-4 Application for Employer Identification Number
advertisement

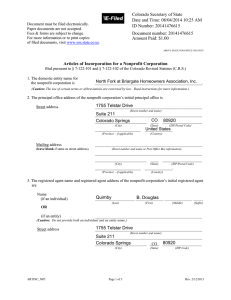
Form CSBS-4 Application Center for Simulated Business Services 1. Name of applicant (Legal name) for Employer Identification Number Keep a copy for your records 2. Trade name of business (if different from name on line 1) 3. Mailing address (street address) (room, or suite no.) 4. City, state, and ZIP code 5. County and state where business is located 6. Name of principal officer 7. Type of entity (check only one box Sole proprietor (SSN ) Personal service corporation Partnership 8. Other corporation (specify) Reason for applying (Check one box) Started new business Hired employees Banking purpose Purchased going business 9. Date business started or acquired (Mo., day, year) 11. First date wages were or will be paid EIN_NUM03 10. Closing month of accounting year (Mo., day., year) 12. To whom are most of the products or services sold? Public (retail) Other (specify) Signature (Type name and Title) EIN Business (wholesale) Telephone number Fax number