2015 Care Rights Report for the Survey
advertisement

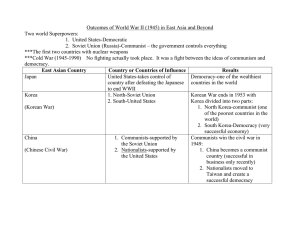
CARE RIGHTS SURVEY 1 2015 Care Rights Report for the Survey Question 1: What is the role of your organization? Do you participate in MIPAA implementation or monitoring thereof? 1.1. Care Rights Mission and Goals Care Rights aims to protect and advocate for elderly patients’ rights during the process of their end-of-life care and decision making(EOLCD). At the core of our mission is our desire to safeguard not only the elderly patients’ but also their caregivers’ and families’ autonomy, independence and dignity. Care Rights works to address a ‘normative gap’, known as the lack of protection for older person's rights through the existing human rights system, and promotes an ‘implementation gap’, known as the lack of provision in international law, health care policy, and immigration law for their autonomy and wellbeing in the process of EOL care and decision. Under the mission, Care Rights sets the three goals. First goal is to educate and support elderly patients, family caregivers, and their loved ones to build social and cultural support systems in EOL care and decision. The second one is to promote and facilitate opportunities for legal action in the context of elderly patients’ rights in EOL care and decisions under the principle of human rights. The third one is to raise public and professional awareness of human rights in regards to one’s EOL care and decision, as well as for the protection of elderly caregivers by spouses and partners. 1.2. Programs and Activities Care Rights runs five activities to administer our goals : Education & Counseling Program Enactment & Advocacy Program UN Activities Survey & Research Program Hospice Camp for Diaspora Community 1.3. MIPPA & Principles Our operating principles are in alignment with those outlined in the Madrid International Plan of Action Ageing (MIPAA)that all the elderly ought to be free from discrimination, isolation, and inequality, especially as they CARE RIGHTS SURVEY 2 navigate the often painful and isolating experience of EOL care and decision. Figure 1 shows the items for older person's rights that were outlined from the MIPPA. Figure 1. The Items for Older Person's Rights that were Outlined from the MIPPA 59. The World Health Organization defines health as a state of complete physical, mental and social well-being, not merely the absence of disease and infirmity... 61. The growing need for care and treatment of an ageing population requires adequate policies. The absence of such policies can cause major cost increases... 69. Investing in health care and rehabilitation for older persons extends their healthy and active years. The ultimate goal is a continuum of care ranging from health promotion and disease prevention to the provision of primary health care, acute care treatment, rehabilitation, community care for chronic health problems, physical and mental rehabilitation for older persons including older persons with disabilities and palliative care for older persons suffering painful or incurable illness or disease... Section for Advancing health care and well-being into old age 76. Objective 3: Development of a continuum of health care to meet the needs of older persons. Actions (d) Support the provision of palliative care and its integration into comprehensive health care. To this end, develop standards for training and palliative care and encourage multidisciplinary approaches for all service providers of palliative care; 86. Objective 1: Development of comprehensive mental health-care services ranging from prevention to early intervention, the provision of treatment services and the management of mental health problems in older persons. Actions (c) Provide programs to help persons with Alzheimer’s disease and mental illness due to other sources of dementia to be able to live at home for as long as possible and to respond to their health needs; CARE RIGHTS SURVEY 3 Question 2: Has a human rights-based approach been integrated in the implementation framework of MIPAA in your country and if so, how did this translate into concrete policies and normative actions? Are there any mechanisms to monitor and assess the impact of MIPAA implementation on the enjoyment of all human rights by older persons? 2.1. Human rights implementation framework South Korea has developed and operated multiple social policies and actions in the implementation framework of MIPAA including social security policy, health care policy, and human right policy for older persons as below1: A. Social security policy : Basic pension to older persons. The nation requires citizens to subscribe to 4 compulsory social insurances by law. Secure income, medical treatment, rehabilitation, and employment opportunity as a social safeguard against disease, disability, old age, death, and unemployment. Four types of Social Insurances are : Health insurance, National Pension, Industrial Accident Compensation Insurance, and Unemployment Insurance. B. Health care policy The nation requires citizens to subscribe to 4 compulsory health security systems. National Health Insurance Program, Medical Aid Program, Long-Term Care Insurance Program and Health Insurance System. However, the report of the Korea National Human Rights Commission (2009) found that Korean elderly is not properly guaranteed their rights for basic income, residential security, unemployment, retirement benefit, health care coverage as well as social activities2. Figure 2 shows the status of the poverty rates by age group. Figure 2. Relative Poverty Rates by Age Group (South Korea) 1 2 National Health Insurance Service, http://www.nhis.or.kr/static/html/wbd/g/a/wbdga0301.html National Human Rights Commission of Korea, 2009, https://library.humanrights.go.kr/hermes/web.search.Search.ex?command=SearchDetailGet, http://library.humanrights.go.kr/hermes/imgview/10-04.pdf CARE RIGHTS SURVEY 4 2.2. Poverty and Suicide Rate First of all, both poverty and suicide rate are the highest among OECD member countries. The poverty rate of older people (65+) is the highest in OECD area. According to figure 2, overall the poverty rate over age 65 increases rapidly. Especially the poverty rate of those above75 increased compared to 2006 and 2011. The poverty rate of the group at 2011 is higher than 2006.3 The suicide rate of Korean elderly population is the highest compared to other age groups. According to national survey(2014), 10.9% of older people have thought about suicide among 60 years and older. Around 12.5% said they actually had tried. They wanted to commit suicide because of economic difficulty(40.4%), health problems(24.4) and etc.4 Especially, some elderly in the community would decide to commit suicide due to severe physical and emotional pain in end stage of life without fully developed emerging services such as inpatient and home-based palliative and hospice care services.(Chang, 2013) 2.3. End of Life Care and Decision World Health Organization(WHO) reported that 56 million deaths occurred worldwide during 2012. Of these, 38 million were due to Non Communicable Diseases (NCDs) between 2000- 2012 principally cardiovascular diseases, cancer and chronic respiratory diseases. In S. Korea 266,000 of total death, 89.2% of older persons have NCDs. 79% of total death accounted with NCDs.5 According to the national survey for older person's life and status (2014), 43.7% of them rate their overall state of health is not good, 32.4% of them rate it is good. Most of caregivers are their family members. In these 3 OECD, OECD Economic Surveys: Korea 2014, http://www.oecd-ilibrary.org/economics/oecd-economic- surveys-korea-2014_eco_surveys-kor-2014-en 4 The Ministry of Health and Welfare, 2014 research on actual condition of aged, http://www.prism.go.kr/homepage/researchCommon/retrieveResearchDetailPopup.do?research_id=1351000201500109 5 WHO, Noncommunicable diseases country profiles 2014, http://www.who.int/nmh/publications/ncd-profiles- 2014/en/ CARE RIGHTS SURVEY 5 survey, subjects were asked about what their preference is for end-of-life care and decision.6 A. Violation of Older Person's Autonomy in EOL care and decision(EOLCD). From a human rights perspective, the elderly patients’ autonomy regarding EOLCD is an essential part of human well-being. They must be informed about the clarification for diagnosis and treatment options, and respected in consideration of their values, goals, and wishes in their end of life care. The right for the elderly to make decisions regarding the type and extent of treatments during final life stages is drawn from guidelines prepared by the Council of Europe that state “Older persons should receive medical care only upon their free and informed consent and may also freely withdraw consent at any time.” (Council of Europe, Recommendation CM/Rec(2014)2, 2014). From a human rights perspective, therefore the elderly patients’ autonomy regarding EOLCD is an essential part of human well-being. The UN principles for older persons indicates that the government should completely guarantee older people’s dignity, faith, desire and privacy. It indicated that especially protecting dignity is greatly important and protecting their self-dignity is also important. According to 7research of older persons’ status in 2014, 88.9% of subjects are against life sustaining treatment in the condition of non-treatable. However the legislation is yet not established and older persons’ preferences are not fully supported. B. Under-developed Infra system for EOLCD When we compared welfare facility program in S. Korea to ombudsman of America, right for self determination is not in the program. Right for self determination is the right to choose doctors, right to participate in care, treatment, related changes and right to be informed about them. “Recommendation for EOLCD”,which was decided by Korea National Institute for Bioethics Council, shows ‘all patients have right to know their illness, progress of sickness, treatment that will be conducted, and right to decide for themselves. Also it accentuated active establishment of systems by government and society, in order to let patients freely choose hospice & palliative care. The recommendation targets patients who are non-treatable, aggravating dramatically, and in end stage of life. At present, a legislative bill regarding “Hospice & Palliative Care Act” is under examination. 8 The purpose of the draft is to expand the targets of hospice service, which is currently limited to cancer patients. On the other hand, legislative law related to offering comprehensive care to those in end of life stage, and their family is under examination.9 At the same time, a draft that supplemented “the counsel” is also under examination. It says if there were no Advance Medical Directives, estimating the mind of patients 6 The Ministry of Health and Welfare, The survey for older person's life and condition 2014, http://www.prism.go.kr/homepage/researchCommon/retrieveResearchDetailPopup.do?research_id=1351000201500109This research is conducted in every 3 years 7 8 The Ministry of Health and Welfare, The survey for older person's life and condition 2014, op. cit. The National Assembly of the Republic of Korea, a draft related to hospice & palliative care, bill number 1914991,http://likms.assembly.go.kr/bill/jsp/BillDetail.jsp?bill_id=PRC_F1L5E0A4S3M0R1G8A1L6B5Y9Q4 N8E3 9 The National Assembly of the Republic of Korea, Draft regarding the use of hospice & palliative care and end- of-life-stage patient’s decision making on life sustaining treatment, 2015,http://likms.assembly.go.kr/bill/jsp/BillDetail.jsp?bill_id=PRC_M1K5N0R7R0U7S1B5X0F4S5C8Y9Z8K 5 CARE RIGHTS SURVEY 6 should be available. Also it suggests patients who are non-treatable and in end stage of life, should freely want and request hospice & palliative care. However, National Human Rights Commission of Korea recommends arranging a standard long-term care service but it's not established nor enacted.10 Also Figure 3 shows that there are very short of numbers of beds and facilities. To make matters worse, government supplementary subsidy is also not enough. Consequently Korea's hospice facilities is deteriorated and limited. Furthermore Korea’s guideline is not sufficient to guarantee patient’s neither self-determination nor autonomy of advanced medical directives.11 In result, 62.6% of advanced demented, older patients end their life in a nursing home in the U.S.; however, only 5.5% of Korean elderly patients end their life in a nursing facility compared to 73.6% of elderly patients receiving acute hospital care in South Korea (J of American Health Care Administration, 2015) Figure 3. The Status of Hospice Services in South Korea12 Management by Administration Number of Facilities Number of Beds Public Health Care Organization 12 209 Designated Hospice Organization 2 31 Regional Cancer Organization 12 154 Religious Hospice Organization 25 440 3 32 Hospice Unit by Private Medical Center C. Monitor Mechanism In current, there are a few monitor mechanisms to observe the disparities for the older persons' human rights including governmental institution for Human Rights Commission of Korea and civic organizations such as Helpage Korea and CareRights, Kakdang 13 social welfare foundation, and 14 Korean Initiative for Advance Directive. Kakdang runs rainbow hospice program. Care Rights mainly concerns in guaranteeing self determination, developing standards and protocols, and also offers education and counseling for older persons and participates in enacting progress by public hearing. Figure 4 shows the recent tragic cases resulting from those lack of legislation and monitoring mechanism for health care setting in S. Korea. According to Han's studies, there are no regulations 10 150224 Press Release: recommendation for protecting human rights for users of Elderly Medical Welfare Facility 11 refer appendix 12 Family Experiences of End of Life Care Decisions for Elderly Patients in South Korea, Soo Han, Tae Hyun Kim 13 Care Rights, http;//www.carerights.org, http://www.kakdang.or.kr/ 14 KAKDANG Korean Initiative for Advance Directive, http://www.sasilmo.net/ SOCIAL WELFARE FOUNDATION, CARE RIGHTS SURVEY 7 and guidelines for social worker's engagement of the process of EOLCD for older patients and their family caregivers.15 15 Han, S. (2015a). "A Study of Social Worker' Understanding of Elderly Patients' and Family Caregivers' Rights to End-of-Life Care Decisions and of Their Own Roles in the Process." Korean J Hosp Palliat Care, 18(1), 42-50. Han, S. (2015b). "Social Workers' Knowledge of Advance Directives for Health Care and Understanding of their Role on Elderly Patients and Family Caregivers' End-of-Life Care Decision in Long Term Care Facilities." Studies on Life and Culture, 36(2). CARE RIGHTS SURVEY 8 Figure 4. Recently Occurred Tragic Cases CARE RIGHTS SURVEY 9 Question 3: Have the needs of specific groups of older persons been taken into consideration in the process of implementation of MIPAA and if so, how? 3.1. NCDs and Older Patients The proportion of older persons in S. Korea is gradually growing, and it was 12.22% of total Korea population (OECD, 2014).16 Figure 5 shows in regard of location of older persons’ death, the proportion of death in medical institution increased 68.5% to 73.1% between 2011 and 2014.17 Even though those who passed away in medical institution are mostly non treatable, they received life sustaining treatment. However the proposed bill is for dying patients who are near death and the conditions between them and patients with NCDs are different. For that reason, patients with NCDs should be considered particularly. Therefore it is essential to be protected and guaranteed their rights for self determination in order to let them free from unwanted life sustaining treatment. Figure 5. Death Place and Increasing rate Location of death %(2011>2014) Medical Institution (hospital, and convalescent hospital) 68.5>73.1 Private Home 19.8>16.6 Others (Long Term Care Institutional Facility, Paramedic Ambulance Service, Workplace, etc.) 11.6>10.3 3.2. Older immigrants In 2013, the number of immigrants worldwide reached 232 million, up from 154 million in 1990. 18 Globally, there are close to 26 million migrants aged 65 and over. 19 Older migrants represent 11 percent of the total 16 OECD Data, https://data.oecd.org/pop/elderly-population.htm#indicator-chart 17 STATISTICS KOREA. 2014 Statistics of birth & death, http://kostat.go.kr/portal/korea/kor_nw/2/2/3/index.board?bmode=read&aSeq=333915, 2011 Statistics of birth & death, http://kostat.go.kr/portal/korea/kor_nw/2/2/3/index.board?bmode=read&bSeq=&aSeq=253821&pageNo=6&ro wNum=10&navCount=10&currPg=&sTarget=title&sTxt= 18 U.N. Department of Economic and Social Affairs (2013). World Population Polices 2013. New York: U.N. , http://www.un.org/en/development/desa/population/publications/pdf/trends/Concise%20Report%20on%20the% 20World%20Population%20Situation%202014/en.pdf 19 U.N DESA. (2013). World Population Ageing 2013. New York: U.N. http://www.un.org/en/development/desa/population/publications/pdf/popfacts/popfacts_2013-4.pdf CARE RIGHTS SURVEY 10 migrant population, as compared to 8 percent for the world’s population. South Korea has the fastest growing ageing population in Eastern Asia. 20 In 2014, the number of international migration of Korea is 1,328,711. The number of non-Koreans living in Korea now exceeds 1.74 million people. 21 Lack of Health Care Legislation promoting Advance Directives raises the risk of immature EOL decisions that could result in healthcare deficits such as neglect, abuse, and discrimination for elderly patients’ EOLCD, domestic/abroad. Differences in legal systems and health insurance plans among countries in EOL care & decision results in lack coordination in upholding the Emergency Medical Service Act and utilizing the Emergency Service Fund (ESF) to aid domestic and foreign older patients. 3.3.Older Patients with Advanced Dementia During 2008 to 2012, the rate of older dementia patients increased from 8.4% to 9.18%. 22 The number of aged patients with dementia in 2012 had increased by 26.8% compared to 2008. According to research which conducted by Ministry of Health and Welfare, prevalence rate of dementia between age 65~69 was 1.3%, however those older than 85 was 33.9%.23 We can say the rate rapidly increased and the financial burdens of treating dementia are also increased. According to a study, among annual total medical expenses, dementia was about 810 billion won in 2010.24 In regard to dementia, the total medical expenditure of dementia increased 1,232.1% in 2010 than that of 2002.25 20 International Migration by Age and Sex.(National and foreign), http://kosis.kr/eng/statisticsList/statisticsList_01List.jsp?vwcd=MT_ETITLE&parmTabId=M_01_01#SubCont 21 Ministry of Foreign Affairs, Republic of Korea, 2015, http://www.korea.net/NewsFocus/Society/view?articleId=128653 22 Ministry of Health and Welfare, 2012,Nationalwide study on the prevalence of dementia in Korean elders,http://www.mw.go.kr/front_new/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&CONT_SE Q=286138&page=1 23 Ministry of Health and Welfare, 2012,Nationalwide study on the prevalence of dementia in Korean elders, op. cit. 24 National dementia management plan, 2012, download : https://www.google.co.kr/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CCIQFjAAahUKEwian8_37 pTHAhVhL6YKHQr3Ao8&url=http%3A%2F%2Fwww.alzza.or.kr%2Fezboard%2Fezboard.asp%3Fmode%3 Ddown%26id%3Dnotice%26idx%3D11811%26filei%3D1%26filename%3D%25C1%25A62%25C2%25F7%2 5B1%25B9%25B0%25A1%25C4%25A1%25B8%25C5%25B0%25FC%25B8%25AE%25C1%25BE%25C7% 25D5%25B0%25E8%25C8%25B9_2012.7.30.hwp&ei=5onDVZqUKOHemAWK7ov4CA&usg=AFQjCNG5z GNVq6RFPsx3-d-SD9wLGWMYWg&sig2=J7K5HNSZZuUzAni3iHCfmQ&bvm=bv.99556055,d.dGY 25 Korea Institute for Health and Social Affairs, Older persons medical expenditure growth and effective way of management, 2011, https://www.google.co.kr/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CCIQFjAAahUKEwjym8jsq 5XHAhXBoJQKHZ5WCpc&url=https%3A%2F%2Fwww.kihasa.re.kr%2Fhtml%2Fjsp%2Fshare%2Fdownloa d_forum.jsp%3Fbid%3D21%26aid%3D114%26ano%3D1&ei=xsnDVfKgAsHB0gSeram4CQ&usg=AFQjCNG 9wQ2O4UnDOezpU-W_vFhEDo69QA&sig2=T2cywWQ9PnGCnT94WXOUXQ&bvm=bv.99556055,d.dGo CARE RIGHTS SURVEY 11 Question 4: Have older persons been informed about MIPAA and if so, how? How are older persons participating in the implementation of MIPAA including in decision-making about MIPAA implementation? 4.1. Lack of awareness and knowledge about EOL care and decision Even though, 86% of subjects want about discontinuing life sustaining treatment and think the enactment of related laws is essential. However, only 6% of the patients were benefited to have DNR order in advanced. Another studies conducted in South Korea found that Korean older persons and their family caregivers tend to be limited in their knowledge of EOLCD and that Korean elderly prefer to relegate their decisions to the family even if they are able to make them on their own. (Hong, 2010; Hong and Kim, 2013). 26 Even if elderly individuals may wish to move forward with their decision, their families may resist because allowing the elderly relatives to make their own decisions or initiate communication is antithetical to the principle of filial piety, which is a critical aspect of their cultural and family norms (Kim & Han, 2013; Park & Song, 2013). Often, older persons are not allowed to get informed about their illness and decision-making. Usually people regard that informing about their illness and close to death is bad for them, so older persons cannot prepare for their death properly. Furthermore, when there are conflicts in the family of patients, Hospital ethic committee will mediate their difference of opinions. 4.2. Education and Counseling Educating and counseling for older persons can be important implementation tool to inform them about MIPAA, Also civic agencies and experts can be helpful resources for them. Letting international societies know the actual states of Korea is necessary. Care Rights held education & counseling program ‘Well-dying & Older person’s Rights” at Gangnam Senior Plaza in Seoul. Now Care Rights are carrying counseling program at Seocho district office, “Well-dying and education & counseling of Hyo program”. In 2015, we are going to participate for public education in ‘2015 ASEM CONFERENCE ON GLOBAL AGEING AND HUMAN RIGHTS OF OLDER PERSONS’27. 4.3. Advocating and Enactment Public campaign is also essential tools for older persons to participate implementation of MIPAA. Care rights 26 Hong, S. 2010, "An empirical study for model development concerning advance directives." Journal of Korean Gerontology, 30(4). 1197-1211, Hong, S. W. & Kim, S. M. 2013, "Knowledge regarding advance directives among community-dweling elderly." Journal of Korean Academic Society of Nursing Education, 19(3), 330-340. 27 2015 ASEM CONFERENCE ON GLOBAL AGEING AND HUMAN RIGHTS OF OLDER PERSONS, http://www.aseminfoboard.org/events/20151026?field_upcoming=All CARE RIGHTS SURVEY 12 participated in legislative process.28 We are participating in enacting process through public hearing.29 28 29 Care Rights, 2015, http://med.carerights.org/bbs/board.php?bo_table=dbcenter&wr_id=9 http://carerights.org/bbs/board.php?bo_table=dbcenter CARE RIGHTS SURVEY 13 Question 5: What impact has MIPAA implementation had on equality and non-discrimination of older persons? 5.1. History of Hospice & Palliative Care in Korea Hospice was first introduced by 'Little Company of Mary' In 1963. After that, operated hospitals and facilities remained unchanged by some religious communities for about half a century. It hasn't been activated so far. Government created legal basis for people with advanced cancer through the "Act on Management of Cancer" in 2011. But unfortunately, the law didn't include all patients suffering from terminal disease. It is a law restricting patients from receiving palliative care services as patients with terminal cancer. Facilities and perspectives for hospice are in poor condition to such an extend Around 260,000 people die, but hospice & palliative care services used for just two percent of them. 1,300,000 Korean suffers, including patients and family caregivers in this situation (KOSIS, 2013). 30 So "Act on Palliative Care & Hospice (No. 14991)31" was proposed in Apr, 30, 2015. The law protect human's dignity for terminal patients and provide care that patients and family caregivers need by defining the main thing about hospice & palliative care. Here are the ramifications of the new law. Definition of hospice, palliative care and life sustaining treatment (Amendment No.2) National planning about hospice & palliative care is a renewable on a five-year (Amendment No.6) Development of specialists on the staff (Amendment No. 8) Fill in an advance directives form (Amendment No. 20) Financial aid of government for hospice & palliative care (Amendment No. 22) 5.2. Target Area and Population A. Elderly Patients Cultural norms and expectations for the family caregiving play an essential role in the process of end- 30 KOSIS. 2013, “Annual Report on the Causes of Death Statistics”, Available from http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B34E01&vw_cd=MT_OTITLE&list_id=MT_CTI TLE_1&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=K2 31 The National Assembly of the Republic of Korea. 2015, “Act on Palliative care & Hospice”, Available from http://likms.assembly.go.kr/bill/jsp/BillDetail.jsp?bill_id=PRC_F1L5E0A4S3M0R1G8A1L6B5Y9Q4N8E3 CARE RIGHTS SURVEY 14 of-life care decision making: Many Asian countries consider these discussions with their elderly relatives as a taboo and a filial impiety (Kim & Han, 2013)32. Often, elderly patients do not understand the concept of the autonomy. Thus, they prefer to relegate their EOL care decisions to their family caregivers (Kwon, 2010) 33. According to the Korean statistical information service (KOSIS, 2013)34, 73% of the total elderly population end their life not in their private homes but in intensive care units, hospital for acute and skilled nursing care, and longterm care facilities. B. Elderly Immigrants Domestic and foreign elderly patients are too often deprived of their rights to informed consent during EOL care & decision in S. Korea. Their desire to refuse aggressive life-sustaining treatments may not be fully preserved, if they are unable to make EOL decisions at the time of service in S. Korea. However, they are often given unwanted aggressive life-sustaining treatments without protection from culturally-designed, advanced EOL decision making process that makes available and promotes painfree and comfortable hospice care. Lack of Health Care Legislation promoting Advance Directives raises the risk of immature EOL decisions that could result in health care deficits such as neglect, abuse, and discrimination for elderly patients’ EOL care & decision, domestic/abroad, C. Older Person with Advanced Dementia Elderly patients diagnosed with advanced dementia are transferred to acute hospital if they need treatment, regardless of their decision for hospice or any other type of EOLCD in advance. Also it may cause greater confusion to discuss about EOLCD with family caregivers of elderly relatives with advanced dementia because of the stigma of certain diseases, and lack of knowledge about EOLCD. 32 Kim, T. H. & Han, S. Y. 2013, “Family Life of Older Korean”, 『Ageing in Korea 3rd』, Seoul: Med Inc. 33 Kwon, H. N. 2010, “A Study on Case Comparison of Withdrawal of Life-Sustaining Care and Possibility of justification in Death with Dignity – Focused on cases of Cardinal Kim Soo-Hwan and former president Kim Dae-Jung”, J of Bioethics, 11(1), 33-49. 34 KOSIS, 2013, “2013 Annual Report on the Causes of Death Statistics”, Available from http://kosis.kr/ups/ups_01List.jsp?pubcode=YD CARE RIGHTS SURVEY 15 Question 6: What impact has MIPAA implementation had on the fulfillment of the right of older persons to an adequate standard of living? There are two different standards regarding EOLCD that we searched. In figure 6 and figure 7, they show the standard of the unit for hospice palliative care and long-term care facility. We could not find the protocol of EOLCD and advance directives. According to the recent survey of Korean ministry of health and welfare (2015)35, 21.4 percent of the total palliative care units are not up to standard; 12 units of 56 palliative care units. They unmet the requirements of the facility standard, including number of required nurse, training, protocols for EOLCD in the palliative care. Here is the <Standard of Palliative Care Units in Korea> 36 Figure 6. Standard of Palliative Care Units in Korea Standard of Palliative Care Units in Korea 1. A. B. Balanced Allotment of Workers Essential Staff Physician or Doctor of Korean Medicine : At least five percent of an average annual patients in facilities(units) Nurse (of palliative care units) : At least 50 percent of an average annual patients in facilities(units) Social Worker : At least one person (Full-time) Training : The essential staffs must complete education about palliative care. a. - Educational contents : Evaluation method of patient with terminal cancer Pre-hospice care planning Communication for patients and family caregivers Contents about palliative care including pain of patients and management of symptoms b. Minimum educational requirements : The 60 hour basic education and four hour refresher training per year c. 35 Education institutions : Regional Cancer Center Palliative Care Unit National Cancer Center Medical · Korean Medicine · Nurse Association Korea Association of Social Workers Association about Palliative Care Asia Today(Newspaper). 03. 12. 2015, Available from http://www.asiatoday.co.kr/view.php?key=20150312010007660 36 Korean Ministry of Government Legislation. “Enforcement Regulation from Act on Management of Cancer (Amendment No. 13)”, Available from http://www.law.go.kr/lumLsLinkPop.do?lsId=009513&lsThdCmpCls=LR&joNo=002500000 CARE RIGHTS SURVEY 2. Standard of Facilities & Equipment Aside of the other units, the palliative care unit operates for patients with terminal cancer separately A. B. 16 Detailed criteria Room Quantity Facilities & Equipment Suction unit, Oxygen concentrator, Wheelchair Notes Distinction of sex Less than five beds per room Separate sections Patient’s room 3 Room for last day 1 Shower room 1 Family lounge 1 Counseling room 1 Separate sections Nurse station 1 Separate sections Treatment room 1 Restroom 2 Necessary equipment for providing bath services Facilities for rest of patients and family caregivers Located in palliative care unit Separate sections Syringe, Dressing, Disinfectant, Tool of venoclysis, etc. Separate sections Distinction of sex Here is the <Standard of Long-term Care Facilities in Korea> Figure 7. Installment standard of requirement of long-term care institution Installment standard of requirement of long-term care institution (Article 22 Section 1 related) 1. Common matter A. Scale of facility Long-term care institution (hereafter “facility”) should be able to accommodate different number of patients according to the following facility type. (1) Facility: more than ten people (more than 23.6㎡ space per one person) (2) Group home: more than five and less than nine people (more than 20.5㎡ space per person) B. Structure and equipment of facility (1) The facility’s structure and equipment should consider lighting, ventilation, residents’ sanitation and environmental safety, etc. (2) Equipment frequently used by residents such as corridors, lavatory, bedroom, etc. should have space for a wheel chair to pass by, and should be convenient for elderly’s activities. (3) Facility should have emergency exit and fire-fighting material. However, facility with fewer than ten residents may take precautions for disasters according to the facility’s circumstances. … 3. Facility standard Room type Facility type Patient room office Staff room Volunteer room Medic and nurse room Physical therapy room Program room Cafeteria, kitchen Emergency evacuation facility Toilet Shower room Laundry room 17 CARE RIGHTS SURVEY Facility More than 30 residents O More than 10, less than 30 residents O Group home O O O O O O O O O O O O O O O O O O O O O O O O O Remarks: … (2) … however the facility should install slopes and elevators for the residents’ convenience if the common physical therapy room is in a different floor with the patient room. 4. Equipment standard A. Bedroom … (2) Men and women bedroom should be separated. (3) 6.6 ㎡ bedroom space per resident is required. (4) Residential room’s capacity is four people or less. … 5. Required standard of employee Type Required standard Administrator of facility Licensed social work under <Social Service Law> and medical staff under the <Health law> Social worker Licensed social work under <Social Service Law> Rehabilitation therapist Licensed rehabilitation therapist under <Law regarding nursing technician> Nursing assistance First level certification of nursing assistance staff 6. Standard for employee’s allocation Type of occupat ion Administrat or of facility Manage r Social worker Doctor(includi ng oriental medical doctor or staff doctor) Nurse or nursing assistan t Rehabilitati on therapist Nonmedica l staff Office worker Dietitia ns Kitche n staff Housekeepi ng staff Securit y More than 30 residen ts 1 1(only when there are more than 50 resident s) 1 (1 per 100 resident s) More than 1 1 per 25 residen ts 1 (1 per 100 residents) 1 per 2.5 residen ts Requir ed number 1 (only when there is more than 50 kitchen staff) Requir ed number Required number Requir ed number More than 10 and less than 30 residen ts 1 1 1 1 Required number 1 per 2.5 residen ts Requir ed number Required number Type of facility Facili ty Group house 1 1 1 per 3 residen ts Remarks: … (2) Social worker establishes plans for providing elderly welfare such as health maintenance, recreational activity program and basic counseling service for the elderly residents. However, it was not mentioned for their role for engagement in the process of EOLCD. … CARE RIGHTS SURVEY 18 Question 7: Please provide examples of best practices from a human rights perspective in your country in the implementation, monitoring, review and appraisal of MIPAA. 7.1. Care Rights provide, A. Education & Counseling This program is designed to clearly elucidate the end-of-life care decision making process through advanced care counseling services and psychosocial support. It serves to guide primarily those who are actively navigating their end-of-life care including their families and health care staffs, but it is also highly recommended to anyone who wants to be planned in advance. B. Advocacy & Enactment This entails encouraging stakeholders, policy makers, as well as the general public to advocate for sound legislations related to end-of-life care and decision making by collaborating with seminars, forums and campaigns. C. Survey & Research We oversee data collection and analysis to develop evidence-based counseling programs, educational manuals for elderly patients, family caregivers, and health care staffs. This program is sponsored by the SSK project under the umbrella of the Korean National Research Foundation and Namseoul University Academic Foundation. D. UN Activity Partnering with the UN and civil organizations, we help design and refine services pertaining to Sustainable Development Goals(SDGs). Participating in the 2015 UN SDGs forum, the 6th Open Ended Working Group on Ageing( OEWGA) meeting and the survey on UN Geneva Human Rights. 7.2. We also conduct project for the 2015, CARE RIGHTS SURVEY A. 19 Education & Counseling "End-of-Life Care Decision & Older Persons Rights" is an educational program about advance directives, and other ways to safeguard one's autonomy. "Well-Dying &HYO(Filial Piety)". We are infusing Korean cultural norm of filial piety -HYO- into our educational content to help better facilitate end-of-life care & decision making. This program equips them with the tools necessary to discuss and plan their advance care in long term care facilities. B. Advocacy & Enactment Care Rights participated at the public hearing of "Legislation about Hospice & Palliative Care" & "Legislation about End-of-Life Care Decision Making" in S. Korea. The events included introduction to legislation of hospice & palliative care, discussion about details and multidisciplinary announcement was a good opportunity for hospice & palliative care system. And we join in side event on the occasion of the 6th Open Ended Working Group from UN DESA. We announced cultural differences in recognizing and protecting older person’s rights in end of life care and decisions through the presentation. And, also, forum on “Hospice & Palliative Care Model of New Paradigm ” was hold in Seoul. Practitioners and administrators for hospice & palliative care facility and home based service in domestic and abroad was discussed about operating the hospice & palliative care unit for patients and family caregivers. The Join World Conference on Social Work, Education and Social Development, under the theme “Promoting the dignity and worth of people”, will be held from 2016 at COEX in Seoul, Korea. The first day of the event, International Health Care Decision Day held by Care Rights, The program will include symposium, exhibition and activities for fill out the advance directives with UN experts, research, NGOs & CSOs that work for older person’s rights, SSK research team of Seoul National University. CARE RIGHTS SURVEY 20 Question 8: Please provide information about the main challenges (such as institutional, structural and circumstantial obstacles) your country faces at the various levels of government (communal, provincial and national etc.) to fully respect, protect and fulfill the human rights of older persons in the implementation of MIPAA. 8.1. Government and Policy Makers “Act on Palliative Care & Hospice (No. 14991)” was proposed for more than 50 years. The government and policy makere therefore, should proceed and support the activation and development of hospice & palliative care by establishing a law about it. 8.2. Health care providers Patients with terminal illness stay mainly Intensive Care Unit at hospitals, therefore professional medical staffs including physicians, nurses, social worker should have a broad knowledge of hospice & palliative care including evaluation method of patient with terminal condition, creative advanced care planning, communication for patients and family caregivers. And they should follow the protocol by the government so the service is sustainable. 8.3. NGOs & CSOs Taboo to do advance care planning is still prevalent in Korean society. However, this consciousness is illogical and must be combated with public education and awareness. That is a key part of NGOs & CSOs’ role. And NGOs & CSOs should demand legislation from the government for the patients suffering from terminal disease, provide public education, create community service that facilities cannot do such as home hospice, volunteer service. CARE RIGHTS SURVEY 21 References 150224 Press Release: recommendation for protecting human rights for users of Elderly Medical Welfare Facility 2011 Statistics of birth & death, http://kostat.go.kr/portal/korea/kor_nw/2/2/3/index.board?bmode=read&bSeq=&aSeq=253821&pageNo=6&rowNu m=10&navCount=10&currPg=&sTarget=title&sTxt= 2015 ASEM CONFERENCE ON GLOBAL AGEING AND HUMAN RIGHTS OF OLDER PERSONS, http://www.aseminfoboard.org/events/20151026?field_upcoming=All Asia Today(Newspaper). 03. 12. 2015, Available from http://www.asiatoday.co.kr/view.php?key=20150312010007660 Family Experiences of End of Life Care Decisions for Elderly Patients in South Korea, Soo Han, Tae Hyun Kim Hong, S. 2010, "An empirical study for model development concerning advance directives." Journal of Korean Gerontology, 30(4). 1197-1211, Hong, S. W. & Kim, S. M. 2013, "Knowledge regarding advance directives among community-dweling elderly." Journal of Korean Academic Society of Nursing Education, 19(3), 330-340. Care Rights, 2015, http://med.carerights.org/bbs/board.php?bo_table=dbcenter&wr_id=9http://carerights.org/bbs/board.php?bo_table=d bcenter https://www.google.co.kr/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CCIQFjAAahUKEwjym8jsq5XH AhXBoJQKHZ5WCpc&url=https%3A%2F%2Fwww.kihasa.re.kr%2Fhtml%2Fjsp%2Fshare%2Fdownload_forum.j sp%3Fbid%3D21%26aid%3D114%26ano%3D1&ei=xsnDVfKgAsHB0gSeram4CQ&usg=AFQjCNG9wQ2O4UnD OezpU-W_vFhEDo69QA&sig2=T2cywWQ9PnGCnT94WXOUXQ&bvm=bv.99556055,d.dGo International Migration by Age and Sex.(National and foreign), http://kosis.kr/eng/statisticsList/statisticsList_01List.jsp?vwcd=MT_ETITLE&parmTabId=M_01_01#SubCont KAKDANG SOCIAL WELFARE FOUNDATION, http://www.kakdang.or.kr/ Kim, T. H. & Han, S. Y. 2013, “Family Life of Older Korean”, 『Ageing in Korea 3rd』, Seoul: Med Inc. Korea Institute for Health and Social Affairs, Older persons medical expenditure growth and effective way of management, 2011, Korean Initiative for Advance Directive, http://www.sasilmo.net/ Korean Ministry of Government Legislation. “Enforcement Regulation from Act on Management of Cancer (Amendment No. 13)”, Available from http://www.law.go.kr/lumLsLinkPop.do?lsId=009513&lsThdCmpCls=LR KOSIS, 2013, “2013 Annual Report on the Causes of Death Statistics”, Available from http://kosis.kr/ups/ups_01List.jsp?pubcode=YD KOSIS. 2013, “Annual Report on the Causes of Death Statistics”, Available from http://kosis.kr/statHtml/statHtml.do?orgId=101&tblId=DT_1B34E01&vw_cd=MT_OTITLE&list_id=MT_CTITLE _1&seqNo=&lang_mode=ko&language=kor&obj_var_id=&itm_id=&conn_path=K2 Kwon, H. N. 2010, “A Study on Case Comparison of Withdrawal of Life-Sustaining Care and Possibility of justification in Death with Dignity – Focused on cases of Cardinal Kim Soo-Hwan and former president Kim DaeJung”, J of Bioethics, 11(1), 33-49. Ministry of Foreign Affairs, Republic of Korea, 2015, http://www.korea.net/NewsFocus/Society/view?articleId=128653 Ministry of Health and Welfare, 2012,Nationalwide study on the prevalence of dementia in Korean elders,http://www.mw.go.kr/front_new/al/sal0301vw.jsp?PAR_MENU_ID=04&MENU_ID=0403&CONT_SEQ=28 6138&page=1 Ministry of Health and Welfare, 2012,Nationalwide study on the prevalence of dementia in Korean elders, op. cit. CARE RIGHTS SURVEY 22 National dementia management plan, 2012, download : https://www.google.co.kr/url?sa=t&rct=j&q=&esrc=s&source=web&cd=1&ved=0CCIQFjAAahUKEwian8_37pTH AhVhL6YKHQr3Ao8&url=http%3A%2F%2Fwww.alzza.or.kr%2Fezboard%2Fezboard.asp%3Fmode%3Ddown%2 6id%3Dnotice%26idx%3D11811%26filei%3D1%26filename%3D%25C1%25A62%25C2%25F7%25B1%25B9%2 5B0%25A1%25C4%25A1%25B8%25C5%25B0%25FC%25B8%25AE%25C1%25BE%25C7%25D5%25B0%25E 8%25C8%25B9_2012.7.30.hwp&ei=5onDVZqUKOHemAWK7ov4CA&usg=AFQjCNG5zGNVq6RFPsx3-dSD9wLGWMYWg&sig2=J7K5HNSZZuUzAni3iHCfmQ&bvm=bv.99556055,d.dGY National Health Insurance Service, http://www.nhis.or.kr/static/html/wbd/g/a/wbdga0301.html National Human Rights Commission of Korea, 2009, https://library.humanrights.go.kr/hermes/web.search.Search.ex?command=SearchDetailGet, http://library.humanrights.go.kr/hermes/imgview/10-04.pdf OECD Data, https://data.oecd.org/pop/elderly-population.htm#indicator-chart OECD, OECD Economic Surveys: Korea 2014, http://www.oecd-ilibrary.org/economics/oecd-economic-surveyskorea-2014_eco_surveys-kor-2014-en STATISTICS KOREA. 2014 Statistics of birth & death, http://kostat.go.kr/portal/korea/kor_nw/2/2/3/index.board?bmode=read&aSeq=333915, The Ministry of Health and Welfare, The survey for older person's life and condition 2014, op. cit. The Ministry of Health and Welfare, 2014 research on actual condition of aged, http://www.prism.go.kr/homepage/researchCommon/retrieveResearchDetailPopup.do?research_id=1351000201500109 The Ministry of Health and Welfare, The survey for older person's life and condition 2014, http://www.prism.go.kr/homepage/researchCommon/retrieveResearchDetailPopup.do?research_id=1351000201500109This research is conducted in every 3 years The National Assembly of the Republic of Korea, a draft related to hospice & palliative care, bill number 1914991,http://likms.assembly.go.kr/bill/jsp/BillDetail.jsp?bill_id=PRC_F1L5E0A4S3M0R1G8A1L6B5Y9Q4N8E 3 The National Assembly of the Republic of Korea, Draft regarding the use of hospice & palliative care and end-oflife-stage patient’s decision making on life sustaining treatment, 2015,http://likms.assembly.go.kr/bill/jsp/BillDetail.jsp?bill_id=PRC_M1K5N0R7R0U7S1B5X0F4S5C8Y9Z8K5 The National Assembly of the Republic of Korea. 2015, “Act on Palliative care & Hospice”, Available from http://likms.assembly.go.kr/bill/jsp/BillDetail.jsp?bill_id=PRC_F1L5E0A4S3M0R1G8A1L6B5Y9Q4N8E3 U.N DESA. (2013). World Population Ageing 2013. New York: U.N. http://www.un.org/en/development/desa/population/publications/pdf/popfacts/popfacts_2013-4.pdf U.N. Department of Economic and Social Affairs (2013). World Population Polices 2013. New York: U.N. , http://www.un.org/en/development/desa/population/publications/pdf/trends/Concise%20Report%20on%20the%20W orld%20Population%20Situation%202014/en.pdf WHO, Noncommunicable diseases country profiles 2014, http://www.who.int/nmh/publications/ncd-profiles2014/en/