1.0 DISEASE SURVEILLANCE
advertisement

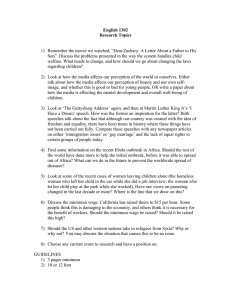
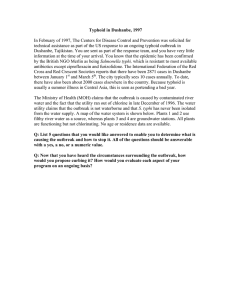
WHO SOUTHERN SUDAN HEALTH UPDATE September 2000 HIGHLIGHTS Surveillance project review takes place in Cairo Modified IMCI and Epidemiology training continues Small scale Tuberculosis control strategy adopted for s Sudan World Aids Day 2000 planned in Yambio for community sensitization Epidemic response to malaria in Bor, measles in Wudier and meningitis in Akobo. Polio AFP surveillance gets a big boost by deployment of 155 Field assistants. 1.0 DISEASE SURVEILLANCE 1.1 Project review team satisfied with s Sudan Surveillance A major project review of the S Sudan Surveillance program took place in Cairo. The review by WHO HQ, EMRO and Sudan WHO staff was satisfied with the progress achieved by the project. The second phase of the project will consolidate the achievements and expand to the government held areas of the south. 1.2 Capacity Building using modified IMCI Further training of health workers on a modified Integrated Management of Childhood Illnesses (IMCI) course, with an emphasis on outbreak prone childhood illnesses, continued in Upper Nile. This is a follow-up of the August WHO/UNICEF/CCM/COSV and WHO/HQ collaborative IMCI TOT at Adior, Bahr Ghazal. The training was conducted at Nyal in two phases: a four-day training for COSV health service supervisors/facilitators and a oneweek training of health workers. A total of 5 supervisors who will also work as IMCI training facilitators and 13 health workers (12 from COSV-run health facilities and a WHO field assistant) were enrolled. To foster understanding and enhance skills, course work, video shows, practical sessions and presentations were used. Lessons from this training will also be incorporated in earlier observations to further improve the quality of IMCI training. WHO appreciates all those who have collaborated in this effort and looks to further enhancing disease surveillance and response. 1.3 Basic Epidemiology training continues As part of the training activity of the three WHO public Health Co-ordinators, one of the WHO staff continued to provide technical backstop to NGOs, another participated at an Emergency needs assessment mission, while the third co-ordinator continued with field supervision of health facilities. As per the schedule, WHO in-house training with an emphasis on “ Infectious Diseases (IDs) Epidemiology” continued in September 2000. 1.4 Laboratory support for surveillance In view of the current malaria outbreaks in Bor, WHO identified two NGOs; ACROSS and NCA for support with binocular microscopes as well as training to improve case management. Once assessments are finalised and organisations provide official requests, binocular microscopes will be handed over to local communities to be used at the NGO health service facilities. WHO encourages health organisations interested in providing laboratory services and enhance outbreak investigation and response to contact the WHO Loki office. 1.5 EWARN Strengthening by community involvement WHO held the second round of advocacy meetings with local partners and community members in Twic county, Turaliel and Aweng, in northern Bahr El Ghazal. Similar advocacy meeting were held at Lankein and Udier in Upper Nile. The discussion identified that malaria outbreak is frequent and health services’ capacity to respond to these outbreaks is limited. It was also identified that there is a need for a community-level sensitization 1 about common outbreaks in the area. WHO will continue its dialogue with the health and education NGOs and local counterparts on the ground. Similar advocacy discussions were held with health workers and WHO field polio assistants. Based on the identified needs, WHO will conduct community awareness and EWARN strengthening activities in these areas. 1.6 Utilising the AFP surveillance network In September, training of AFP/Polio field supervisors and assistants continued at Lankien and Nyal, in Upper Nile; Boma and Mapel, in Bahr El Ghazal; and Tambura and Maridi, in Equatoria. At these sessions, orientation on enhancing EWARN through community alerting and response was given for a total of 84 field staff and local partners. As a result of this integration of AFP Surveillance to EWARN, WHO is already receiving outbreak alerts from the polio field staff. 1.7 Outbreak Verification and Response 1.7.1 Malaria at Paluer, Bor, Upper Nile WHO received a report of a malaria outbreak from UNICEF and ACROSS on 01/09/00. Bor, like most of Upper Nile, is known as a highly malaria endemic area with repeated outbreaks. Following the report, WHO with ACROSS did a preliminary investigation to assess the magnitude and identify urgent response needs. It was identified that eight health facilities in the county have reported increasing cases starting mid June 2000 which more than doubled by August. Those severely affected were children, with more than 95% of all admissions and deaths occurring among this group. WHO through UNICEF support provided emergency drugs and supplies. Radio monitoring, field-visits, and service data and situation reports were used to track the outbreak. As of September 2000, the number of cases remains high but trends in mortality rate among those admitted to health facilities show a marked decrease (from 1.4% in August 2000 to 0.85% in September). Increase in cases is attributed to an improving health seeking behaviour (scaled up health messages and services), continued transmission (season), and improved reporting from PHCUs. The marked decrease in death rate is attributed to improved case management and an early health-seeking behaviour. A follow-up visit indicated that the outbreak is fully contained. 1.7.2 Measles at Wudier, Latjur, Upper Nile On 05/09/00, WHO received an outbreak call from its Polio/AFP field staff. The cases reported fitted a case definition of measles. First cases were detected by the PHCU on the 4th week of July (22/08/00). A preliminary investigation was done on the date of report. It was established that this was a measles outbreak with high risk of further spread to vulnerable host community children in other villages and among internally displaced population villages. Immediate needs were identified and WHO provided technical support on immediate interventions, including health education, management of complicated cases and vit A supplementation. Through UNICEF support, on 10/09/00, WHO deployed a Public Health Coordinator with drugs, vaccines, vit A and supplies. The WHO Public Health Co-odrinator deployed two local teams of six PHCU health workers. The teams, lead by WHO Medical Doctor investigated and managed measles cases, sensitised communities through health education and carried out immunisation in adjacent and distant villages. To enhance outbreak investigation skills of PHCU health workers, along with promoting effective management of cases, the MD investigated 20 suspected cases; of which 19 were proved measles. A total of 856 cases were registered. A total of 30 deaths were reported (case fatality rate of 3.5%), out of whom 15, i.e. half of all deaths, are registered. High level of malnutrition believed to have contributed to severe complications. More lives, however, were saved as a result of prompt intervention, including intensive health education, improved health seeking, and early and effective management of common and treatable complications. Most of the villages were crowded. In one location alone, it was reported that there were 5,276 IDPs and 4,684 returnees. Based on local population estimates, a total of 5,459 children (6 months to 12 years) from 11 villages, including the three outbreak villages, were targeted for vaccination and vit A supplementation. A total of 4,464(84.6% of the target) were vaccinated; and given vit A supplementation. This outbreak investigation and response is unique and an encouraging experience. This is particularly so considering the fact that there is no health NGO working in the area. These achievements were by volunteer health workers of a PHCU supported by the local counterpart. An important experience from this epidemic was the daily follow-up and technical backstop through radio, which was very useful in prompt and effective response. WHO’s proactive involvement of local staff in investigation, response, and monitoring was invaluable to build sustainable local capacity and ensure prompt response. 1.7.3 Rumours of Meningitis at Bunagok; Yerol; Bahr El Ghazal…cerebral malaria WHO received rumours of suspected meningitis cases at Yirol in Bahr Ghazal from ICRC on 09/09/00. Based on this report, WHO did a follow-up investigation and verified that there were three cases of reported cerebral malaria with one reported death at a place called Bangok. After a follow-up for two weeks after the first reported cases, no other cases were reported. Conclusion: No meningitis outbreak. 1.7.4 Meningitis at Akobo; Beih; Upper Nile On 18/09/00, MSF-Beligium reported to WHO that there 2 Figure 1.6.6 Meningitis at Akobo, Beih, Upper Nile; September 2000 8 7 6 5 Number were three cases of meningitis on week 36, which increased to six cases on week 36. The disease is reported to manifest with headache, high fever, and neck stiffness. The number of cases increased to seven on week 38 and declined to one case on week 39. A total of 18 cases were reported (See Figure 1.6.6). Most of these cases were children, and there was one death. MSF-B had enough stocks of drugs and supplies and managed all the reported cases at its PHCC at Akobo. At present, there are no more cases reported in the area. Number of Cases Number of Deaths 4 3 2 1.7.5 Febrile illness- Influenza- in, Maridi;Western Equatoria WHO received a report of a febrile outbreak from Maridi County Health Department on 22/09/00 in the village of Makke. Onset was beginning of week 11-17/09/00. Presenting symptoms were mild fever, cough, neck pain, and malaise. The number of reported cases is not established. However, it was reported that there are no deaths. A County Health Department investigation team, with technical support from WHO, visited the area and confirmed that this was a self-limiting flue-like outbreak. The working diagnosis was influenza. Health education on bed rest and fluid and diet was provided. There are no reported deaths. WHO maintains very vigorous surveillance of unexplained fevers in Western Equatoria because of the high risk of haemorrhagic fevers from Central African States. 1.7.6 Measles at Kurmouth, Latjor; Upper Nile An outbreak with fever, skin rash, headache, with reported childhood deaths, was reported to WHO on 18/09/00 from RASS. The outbreak is reported to start in the second week of August at Dualdap village. The descriptions suggest that it is a measles outbreak. Consultations with RASS revealed that the area was not cleared for flight. Further discussions with OLS show that the area is not cleared for flight. Difficult communication and absence of health NGO are obstacles to prompt response. WHO has received a special security clearance to respond to this outbreak. 1.7.7 Measles at Mading, Latjor; Upper Nile WHO received a report, on 22/09/00, of an outbreak of fever, skin rash, and running nose and eye problem among children. This report was from WHO/Polio Surveillance staff. Following the report, radio contacts were made and technical support was provided on prevention of further spread, management of cases, and vit A supplementation. On 26/09/00, WHO through UNICEF support mobilised drugs, supplies and vit A. A total of 258 cases and 10 deaths were reported (case fatality of 3.8%). WHO organised and co-ordinated three vaccination teams of 12 people to respond to the outbreak. The teams were orientated on EWARN, outbreak alerting, clinical diagnosis (case definitions), management of measles complications, safe immunization, and reporting. Following the orientation, the teams were deployed, vaccinated and provided vit A capsules to 3,136 (90.6% of targeted) children in 10 villages, including three outbreak villages and three IDP settlement villages. Major challenges of health care in Mading are lack of essential 1 0 Week 36 Source: MSF-B Week 38 Week 37 Week 39 Report Weeks drugs and supplies and absence of immunization programs as there is no NGO in the area. 1.7.8 Rumours of Meningitis at Mading, Latjor; Upper Nile On 22/09/00 WHO received a report of two childhood deaths from a disease with fever and neck stiffness at Mading. It was rumoured that these cases are meningitis. A retrospective investigation and a one-week follow-up after these deaths occurred documented that no other cases were reported in the area. Moreover, WHO field investigation verified that the two deaths were from tetanus following injuries. 1.8 Supervisory Support In August, WHO provided supervisory support to health facilities in Twic county in northern Bahar El Ghazal, in Bor in Upper Nile, Maridi in Equatoria. A total of six health facilities were visited and discussions were held with health workers. Identified common and critical constraints to improve access and quality of basic health care included inadequate drugs and supplies, little supervisory support, and poor infrastructure and communication. Moreover, lack of in-service training, reference materials, and shortage of personnel were shared challenges. The team informed the health workers on outbreaks and the need for reporting data. 1.9 Internal program reviews From 11-13/09/00, WHO held an in-house process monitoring exercise at Lokichoggio. A meeting with WHO-Khartoum, which discussed on the north-south Sudan activities, followed this review. Based on the Lokichoggio exercise and feedback from HQ, WHO developed a WHO information profile, reviewed a draft and produced a Quarterly Epidemiological Bulletin. WHO also finalised its quarterly activities performance and activities plan reports, and drafted an Outbreak specimen collection and referral format. In addition, WHO did an IMCI follow-up session with HQ, UNICEF, and CCM in Nairobi. The reviews provided invaluable lessons for improving our activities. 3 1.10 Program/Activity Development 2.0 POLIO ERADICATION 1.10.1 STI/HIV/AIDS activities HIV/AIDS is a problem least addressed in southern Sudan. Despite the fact that there are few data on prevalence of HIV infection, low level of awareness and increasing concern among some informed members of communities, there is no organized and well- defined HIV/AIDS intervention so far. Worried by this program gap and aware of the indispensable role of such interventions to curb the epidemic, WHO developed a proposal aimed at program advocacy, improving AIDS awareness, and reducing risky behavior. The proposal has two phases: for the “World AIDS Day", and based on this advocacy and consensus building, a one-year community-based and focused AIDS intervention. This project is shared with UNICEF, and has become a joint initiative. Moreover, UNICEF is ready to play an active role in this invaluable effort. Partial funding is expected from EMRO and UNICEF. 2.1 Training county supervisors and Field Assistants Training for County Supervisors and Field Assistants has been completed in all counties (states) and payams (districts) accessible to OLS. The Field Assistants are distributed as shown below. These Field Assistants are responsible for the implementation of all polio eradication activities at the district level, including campaigns, AFP surveillance and social mobilisation. 1.10.2 TB Control and Leprosy support TB remains a major public health problem that is receiving no attention in s Sudan. WHO s Sudan in collaboration with Headquarters is developing small-scale TB treatment projects using Directly Observed Treatment Short Course (DOTS). A project with possible funding from Norwegian government is under development. Support with drugs is also being provided to Leprosy patients by WHO HQ. 2.3 AFP Surveillance Although 27 cases of Acute Flaccid Paralysis (AFP) from 2000 have been identified by end September, still no wild virus has been isolated (5 cases still pending laboratory analysis). However, we are still faced with the problem of identifying and investigating AFP cases within 14 days from the onset of paralysis. Only 6 out of the 27 cases (22%) can be considered adequate. On a positive note, we are beginning to see the results of placing field assistants in each payam/district with the identification of cases from payams that were previously silent. 1.11 Emergency drugs and supplies WHO developed a proposal for improving stocks of emergency drugs and supplies for southern Sudan. This proposal was developed based on lessons learnt so far in outbreak response, assessment of the health status and facilities, and identified urgent needs for basic services. Moreover, major contributing factors for deterioration of basic health care and subsequently outbreaks were considered. The draft proposal is shared with WHO/HQ, EMRO, WHO/Sudan and an NGO with an interest to support health needs in African countries for possible support. Active AFP Surveillance Reporting sites southern Sudan 2000 2.2 SubNIDS The campaigns were implemented as planned from 16-22 September in Tambura, Yambio, Juba, Yei, Kajo Keji, Torit and Kapoeta counties. Only preliminary results are available at this point from Yambio County where the number of children immunized in the targeted payams exceeded all previous campaigns in the county. Detailed results of the first round in these counties will be available in the October update. IMPORTANT EVENTS 23rd - 27th sNIDs 1st round B/Ghazal 20th-24th 2nd round sNIDs 6-10th Nov 1st round Upper Nile 4-8th December- 2nd round sNIDs 2- 4th December Polio partners evaluation s Sudan 14 - 15TH December - North South NID gap areas Coordination meeting- Fairview Nairobi. UPPER NILE BAHR EL GHAZAL WORLD AIDS DAY 2000 LAKES JONGLEI 1ST DECEMBER 2000 W. EQUATORIA E. EQUATORIA YAMBIO KEY Location of each field assistant who is responsible for active surveillance in his/her district. All districts under OLS have trained field assistants in place. 4