The UCLH Quality Improvement Framework Guy Young Head of Quality Improvement
advertisement

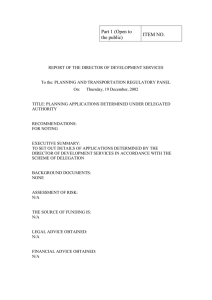
The UCLH Quality Improvement Framework Guy Young Head of Quality Improvement What is quality? • Excellence in meeting customers’ expectations • In healthcare 3 components: – Is it safe? – Is it effective? – Is the experience good for the patient? Why do we need a quality improvement programme? ne ay ril 25 Ju Au ly Se gu s pt em t be O c r N t ob ov er e D mb ec er em b Ja er nu Fe ary br ua r M y ar ch Ap ril M ay Ju ne Ju Au ly gu st Se pt O ct N ov D ec Ja n Fe b M ar ch Ju M Ap Number Falls with harm 2010-2011 30 Moderate + All harm Target 20 15 10 5 0 Composite patient experience scores 2010/11 90 89 88 87 % 86 85 84 83 82 81 80 Apr-10 May-10 Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 13 19 11 8 17 53 51 49 48 45 41 Patient board 10 23 6. 32 21 40 46 31 27 38 58 4 29 9 1. 20 47 5. 24 18 26 62 14 16 Discharge Midwives 44 lounge station 12 25 22 28 7 35 Clean Treatment utility room 15 Patient board 30 39 54 42 33 2. 56 Midwives 50 37 Dirty 43 Patient utility bathroom station 55 34 52 Ward reception desk 57 60 3. 59 61 Paeds room 36 SPAGHETTI DIAGRAM OF ONE MIDWIVES’S TRAVEL ON POSTNATAL WARD Key Findings: • In one hour, one midwife in charge of discharging women from the ward had 62 different stop offs • Clusters of stop offs at patient boards, midwives stations, bays of women being discharged and in the clean utility room • Midwife was interrupted twelve times with questions and queries from colleagues, women and their partners • Difficult to identify which woman to discharge next because of information on the patient white boards. • Ward environment increases hunting and gathering time. The UCLH Quality Improvement Framework • A way of delivering continuous quality improvement at ward/unit level driven by frontline staff – Draws on: • Transforming Care at the Bedside • Productive Ward • Lean • Aligns well with HIAs and Energising for Excellence Key themes • Transformational Leadership • Safe and Reliable Care • Vitality and Teamwork • Patient-Centered Care • Value-added Care Processes Cross cutting interventions • • • • • Intentional rounding Patient status boards SBAR The Well Organised Ward (5S) Care bundles How it is done? • Change driven by frontline staff • Staff agree areas for improvement and identify potential solutions (snorkel) • Small tests of change • Adoption and spread Results of a snorkel Small tests of change • Small means small! – One nurse – One patient – One time/one shift The PDSA Model Components • Plan an activity or improvement test • Do the activity (implement the improvement plan) • Study the Impact of the improvement plan (what was learned) • Act determine what changes are to be made in light of what you have learned. Measures Display Boards Patient status board Environments after 5s Situation to date • 8 pathfinder wards – 4 TCAB – 4 Productive ward • 6 new wards this year • From May onwards 4 wards to join every 2 months • 1 full day start up training required (5 staff)