org//subscriptions/
 0
0
advertisement



Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users