by Hezekiah George Owojuyigbe Bachelor of Medicine, Bachelor of Surgery (MBBS)
advertisement
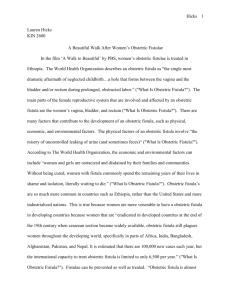
OBSTETRIC FISTULA IN AFRICA by Hezekiah George Owojuyigbe Bachelor of Medicine, Bachelor of Surgery (MBBS) University of Jos, Nigeria, 1998. Submitted to the Graduate Faculty of Multidisciplinary Master of Public Health Program Graduate School of Public Health in partial fulfillment of the requirements for the degree of Master of Public Health University of Pittsburgh 2013 UNIVERSITY OF PITTSBURGH GRADUATE SCHOOL OF PUBLIC HEALTH This essay is submitted by Hezekiah George Owojuyigbe on April 12, 2013 and approved by Essay Advisor: Ronald E. LaPorte, PhD. Director, Multidisciplinary MPH Program Professor, Department of Epidemiology Graduate School of Public Health University of Pittsburgh _______________________________ Essay Reader: Steven M. Albert, PhD. ________________________________ Professor and Chair Department of Behavioral and Community Health Sciences Graduate School of Public Health University of Pittsburgh ii Copyright © by Hezekiah George Owojuyigbe 2013 iii Ronald E. LaPorte, PhD OBSTETRIC FISTULA IN AFRICA Hezekiah George Owojuyigbe, MPH University of Pittsburgh, 2013 ABSTRACT Obstetric fistula as a debilitating complication of labor obstruction is a major public health concern that requires urgent public health interventions. This review looked into a number of major factors that affect obstetric fistula (OF) prevalence, prevention and management in the underdeveloped and developing countries. These contributing factors namely cultural practices of teenage and/or forced marriages leading to earlier pregnancies, extreme poverty, poorly equipped health care services, and lack of education and knowledge about the causes of obstetric fistula. Obstetric fistula is obviously a problem afflicting thousands of women in the underdeveloped and developing nations of the world, women education and empowerment, improved health care services, and poverty alleviation in regions in question would bring some improvement to this “public health problem called obstetric fistula” iv TABLE OF CONTENTS PREFACE ................................................................................................................................. VIII OBJECTIVE…………………………………..………………………………..………………IX KEYWORDS………………………………………….………………………..………………..X 1.0 INTRODUCTION…………………………………………………………………………..1 2.0 METHODOLOGY……………………………………………………………….………….5 3.0 BACKGROUND……………………………………………………………………………..7 4.0 DISCUSSION………………………………………………………………………….........14 5.0 CONCLUSION……………………………………………………………………………..17 BIBLIOGRAPHY………………………………………………………………………………20 v LIST OF TABLES Table 1. Case series of fistula in low income countries…………………………………..……8 Table 2. Contributing factors to vesico-vaginal fistula……………………………………….13 vi LIST OF FIGURES Figure 1. Maryama's story………………………………………………………………………...1 Figure 2. Obstetric vesico-vaginal fistula probe…………………………………………………..2 Figure 3. Methodology………………………………………………………………………….....6 Figure 4. Worldwide fistula center………………………………………………………………19 vii PREFACE Having worked as a physician in sub-Sahara Africa for a number of years, I had the opportunity to see, manage and refer several fistula patients to a more advance care center for further reconstruction care. It is very sad to witness first-hand what these young innocent women have been subjected to; they are been neglected, abused physically and emotionally by their spouses, other family members and their community. They are punished, rejected and ostracized for something they did not do to themselves. There is systemic failure; they are forced into early marriages, there is no standard medical care, they are being subjected to crude traditional procedures, poverty level is at its peak and literacy level is at zero. I have great interest in dissecting and finding a long lasting solution to reducing the incidence of fistula in African women. I believe this is achievable by incorporating better education for women and instituting a better health care system within their reach. I spent hours researching and reviewing a number of related-articles from the library and I also spoke to a number medical professionals in and around the world especially in Africa. I want to seize this opportunity to thank my parents and my siblings for their love, support and prayers. I want to also thank my Professors, Professor Steven Albert and Professor Ronald LaPorte for the time spent in reviewing my essay and for their constructive criticism. Lastly, my appreciation goes to my friends and colleagues for their encouragement. viii OBJECTIVE To analyze and identify pertinent factors influencing the rate of fistula occurrence and how to prevent and manage this obstetric complication in Africa nations from a number of case series and case-control articles reviewed. ix KEYWORDS Obstetric fistula; Vesicovaginal fistula; Rectovaginal fistula; obstructed labor; Maternal Mortality; Gishiri cutting. x 1.0 INTRODUCTION Obstetric fistula is an abnormal connection between two epithelial surfaces. There are different types of obstetric fistula namely; VVF, known as vesico-vaginal fistula, this is a connection Figure 1: Maryama’s Story Maryama comes from a village 100 miles north of Danja, Niger. She was married and became pregnant while still in her teens. As is the local custom – and because maternal health services are not easily accessible – Maryama planned to deliver her baby at home. Since this was her first delivery . Courtesy of Worldwide Fistula Fund between the bladder and the vagina; also there is recto-vaginal fistula which is a connection between the rectum and the vagina. Obstetric fistula is a debilitating obstetric condition resulting 1 from prolonged obstructed labor mostly affects women in the underdeveloped and developing nations of the world especially in Africa and Asia. [1][2]. Figure 2: Obstetric vesico-vaginal fistula from prolonged obstructed labor Probe showing the connection between the bladder and the vagina © PLoS Negl Trop Dis. 2012 August; 6(8):e17 Obstetric fistula (OF) is a major public health problem, there is no doubt especially in Africa where 99% of maternal deaths occur, maternal mortality ratio in developing countries is 240 per 100 000 live births versus 16 per 100 000 in developed counties. Those that did not die will go into labor obstruction which is either unattended to or poorly managed, thus leading to one of its ultimate complications, “fistula.” 2 Obstetric fistula prevention and/or management remain a major challenge in countries where the complication is rampant [3]. There is increased international attention on obstetric fistula as a global public health problem requiring quick solution. Obstetric fistula is a very good example of a neglected tropical disorder, once rampant in western countries, today; obstetric fistula is confined to the cultures of tropical poverty. Labor could be obstructed or prolonged due to three Ps; large passenger (baby), too narrow a passage (birth canal) or low power (mother’s ability to push) which will eventually lead to devitalization of the entrapped soft tissues of the blabber, vagina, rectum and pelvis between the two opposing boney surfaces, the entrapped tissue dies and sloughs away, creating a fistula between the urinary tract and the vagina or between the rectum and the vagina or a combination of both. [4] “Make every mother and child count” World Health Report 2005 says that almost 11 million children under five years of age will die from preventable causes, 4 million of which will not survive the first month of life and half a million women will die in pregnancy, childbirth or soon after. The Millennium Development goals are to reduce this toll by providing access to health care for every mother and every child from pregnancy through childbirth, from neonatal period through childhood. [5] The World health organization states each year between 50,000 to 100,000 are affected by obstetric fistula. The development of obstetric fistula is directly linked to one of the major causes of maternal mortality, which is obstructed labor. In addition, it is also estimated that more than two million young women live with untreated obstetric fistula in Africa and Asia, and these women suffer physical, psychological and social issues; namely nerve damage, leg paralysis, depression, community ostracism, divorce, loss of earning potential and suicide [6] 3 There is strong evidence that major contributing factors to obstetric fistula development in Africa are closely related to socio-cultural and religious beliefs and practices. There is insufficient emphasis placed on community education on causes of obstetric fistula and prevention, and lack of standard health care system in place to urgently address any ensuing obstetric emergencies. Obstetric fistula is preventable; it can largely be avoided by discouraging earlier teenage pregnancies, putting a stop to harmful “gishiri” traditional practices, and most importantly there should be accessibility and affordability of obstetric care. [6] After a prolonged pressure of the infant skull against the tissue of the birth canal, this leads to ischemia and tissue death. The woman is left with a hole between her vagina and bladder or vagina and rectum or both. This results in uncontrollable leakage of urine and/or feces, the view of all these is awful. It is widely reported in scientific publications and the media that women with obstetric fistula suffer devastating social consequences but these claims are rarely supported with evidence. Therefore social implications of obstetric fistula are unknown. [7] 4 2.0 METHODOLOGY This is a cross-sectional study focusing on African women of child-bearing age to determine factors that affect prevalence, prevention and management of obstetric fistula. To achieve this, PubMed, Ovid, Embase, World Health Organization and Global Health databases were searched to identify articles on obstetric fistula in Africa. Searches were conducted with key words: “obstetric Fistula in Africa, vesico-vaginal fistula, or recto-vaginal fistula,” and “obstetric complications.” Articles that were based on case-series, case-control and regional focused on African countries were selected for the review. Six hundred and sixty-one articles on obstetric complication and fistula from around the world were located, a full article and review filter were activated to narrow down the search to 79 articles that were related to Africa and low-income countries, and this was then narrow down to 50 full articles and 21 of the full and cited articles were looked at and reviewed in this essay. 5 661Obstetric complications articles around the world. 344 articles on obstetric complications other than obstetric fistula. 238 non-African nation related article on obstetric fistula. 79 Obstetric fistula articles related to Africa, developing nations. 18 non-full articles, only abstract. 11 articles purely surgical treatment/repair of fistula. 50 Full article on Obstetric fistula in Africa. 21 articles not cited. 8 inaccessible articles. 1 case-control on Obstetric fistula in Africa. 21 Case-series and case-control articles, full and cited articles on obstetric fistula in Africa Figure 3. Methodology 6 3.0 BACKGROUND Several literature searches and reviews were conducted in PubMed, Ovid, Embase and Global Health regarding obstetric fistula amongst women in African, in one of the reviews, among the 19 selected studies, 15 were reported from sub-Saharan African and 4 from the Middle East, it was shown that 79.4% to 100% of fistula cases were obstetrical while the remaining cases were from other causes. Rectovaginal fistula (RVF) accounts for 1% to 8%, Vesicovaginal fistula (VVF) for 79% to 100% of cases, and combined vesicovaginal and rectovaginal fistula were reported in 1% to 23% of cases. Teenagers accounted for 8.9% to 86% of the obstetric fistula patients at the time of treatment, 31% to 67% of these women were primiparas, with 40% - 79% of them being shorter than 1.5m. Among women with obstetric fistula, 57.6% to 94.8% of them labored at home and were transferred late to health care facilities. Nine of 84% of these women delivered at home with mean duration of labor among the fistula patients ranging from 2.5 to 4 days, of which 20% to 95.7% of them laboring for more than 24 hours and operative deliveries were eventually performed in 11% to 60% of cases [8] Obstructed labor is very common in underdeveloped and developing nations of Africa and part of Asia, and vesicovaginal fistula is usually a common complication of this obstetric condition. The formation of fistula remains largely an overlooked problem in developing nations, affecting very young, naïve, illiterate women who live in extreme poverty in remote areas of Africa. It has been shown by several studies and articles that the formation of obstetric fistula is as a result of complex interactions of social, biologic, and economic influences. The key underlying 7 determinants of fistula are the combination of a lack of functional emergency obstetric care, poverty, lack of education, and cultural practices. [9] Table 1. Case series describing characteristics of obstetric fistula patients in low-income countries Series size Time period Age (at repair) Age/parity at fistula Labor/delivery experience Sociodemographic characteristics Kelly [10]; Kelly and Kwast [11] 309 (drawn from 3000) 1983– 1988 Ave 22.4 (9–45) 63% primiparous Ave 3.9 days labor (1–6) 52% deserted by husband after fistula 97% obstetric Muleta [12] 1210 1991– 1992 Ave 21.6 (10– 50) 56% younger than 20, 55% primiparous 77% labored more than 3 days 44% divorced after fistula, 8% had rudimentary education 97.4% obstetric 96% prolonged obstructed labor Gessessew and Mesfin [13] 193 1993– 2001 Mean 24.7 60% under 25 40% younger than 19, 47% primiparous Ave 3.6 days labor (1–7), 92% no PNC, 58% delivered at home 67% married, 81% illiterate, 93% rural 95.3% obstetric Muleta [14] 639 1999– 2000 84% younger than 20, 64% primiparous Ave 3.8 days labor, 84% labored more than 3 days, 44% delivered at home Marriage age average 14.7, first delivery ave age 17.8, 62% owned “nothing valuable,” 54% divorced Ave 149 cm 70 1975– 1980 52% age 15– 19, 70% primiparous, 18% parity > 4 67% delivered in hospital 93.6% married before age 18, 95% no education, 75% very poor 68% under 150 cm Citation Height Etiology Ethiopia Nigeria Ghatak [15] Table 1 Cont 8 83% prolonged obstructed labor Hilton and Ward [16] 656 1990– 1994 Ave 28 (7–68) 31% primiparous, Ave parity: 3 (0–17) Ave 2.5 days labor, 57% managed labor at home Gharoro and Abedi [17] 49 1992– 1997 Ave 31 (20– 65) Ave parity: 3 (1–11) Ave 3 days labor, 65% operative delivery Ibrahim et al. [18] 31 1996– 1997 60% age 13– 15, Ave age 15, 81% primiparous Ave: 4 days labor 55% divorced, 6% literate, 60% rural Ave 149 cm (140– 159) 100% prolonged obstructed labor Wall et al. [19] 932 1992– 1999 45.8% primiparous, 20% parity > 4 24% home delivery 26% married, ave age at marriage 15.5, 78% illiterate, common occupation in manual labor Typical 44 kg, under 150 cm 96.5% obstetric Ijaiya and Aboyeji [20] 24 1989– 1998 26% age 15– 19 yrs, Ave age 23.9, 50% primiparous, 32% parity > 5 91% attempted home delivery 94.1% illiterate, 24% separated/divorced 164 1977– 1992 Ave 27 62.5% married, 29% could sign name, 37% aware of own age 92.2% obstetric 80% prolonged obstructed labor (2389 cases 1970– 1994) 82% prolonged obstructed labor Ghana Danso et al. [21] Ave 26.6 43% primiparous, Ave parity 2.6 Table 1 Cont Niger 9 91.5% obstetric Meyer et al. [22] 58 2005– 2006 Ave 26.1 (16– 44) 45% primigravida Ave 2.6 days labor, 95% began labor at home, 91% at health center by delivery 62% married, ave age at marriage 15.6, ave first pregnancy at 17.3, all illiterate Median 148 cm 254 2003– 2005 Median 25 (15– 59) Median age 22 (11–45), 49% primiparous, 27.6% parity > 67.5% 2 days + in labor, Delays to EmOC mostly due to transport, 97.5% attended PNC, 84.% in labor 1–3 days 15% divorced, median marriage age 18, 69% did not complete primary education 68% under 150 cm Median 25 (14– 65) Median age 22 (13–46), 45% primigravida, median third delivery 11.5% perinatal survival, 80% delivered in hosital, 25% labor ≥ 2 days 40% separated or never married, 31% ompleted primary education, 2%comleted seconday education 70% shorter than 156 m Zambia Holme et al. [23] Kenya, Tanzania, Uganda Raassen et al. [24] 581 2001– 2003 100% obstructed labor © University of Michigan Medical School, Department of Obstetrics and Gynecology, Ann Arbor, Michigan, USA. Abbreviations: Ave, average; EmOC, emergency obstetric care; PNC, prenatal care. Obstetric causes include prolonged obstructed labor, cesarean delivery, and uterine rupture. Obstetric fistula as one of the complications of pregnancy and/or childbearing has a number of determinants which is simply analyzed using a framework which begins with remote general socioeconomic and cultural environment such as chaotic socio-economic and political systems, poverty, discrimination, power hierarchies, low self-esteem and lack of social support for 10 women. Secondly, intermediate determinants such as women’s health and reproductive status during their pregnancies, access to and use of health care resources are in most cases reflections of general socio-economic and cultural environment. Lastly, intermediate determinants set a stage for acute clinical determinants which refers to the intrapartum factors that arise when active labor becomes obstructed as well as post-obstruction period with the likelihood of fistula formation as an obstetric complication. [25] It has been widely reported in a number of articles that age at first pregnancy plays a major role in obstetric fistulation, reports from Ethiopia and Niger clearly indicate that affected women are often very young, in their early teens, carrying their first pregnancy and have low educational level while the opposite is the case in some countries like Nigeria, Ghana and Zambia where most women affected tended to be older, with higher parity (prior 4 or 5 pregnancies or children) with some being subjected to the crude traditional Hausa surgery popularly referred to as “gishiri cutting” (gishiri = salt; random cuts within the vagina with a “salt slashing knife” to enlarge the birth canal once labor obstruction sets in). These studies have common denominators which are factors like accessibility to health facilities, distance to health institutions, transportation, financial constraints and poor knowledge were frequently cited problems in many parts of Africa. In Cameroon Far North Province, amongst fistula patients aged 15-49 years, the illiteracy rate was as high as 78%, and 86% of them were teenagers at first delivery. [26] Based on comparative study from North-Eastern Nigeria, data analyzed shows that majority of patients analyzed were Fulani/Hausa, 91.2% were Muslims, 93.7% had labor obstruction, majority married early (average 14 years), and short stature (average height 146.2cm) was also a factor. Some other article states in support of the above statistics that amongst these young women, 96.3% were illiterate, no gainful employment and low social class. Ninety-six point seven 11 percent (96.7%) failed to register for antenatal care while majority lives in the rural areas, far away from a health care facility (>3km). [27] A university Hospital in Northern Nigeria reported that gishiri cutting leading to fistula accounted for 13% of cases in about 1443 patients operated upon; this practice along with packing the vagina with caustic and local medicines is common among the Hausa, Fulani and Kanuri tribes in the sub-Sahara Africa. [28] In Sudan, a descriptive, cross-sectional community-based study of 52 patients with vesicovaginal fistula who presented at the Fistula Center in Khartoum Teaching Hospital was conducted. It is clearly in support of determinants of fistula from other parts of Africa as stated in the table below even though circumcision leading to vesico-vaginal fistula (VVF) stands out in Sudan compare to other countries. [29] 12 Table 2: Contributing factors of vesico-vaginal fistula © Contributing factors of vesico-vaginal fistula (VVF) among fistula patients in Dr.Abbo's National Fistula & Urogynecology Centre - Elsadig Yousif Mohamed et al In northern Nigeria, a case-control study was carried out involving 241 fistula cases and 148 patients without fistula as controls, both cases and controls were interviewed and their records over the last 2 years were reviewed and analyzed. This retrospective study, is consistent with other studies, showed that prolonged labor constituted 75.6% of all cases of fistula, Gishiri cut constituted 6.2% of cases and other factors like earlier age of marriage (26.9%), height of women (51.9% below 150cm with the relative risk of 1.8), surgical trauma (3.1%), infection (2.1%), cervical carcinoma (1.7%) are of great importance. More so, about 49.9% of women with fistula were married as compared to 85.3% of the controls, a higher percentage of fistula patients were divorced than controls. [30] 13 4.0 DISCUSSION The purpose of this essay is to perform a peer-review and to substantiate some of the factors influencing prevalence, prevention and treatment of obstetric fistula in Africa. There is no doubt that obstetric fistula (OF) has been and is still a major public health problem. The social and economic impact of this on underdeveloped and developing nations cannot be over emphasized. OF affects thousands of women yearly and a couple of millions of them go about with fistula, mostly in Africa. There is strong relationship between OF and a number of factors like sociocultural practices, economic situation of the continent of Africa, educational status, political influences and health care availability/accessibility/affordability and these have been proven in many studies. Looking at Africa, it is a common cultural practice in part that young teenage girls are married away or actually forced into marrying older men when there are physically and psychological immature for marriage and ultimately pregnancy. Studies have shown that very high percentage of obstetric fistula occurs in very young, primipara and/or short stature women. Level of community education and knowledge of the etiology of fistula, the better the awareness of the causes of fistula at the community level the more we are likely to reduce its rate of occurrence. The truth is that OF as an obstetric complication can be reduced by delaying or discouraging teen marriages which will eventually reduce teen pregnancies. Women empowerment in Africa will change the equation, women should have a say in their sexual and reproductive life, they should not be forced or coerced into it. 14 Obviously, most affected African countries are either underdeveloped or still developing; people are living in extreme poverty, lack of good food, poor growth and development, poor living conditions and little or no financial means to cater for the family’s medical need. Poverty alleviation programs will go a long way in Africa; this will bring improvement to women and children’s health, living standard and the ability to seek medical care when deemed necessary. Women living in the remote areas of Africa where there are very few or no schools are highly uneducated; literacy level has great effect on how a woman sees her body, sees her pregnancy and her ability to make decisions in seeking medical care. Furthermore, political instabilities in most Africa nations have contributed greatly to high rate of poverty, lack of basic amenities and lack of standard health care system outside major cities. In Africa, as mentioned before there are a number of well-equipped medical centers in most African major cities, except in the in remotes areas where, in reality, majority of the people especially women and children live. Health care services are not available, non-affordable, nonaccessible, or in few area where this is available, the care is poor and inadequate in terms of equipment and staffing. Health is unaffordable for these women; some would rather stay and attempt to have a domiciliary delivery, which is affordable to them. Majority of these women who stayed at home to deliver would either develop some intra-partum or post-partum complications like fistula following labor obstruction and/or traditional gishiri cutting. The gishiri cutting is a common practice among the Hausa, Fulani and the Kanuri tribes of the subSahara region of Africa; this factor is peculiar and is one of the major contributors to high rate of fistula in this region. 15 Community education regarding problems associated with teenage pregnancy, danger in forced marriage, signs and symptoms of obstructed labor, as well as better access to medical care in order to benefit from standard care during delivery. 16 5.0 CONCLUSION Obstetric fistula (OF) is a major public health problem there is no doubt, and most importantly this is multi-factorial in etiology that could be related directly or indirectly to factors like cultural, socio-economic and religious practices, biologic, regional poverty and lack of women education and empowerment, poor health care system and political instability. The question is how do we prevent, reduce or manage fistula? We all understand and agree at this juncture that we can safely conclude that high incidence of fistula in sub-Sahara Africa is a reflection of medically inappropriate cultural practices by forcing women that are not physically and mentally mature (some have height < 150 cm) into marriages and lack of accessible, affordable and/or a well-equipped health care services. In some of these fistula “infested” regions, more government and non-governmental organization campaigns are needed and should be implemented. Better funding to educate families and communities to really understand the causes and prevention of fistula and the importance of antenatal care. There should be robust governmental policies and funding that is aimed at discouraging forced/teen marriages, teen pregnancies which will subsequently have a positive effect on maternal/child morbidity and mortality rate reduction. Health care facilities that is well equipped with well-trained health personnel. Governmental and non-governmental organizations should be put in place in these regions for quick and better obstetric intervention when necessary. 17 Conflicts, corruption and political instabilities in most Africa nations has led to increased poverty level, governments should invest more in their citizens; there should be poverty alleviation programs and fast-track education for women should be put in place, and most importantly laws should be promulgated to empower women. Lastly, more research is required to statistically establish the full impact of “gishiri cutting” on obstetric fistula prevalence in Africa. In addition, very few case-control studies on fistula in is currently available, there should more governmental and non-governmental funding to carry out more extensive studies on obstetric fistula. 18 “The opening of the Danja Fistula Center marks a great step forward for the women of Niger and all of sub-Saharan Africa . . . The fistula hospital is truly a beacon of hope which will permeate throughout the sub-Saharan region and into the rest of the world”. United States Senators James M. Inhofe, Christopher Coons, John Boozman, Mike Enzi and John Barrasso Figure 4 Worldwide Fistula Center Courtesy of Worldwide Fistula Fund 19 BIBLIOGRAPHY [1] Worldwide Fistula Fund. Africa: Obstetric Fistula fact sheet. 7 February 2012. [2] Ahmad-Rufai Abdullah. Socio-cultural and religious factors affecting obstetric fistula in an Islamic population in Northern Nigeria: An exploratory study. American Public Health Association 28 October 2008 [3] S. Ahmed, R. Genadry, C. Stanton, A.B. Lalonde. Dead women walking: neglected millions with obstetric fistula Int J Gynecol Obstet, 99 (Suppl 1) (2007), pp. S1–S3 [3] International Journal of Gynecology & Obstetrics, Volume 104, Issue 2, February 2009, Pages 85–89 [4] Obstetric Fistula is a “Neglected Tropical Disease” - Wall LL (2006) Obstetric vesicovaginal fistula as an international public health problem. Lancet 368: 1201–1209 [5] World Health Organization. The world health report 2005: make every mother and child count. WHO, Geneva, Switzerland (2005) http://www.who.int.pitt.idm.oclc.org/whr/2005/en/. Accessed April 13, 2007. [6] World Health Organization. Facts on Obstetric Fistula. March 2010 [7] Roush KM.J Midwifery Women’s Health. 2009 Mar-Apr; 54(2):e21-33. [8] Melah, G. S.; Massa, A. A.; Yahaya, U. R.; Bukar, M.; Kizaya, D. D.; El-Nafaty, A. U. Risk factors for obstetric fistulae in north-eastern Nigeria. Journal of Obstetrics and Gynaecology; 2007. 27: 8, 819-823. 20 ref. [9] Capes T, Ascher-Walsh C, Abdoulaye I, Brodman M. - Mt Sinai J Med. 2011 May-Jun; 78(3):352-61. doi: 10.1002/msj.20265. [10]. Kelly. Ethiopia: an epidemiological study of vesico-vaginal fistula in Addis Ababa. World Health Stat Quart, 48 (1) (1995), pp. 15–17 [11] J. Kelly, B.E. Kwast. Epidemiologic study of vesicovaginal fistulas in Ethiopia. Int Urogynecol J, 4 (5) (1993), pp. 278–281 [12] M. Muleta. Obstetric fistulae: a retrospective study of 1210 cases at the Addis Ababa Fistula Hospital J Obstet Gynaecol, 17 (1) (1997), pp. 68–70 [13] A. Gessessew, M. Mesfin. Genitourinary and rectovaginal fistulae in Adigrat Zonal Hospital, Tigray, North Ethiopia. Ethiop Med J, 41 (2) (2003), pp. 123–130 [14] M. Muleta. Socio-demographic profile and obstetric experience of fistula patients managed at the Addis Ababa Fistula Hospital. Ethiop Med J, 42 (1) (2004), pp. 9–16 [15] D.P. Ghatak. A study of urinary fistulae in Sokoto, Nigeria. J Indian Med Assoc, 90 (11) (1992), pp. 285–287 [16] P. Hilton, A. Ward. Epidemiological and surgical aspects of urogenital fistulae: a review of 25 years' experience in southeast Nigeria. Int Urogynecol J Pelvic Floor Dysfunct, 9 (4) (1998), pp. 189–194 [17] E.P. Gharoro, H.O. Abedi. Vesico-vaginal fistula in Benin City, Nigeria. Int J Gynecol Obstet, 64 (3) (1999), pp. 313–314 20 [18] T. Ibrahim, A.U. Sadiq, S.O. Daniel. Characteristics of VVF patients as seen at the specialist hospital Sokoto, Nigeria. West Afr J Med, 19 (1) (2000), pp. 59–63 [19] L.L. Wall, J.A. Karshima, C. Kirschner, S.D. Arrowsmith. The obstetric vesicovaginal fistula: characteristics of 899 patients from Jos, Nigeria. Am J Obstet Gynecol, 190 (4) (2004), pp. 1011–1019 [20] M.A. Ijaiya, P.A. Aboyeji. Obstetric urogenital fistula: the Ilorin experience, Nigeria. West Afr J Med, 23 (1) (2004), pp. 7–9 [21] K.A. Danso, J.O. Martey, L.L. Wall, T.E. Elkins. The epidemiology of genitourinary fistulae in Kumasi, Ghana, 1977-1992. Int Urogynecol J Pelvic Floor Dysfunct, 7 (3) (1996), pp. 117–120 [22] L. Meyer, C.J. Ascher-Walsh, R. Norman, A. Idrissa, H. Herbert, O. Kimso et al.. Commonalities among women who experienced vesicovaginal fistulae as a result of obstetric trauma in Niger: results from a survey given at the National Hospital Fistula Center, Niamey, Niger. Am J Obstet Gynecol, 197 (1) (2007), p. 90.e1-4 [23] A. Holme, M. Breen, C. MacArthur. Obstetric fistulae: a study of women managed at the Monze Mission Hospital, Zambia. BJOG, 114 (8) (2007), pp. 1010–1017 [24] T.J. Raassen, E.G. Verdaasdonk, M.E. Vierhout. Prospective results after first-time surgery for obstetric fistulas in East African women. Int Urogynecol J Pelvic Floor Dysfunct, 19 (1) (2008), pp. 73–79 [25] A Framework for Analyzing the Determinants of Obstetric Fistula Formation. L. Lewis Wall. Volume 43, Issue 4, pages 255–272, December 2012 [26] Tebeu, P. M. Bernis, L. de Doh, A. S. Rochat, C. H. Delvaux, T. International Journal of Gynecology & Obstetrics; 2009. 107: 1, 12-15. [27] Risk factors for obstetric fistulae in north-eastern Nigeria 2007, Vol. 27, No. 8, Pages 819-823 (doi: 10.1080/01443610701709825) G. S. Melah1†, A. A. Massa1, U. R. Yahaya1, M. Bukar1, D. D. Kizaya1 and A. U. El-Nafaty1 1Department of Obstetrics and Gynaecology, Federal Medical Centre Gombe (FMCG), Gombe, Nigeria Read More: http://informahealthcare.com.pitt.idm.oclc.org/doi/abs/10.1080/01443610701709825 [28] Tahzib F. Br J Obstet Gynaecol. 1983 May;90(5):387-91. [29] Mohamed, E. Y. Boctor, M. F. A. Ahmed, H. A. Seedahmed, H. Abdelgadir, M. A. Abdalla, S. M. Sudanese Journal of Public Health; 2009. 4: 2, 259-264. 16 ref. [30] Ampofo EK, Omotara BA, Otu T, Uchebo G. Trop Doct. 1990 Jul;20(3):138-9. 21
 0
0
advertisement




Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users