Geriatric Care and Financing in the United States
advertisement

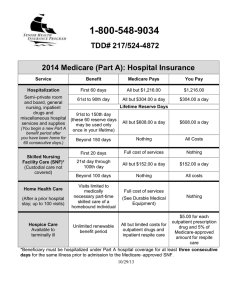
Geriatric Care and Financing in the United States Prepared by: Joseph G. Ouslander, M.D. Professor and Senior Associate Dean for Geriatric Programs Charles E. Schmidt College of Medicine Professor (Courtesy), Christine E. Lynn College of Nursing Florida Atlantic University Learning Objectives 1. Define different settings of care for older people, including home care, assisted living, SNF, and continuing care retirement communities 2. Compare financing of health services in different settings, in particular what Medicare does and does not pay for, and the role of Medicaid 3. Identify challenges and patient safety issues related to transitions between care settings 4. Discuss potentially effective models of care for older patients and their relevance to health care reform 5. Recognize opportunities to work as a physician in various geriatric care settings J. Ouslander, MD Page 1 Overview of Geriatric Care Financing Federal and state health care financing in the U.S. is overseen by the Center for Medicare and Medicaid Services (CMS; www.cms.gov) Most care for the elderly in the U.S. is financed by Medicare (www.medicare.gov ), a federal program that is predominantly for people older than 64. Younger people with end-stage renal disease or certain other medical disabilities may qualify. Medicare has four parts: o o o o The majority of Americans are covered by Medicare through the “fee-for-service” system. The percentage of people who enroll in Medicare managed care programs (Medicare Part Advantage plans) varies throughout the country, but is less than 40% in most states. o Medicare Part A – finances inpatient hospital care, post-acute skilled care, home care, and hospice care. All Medicare beneficiaries get Medicare Part A. Medicare Part B – finances outpatient care, including physician fees (for both outpatient and inpatient care), laboratory, and rehabilitation services. People have to elect to have Part B (most do) and pay a monthly fee for it. Medicare Part B also covers certain preventive services, such as flu shots, mammograms, and bone density testing. Medicare Part C – also called “Medicare Advantage” – is a managed care option that individuals can elect to participate in. Medicare Part D - is the new prescription benefit program that is also elective. In the fee-for-service system, there are deductibles and co-payments, which can result in substantial out-of-pocket expenditures. Many older people have supplemental insurance (e.g. Blue Cross/Blue Shield) that helps reimburse these additional costs. Until 2006, Medicare did not pay for outpatient prescription medications. Now, Medicare beneficiaries can elect Medicare Part D, which is administered by many different private “Prescription Drug Plans” (PDPs). o o Individuals may elect to continue their own insurance companies if their coverage is as good as Medicare Part D. Each PDP has its own formulary, which is required to pay for some medications in each major class of drugs. Patients can elect “second-tier” and “third-tier” drugs, but must pay substantial co-payments for them. Some elderly people (or their spouses) do not qualify for Medicare because they have not put enough tax dollars into the Medicare program. These people may be poor enough to qualify for Medicaid (below), but many slip through the cracks, and are cared for by government funded county hospitals. Many elderly people are poor enough to qualify for Medicaid, a government program for the poor that is financed by both state and federal funds. Each state has its own Medicaid program, and the covered health care services vary from state to state. o The majority of older people on Medicaid also have Medicare. They are generally referred to as “dual eligibles”, and may qualify for state programs designed to prevent unnecessary hospitalizations and nursing home placement. J. Ouslander, MD 2 July, 2011 Settings of Care Home Care Most care in the home for older people with chronic illnesses and functional disability is provided by family and informal caregivers. Medicare does not pay for care that only provides assistance with activities of daily living. o Medicare will cover skilled home care services if nursing or rehabilitation therapy is necessary. This payment is time-limited, and requires the patient to be “homebound”. It is usually, but not necessarily linked to a hospitalization. Medicare home health care is reimbursed on a prospective (as opposed to feefor-service) based system, which is derived from a comprehensive assessment – the Outcome & Assessment Information Set (OASIS) o Medicare will also cover home visits by physicians and nurse practitioners. o In-home assistance with activities of daily living and other caregiver services are available from a variety of agencies. Geriatric care management services are available to help coordinate services All of these services are paid for out of pocket, unless the person has long-term care insurance (which often provides limited coverage) or is poor enough to qualify for Medicaid Medicaid provides a variety of community services directed at avoiding the need for institutional care. Local Area Agencies on Aging are involved in screening and eligibility for these services, and help with access to them. (See for example http://www.myanswersonaging.org/content.asp?id=4 for the Palm Beach County agency. Outpatient Clinic Care Outpatient care, including physician fees, diagnostic tests, and rehabilitation are covered by Medicare Part B (for those who elect it), supplemental insurance, and/or out-of-pocket. Acute Hospital Care There are four types of acute hospitals that provide care to older patients – general acute care hospitals, acute rehabilitation hospitals, long-term acute care hospitals, and psychiatric hospitals. The Veterans Administration has over 100 acute care hospitals; most are affiliated with medical schools where older Veterans can be admitted, and there are many publicly funded hospitals (e.g. county hospitals) that serve a predominantly indigent population. Acute Hospital care is funded by Medicare Part A for those older people who have Medicare o All acute hospital care, including medical, surgical, psychiatric, rehabilitation, and “longterm acute care” is now reimbursed by a prospective payment system in which the hospital gets a fixed amount per day or a fixed amount for the hospital stay. J. Ouslander, MD 3 July, 2011 o For medical and surgical care in an acute care hospital, payment is determined by a “Diagnosis Related Group” (“DRG”). There are over 400 DRGs, and many of them have additional payments for complications. Medicare is, however, now limiting additional payments for certain complications (“never events”). The average length of stay in for older patients in Acute Care hospitals in the U.S. varies, but is generally between 4 and 6 days. 75% of patients admitted to Acute Rehabilitation Hospitals have to fit into one of approximately 10 diagnoses (e.g. hip fracture, stroke). Long-term Acute Care (LTAC) hospitals are available in most states. The average length of stay in these units must be at least 25 days, but total payment for the stay is capped. Patients in these hospitals are generally being weaned from respirators, or have complex wounds or osteomyelitis requiring long-term antibiotics. There are relatively few Psychiatric Hospitals that exclusively care for geriatric patients because of Medicare funding limitations. Older patients with acute psychiatric needs are therefore often treated in general acute psychiatric facilities along with younger patients with mental illness. Post-Acute Skilled Nursing Facility (SNF) Care (commonly referred to as “Rehab”) The majority of older people and their families believe that Medicare will pay for SNF care. This is not the case. A SNF usually includes one or more units for short-stay post-acute care patients, and other units for long-stay residents of the facility. Individuals who have Medicare Part A benefits may qualify for reimbursement for a stay in a skilled nursing facility (SNF) after an acute hospitalization of at least 3 days. Unless the person is in a Medicare managed care program (e.g. Humana is the largest in Florida), a person must be in an acute hospital for 72 hours on an inpatient (not observation) status in order to qualify for Medicare Part A coverage in a SNF. o In order to qualify, the patient must need 24-hour nursing care, frequent physician visits, and/or rehabilitation to achieve a higher functional status. All SNF services(including medications) are covered by Medicare Part A except physician fees (which are covered by Medicare Part B, private insurance, out-of-pocket, or Medicaid). The SNF is reimbursed a daily rate based on “Resource Utilization Groups” (RUGs), which are calculated from a comprehensive assessment - the Minimum Data Set (MDS). Medicare Part A reimbursement for an SNF stay is limited to the time during which the patient qualifies for skilled care. Once they are determined to not need skilled care and/or have made maximum progress in rehabilitation, payment for care reverts to private pay or Medicaid. o The average length of a Medicare skilled stay is about 25 - 30 days, but Medicare will theoretically pay for up to 100 days per illness episode. J. Ouslander, MD 4 July, 2011 Long-Term Nursing Home Care Long-term care in a nursing home (the vast majority of nursing homes are also qualified as SNFs) is paid for out-of-pocket, unless the individual is poor enough to qualify for Medicaid, in which case Medicaid pays. o o o Good nursing homes cost $4,000 -$5,000 or more per month. Medicaid pays nursing homes much less than that in most states. Some people have long-term care insurance, but benefits are usually very limited. The Veterans Administration has over 100 nursing homes, and also places older Veterans who qualify in state Veterans homes as well as in community nursing homes that are under contract. o The total number of Veterans served by these programs is limited by the eligibility criteria; less than 100,000 Veterans benefit by these programs in the U.S., compared to a nursing home population of over 1.5 million. Assisted Living Facilities (ALFs) ALFs vary considerably in size and scope of services. Although residents generally have to be independent, many people “age in place” – thus some residents of ALFs are medically and functionally similar to long-stay nursing home residents. Generally there is very limited presence of nurses and physicians in ALFs. Medicare does not pay for ALF care. Some state Medicaid programs support ALF care. o Residents generally pay out-of-pocket, and the fees are graduated based on level of care needs (e.g. medication assistance may cost extra) Continuing Care Retirement Communities (CCRCs) CCRCs generally include independent living, assisted living, and skilled nursing care. Residents buy in by purchasing an independent living unit, and pay a monthly fee, and generally live at the CCRC for the rest of their lives. Many CCRCs are very upscale, and include a wide variety of services and activities for their residents. Hospice Care Medicare will pay for hospice care for patients who have a life expectancy of less than 6 months. The payment rules are complicated. Patients must qualify, and elect to enroll in a hospice program. The vast majority of hospice care is provided in the patients’ homes. There are a limited number of inpatient hospices for acute symptom management, and some patients receive hospice care while in a nursing home. J. Ouslander, MD 5 July, 2011 Transitions Between Care Settings Care transitions for geriatric patients are now a major focus of attention nationally; transitions between the acute hospital and home or to a SNF are the major focus. o 1 in 5 acute care hospitalizations of Medicare fee-for-service patients are associated with a hospital readmission within 30 days; and 1 in 4 admissions to a SNF are associated with a hospital readmission within 30 days. These admissions are costly, fraught with risks of iatrogenic illness and hospitalrelated complications, and result in billions of dollars in unnecessary health care expenditures. Current financial incentives in the Medicare-fee-for-service system favor hospitalization. o Medicare is going to be testing and implementing new payment methods that reduce these incentives through the new Center for Medicare Innovation (established as a major component of the Accountable Care Act (the “health care reform act”). o These changes in financing will drive the development of new models of care and financing that provide opportunities for coordinated, high quality, and efficient care for the growing geriatric population. Examples of payment reforms include: o Pay-for-Performance (“P4P”) Physician offices Hospitals, SNFs, Home Care Agencies (no payment for certain complications; disincentives for avoidable hospitalizations) o Payment for care coordination (e.g. the “Medical Home”) o Creation of Accountable Care Organizations that include hospitals, physicians, home health agencies, and SNFs who are responsible for the care of a defined group of patients o Bundling of payments for episodes of care There are a variety of resources available to improve care transitions o http://interact2.net is a website that contains tools for SNFs to improve care and reduce unnecessary hospitalizations J. Ouslander, MD Several other websites can be located by clicking “Care Transition Resources” on the top banner of http://interact2.net 6 July, 2011 Innovative Models of Geriatric Care The Medicare fee-for-service system as it exists today is not sustainable. It must change, or there will not be enough money for future generations to have adequate Medicare benefits. The fee-for-service Medicare system financially incentivizes tests, procedures, hospitalization, and technology – i.e. in general, the more you do for patients, the more you get paid. o More care is not always better care Interventions can often do more harm than good in elderly patients, and can result in unnecessary morbidity and health care expenditures Several innovative models for geriatric care have been developed and tested, and shown promise for improving care and reducing unnecessary health care expenditures. Examples include: o The Program for All Inclusive Care of the Elderly (PACE) mixes Medicare and Medicaid support to keep frail elderly out of nursing homes and hospitals. (http://www.npaonline.org) o Evercare is a managed care program for long-stay nursing home residents designed to minimize the use of acute hospital and other expensive care (http://evercarehealthplans.com ) o The Geriatric Resources for Assessment and Care of Elders (GRACE) model of primary care for low-income seniors and their primary care physicians (PCPs) was developed to improve the quality of geriatric care to optimize health and functional status, decrease excess healthcare use, and prevent long-term nursing home placement (http://medicine.iupui.edu/IUCAR/research/grace.asp ) o The Transitional Care Model (TCM) provides comprehensive in-hospital planning and home follow-up for chronically ill high-risk older adults hospitalized for common medical and surgical conditions (http://www.transitionalcare.info/Abou-1783.html) o Guided Care™ is a new solution to the growing challenge of caring for older adults with chronic conditions and complex health needs. A Guided Care Nurse, based in a primary care office, works with patients and their families to improve their quality of life and make more efficient use of health services. The nurse assesses patient needs, monitors conditions, educates and empowers the patient, and works with community agencies to ensure that the patient’s healthcare goals are met (http://www.guidedcare.org/index.asp ) J. Ouslander, MD 7 July, 2011