I authorize the release and exchange of medical and educational... child’s physician and school staff that is necessary in carrying...
advertisement

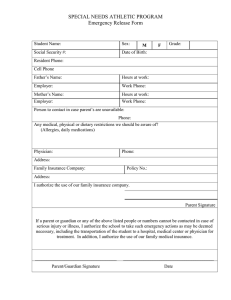
Yes ___ No___ The student has been instructed in self-administration of the Epi-Pen. Yes ___ NO___ I authorize my child to carry and administer own medication as prescribed by Physician. I authorize the release and exchange of medical and educational information between my child’s physician and school staff that is necessary in carrying out this service to my child. Parent Signature __________________________ Date___________________ Phone numbers ___________________ Emergency contact_________________________ Phone numbers___________________ Physician PRINT ___________________________ Phone numbers __________________ Physician Signature_______________________________ Revised Mar 2014 Date__________________