Update to Salford Child and Adolescent Mental Health Services (CAMHS) Strategy 6
advertisement
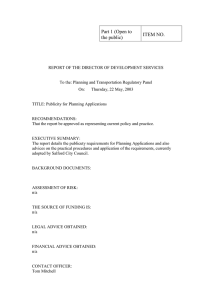
 Strategy 6")
Salford PCT 2nd Floor St. James House Pendleton Way Salford M6 5FW 6th October 2003 Tel: 0161 212 4843 Fax: 0161 212 4856 Email: Harry.Golby@salford-pct.nhs.uk Dear Colleague Update to Salford Child and Adolescent Mental Health Services (CAMHS) Strategy Please find enclosed an update to the Salford CAMHS Strategy. The original Salford and Trafford Strategy was written in 1998 and this document considers developments in national policies and guidance, provides a Salford specific focus when describing existing services and lists actions that need to be undertaken in the short / medium term. Salford Children’s Services Planning Forum is the forum that has an overview of all developments relating to children, young people and transition into adulthood and ensure consistent and cohesive implementation of a Salford Children’s Strategy. That strategy aims transform the lives of Salford’s children’s, their families and communities through effective partnership built on inclusion and empowerment. CAMHS represent an important aspect of the overall Children’s Strategy. More work is required before Salford has a CAMHS strategy that meets the vision of the Children’s Services Planning Forum. Much of this work will focus on better understanding the approaches used in schools and across the community to promote good mental health and agreeing how to maximise their contribution. In the meantime this strategy update will be used locally to agree short / medium term actions and to inform the City Council’s Health Scrutiny Committee, the Joint (PCT / Social Services) Executive Commissioning Forum and the Greater Manchester Strategic Health Authority. Yours sincerely, Harry Golby Head of Children’s Commissioning Salford Primary Care Trust Encs. (see attached distribution list) Copies to: Paul Woltman, Assistant Director (Children’s Services), Community & Social Services Directorate, Salford City Council Edna Robinson, Chair of Salford Children’s Services Planning Forum & PCT Chief Executive Alan Campbell, Chair of Salford Joint Executive Commissioning Forum Nick Clawson, Associate Director – Clinical Strategy, Greater Manchester Strategic Health Authority Members of Salford CAMHS Strategy Group Hilary Wensley, Head of (Adult) Mental Health Commissioning, Salford PCT THE MENTAL HEALTH OF CHILDREN & YOUNG PEOPLE OF SALFORD UPDATE TO CAMHS STRATEGY OCTOBER 2003 FINAL (VERSION 3) 1 INTRODUCTION Good mental health is a key component of a healthy active life. A child or young person with good mental health is more likely to fulfil their full potential later in life. There is evidence of an increase in poor mental health amongst children and young people over the last three decades, particularly amongst those who are at risk of social exclusion. The aim of this strategy is to describe the actions to be undertaken to maintain and improve the mental health of children and young people in Salford. The strategy is written in four sections: ‘context’ describes this strategy’s place in terms of national and local plans for services that will improve outcomes for children and young people; common themes for the development of services fall out of this section. ‘need’ provides an overview of the mental health needs of children and young people in Salford. ‘services’ describes some of the existing services in Salford (this section does not attempt to comprehensively describe all services – it focuses on a few that may be particularly relevant.) ‘actions’ lists what has been done recently and what else needs to be done to address the development themes locally. 2 CONTENTS 1 Introduction 2 Contents 3 Context 3.1 Scope of Strategy 3.2 National Context 3.3 Local Context 4 Need 4.1 Needs Assessment 4.2 User Views 5 Services 5.1 North West Children’s Taskforce Model – PREVENTION 5.2 4 Tier Model - INTERVENTION 5.3 Description of Some Salford CAMHS services 5.4 ‘Dyson’ Model - PATHWAYS 5.5 Investment in Salford CAMHS 6 Actions 6.1 Recent Progress 6.2 Actions to be Undertaken 3 CONTEXT 3.1 Scope of the Strategy This strategy has relevance to all children and young people in Salford, whether they are resident in the area, looked after by Salford Social Services, registered with a Salford GP, go to a Salford school or are placed in an independent sector special school. It applies to them from when they are born to the point that they are no longer receiving ‘children’s services’ and their care, where appropriate, has been handed over to adult services (in the vast majority of cases children and young people are aged 0 –19.) It applies when the child or young person is well and are trying to maintain their mental health, when the first signs of a mental health issue is recognised (whether this by the child themselves, a family member, friend or professional), throughout the period that they are receiving an intervention to improve their mental health, until they no longer require that service either because their mental health has been restored or because they have passed through transition into adult services. 3.2 National Context Green Paper ‘Every Child Matters’ The government’s vision for children and young people can be summarised in the five outcomes described in the new Green Paper ‘Every Child Matters’, these are: being healthy: enjoying good physical and mental health and living a healthy lifestyle staying safe: being protected from harm and neglect enjoying and achieving: getting the most out of life and developing the skills for adulthood making a positive contribution: being involved with the community and society and not engaging in anti-social or offending behaviour economic well-being: not being prevented by economic disadvantage from achieving their full potential in life. This vision sets considerable challenges if the agencies across the education / health / social care spectrum are going to help all children and young people achieve their full potential, particularly those children who are at risk. Children’s National Service Framework ‘Getting the Right Start’ Emerging Findings One element of the NSF emerging findings relates to the mental helath and psychological wellbeing of children and young people. The key themes in the document are: commissioning: effective, high quality, joint commissioning arrangements across health, social services and education partnership: joint provision of services and smooth transition between services across health, education, social care, youth justice and voluntary agencies developmentally appropriate care: clarity about the age range CAMHS serve and better transition to adult mental health services evidence based practice, training and a skilled and competent workforce: matching skills and competencies of workforce across whole CAMHS service to local need service composition: ensuring services have the appropriate critical mass of staffing and supporting infrastructure (e.g. appropriate IT, admin, buildings, etc.) to be sustainable access: ensuring services are managed and delivered in a way that the children and young people who need them can access them user views: enabling service users and their families / carers can influence the services that are offered audit and outcomes: routinely collecting and using information that demonstrates the effectiveness of services Other Developments The Green Paper and NSF builds on a number of other relevant publications and strategies: Keeping Children Safe - the response to Lord Laming’s report which highlighted a failure of the relevant agencies to intervene early enough, in a properly co-ordinated way, to prevent the death of Victoria Climbie Getting the Right Start: The National Service Framework for Children and Young People which is being developed and will describe a 10 year plan for services, including CAMHS, to meet new standards for services The Kennedy Report into the children’s heart surgery at the Bristol Royal Infirmary which highlighted the importance of designing children’s services from the child’s point of view Quality Protects - a programme to improve services for some of the most vulnerable children in our society – those who are looked after by local authorities; considering issues such as placement stability, support for care leavers, children and young people’s participation, partnership working and services for particular groups of children (e.g. disabled, ethnic minorities, refugees, etc.) Youth Justice Board which provides expert advice on prevention of offending amongst young people through earlier provision of multi agency support for families and juvenile sentencing reforms Full Service Schools which will bring together services previously provided from different location, onto a single site – the local school, for example health education and promotion, housing, teenage pregnancy, crisis intervention and community policing advice Sure Start, Sure Start +, Teenage Pregnancy Grant which provide extra resources to improve the multi agency response to the needs of young parents and young children in deprived areas. These developments bring significant extra resources to Salford, for example in 2003/4 Salford’s Sure Start revenue allocation is £2925k, Sure Start+ £118k and Teenage Pregnancy £135k. Some of the services provided through these developments will help maintain and improve the mental health of children and young people for example additional speech therapy, reading skills projects, domestic violence services and sex and relationship advice services. Salford Children’s Fund brings an investment of £5.5m to the deprived areas of the city over a five year period, in order to promote and develop preventative services for 5-13 years olds. Over 60 different projects are being supported and are to be externally evaluated. Most , if not all, of these projects have a role in maintaining and improving the mental health of the children and young people who are involved, 5 specifically target this area – Circle Time Training, Young Runaways, Triple P, Child Witness Support and Pyramid Clubs. Education legislation such as the Special Educational Needs and Disabilities Act which promotes the inclusion of all young people Many of these strategies were brought together in relation to CAMHS in Health Service Circular / Local Authority Circular HSC 2003/003: LAC (2003)2 ‘Child and Adolescent Mental Health Service (CAMHS) Grant Guidance 2003/04.’ This document described increased allocations to councils, alongside increases to PCT’s baseline allocations, to deliver ‘comprehensive CAMHS services’ in every locality by 2006. A comprehensive CAMHS service is described in several ways: Underpinning principles to inform the commissioning and delivery of services Range of services to meet the full range of users needs Workforce and training to ensure the skills and competencies required to deliver the service are available Organisational arrangements to ensure CAMHS services and their interfaces with other services are effectively managed. In total in the next two years in addition to its current ‘core’ allocation Salford (City Council and PCT combined) will receive in excess of £550,000 ringfenced funding for CAMHS services. Other sources of funding are available through Children’s Fund, Sure Start, Education Authority and schools allocations National Good Practice in CAMHS Various publications (e.g. Department of Health (November 2002) What’s New: Learning from the CAMHS Innovation projects, Alexander T. (November 2002) A Bright Future for All: Promoting Mental Health in education, Meltzer H., Gatward R., Goodman R., Ford T. (2000) The mental health of children and adolescents in Great Britain, Roberts H. (2000) Barnardo’s: What works in reducing inequalities in Child Health, Ashton C. (2001) Promoting Children’s Mental Health within Early Years and School Settings, Audit Commission (1999) Children in Mind: child and adolescent mental health services) reveal that effective CAMHS services have a number of characteristics in common, including: Strategy. Child and adolescent mental health data shows strong inequalities, where poorer children are more likely to experience high levels of mental distress. It is crucial that the overall direction of CAMHS relates closely to the strategies of other agencies working with children to improve their life chances. A clear set of aims and objectives should be articulated, to identify the opportunities for reducing inequalities through joint work where it would add value. Monitoring frameworks are necessary to identify areas of local progress. The NSF will provide a source of good practice standards against which services will need to be monitored. Partnership working. Clear and consistent leadership is needed to develop co-ordinated and integrated approaches. Effective CAMHS have strong relationships with local education authorities, schools, social services and other parts of the health service. In addition, there are numerous opportunities for joining up with the voluntary sector and Connexions. These partnerships should be formed at strategic levels, through established high-level mechanisms; they should also exercise their ability to influence agendas to promote well-being for young people more generally. Multi agency approaches are very effective and should be developed. Therefore, partnerships should be developed at operational levels; for example, CAMHS should offer advice, training and support to partner agencies working with young people and their families. Accessibility. CAMHS must be accessible for young people; they should operate at times when young people are able to use them, and in locations that are not intimidating or difficult to find. Similarly, different models should be used, including outreach, which take the service out to young people, especially for those in communities that have not always benefited from statutory provision. Appropriateness. A range of services should be made available depending upon the needs of young people and the realities of their lives. It should be recognised that they, and their families/carers, have diverse cultural, social and individual needs (for example child from black and ethnic minority communities). Different interventions are necessary to meet diverse needs - taking into account the range of experiences which might indicate poor mental health - including therapies, advice and support. Acceptability. CAMHS should provide non-stigmatising environments, which welcome young people, where staff members respect their diversity and difference. Involvement and participation. Young people, their families and their carers should be systematically and meaningfully involved in the design, implementation and evaluation of services. Adequate resources. CAMHS services should be adequately resourced, using benchmarks and evidence of good practice as means of assessing appropriate funding. Given the multi agency nature of the work, funding should be provided from a range of sources. 3.3 Local Context Salford Salford is a medium sized metropolitan area within Greater Manchester with a population of around 215,000 of whom approximately 20.4% are aged under 16. In common with many other urban communities with an industrial heritage there are pockets of very high levels of deprivation across Salford with nine of the twenty wards falling within the lowest 10% of wards nationally in the Index of Multiple Deprivation 2000. Five of the inner city wards have a child poverty index score higher than 66.4. Educational attainment within the city is below the national average but rising. Children’s Services Planning Forum Local organisations have committed to work together to achieve the best outcomes for children and young people. This work is overseen by the Local Strategic Partnership and within that framework the Children's Services Planning Forum, which is chaired by the PCT Chief Executive, works to 5 key aims for children in Salford: to live in nuturing and well supported families to have high levels of achievement and aspirations to live in, and make a positive contribution to, a community which they respect and which respects them to be able to access relevant and welcoming services to grow up healthy and to minimise the impact to their potential of any health disadvantages, illness or disability The CSPF is made up of representative of all the agencies that deliver services for children across the city. This includes the voluntary sector, as well as the statutory agencies, which has an equally important role in shaping and delivering services. Integrated Children’s Services Salford’s application to become a Children’s Trust Pathfinder Site is a clear statement of the vision to develop integrated services across health / social care / education. Integrated services are expected to achieve easier access through a single point of entry, joined up assessment to reduce the need for children and families to retell their story and better links between services to ensure there are no gaps in provision. Although the application to become a pathfinder was unsuccessful the City Council and Primary Care Trust are continuing to take this work forward. This will be via a phased approach initially through the creation of a joint commissioning function and then by a gradual roll out of integrated services for children, young people and families. CAMHS services are one area where health, social services, education and independent / voluntary sector services all have a contribution to make, so will be a fundamental part of Salford’s integrated children’s services. The CAMHS services, services for sick children and services for disabled children need to be integrated. The re-configuration of Salford’s children’s health services presents an opportunity to implement the necessary changes within Salford’s CAMHS services. Royal Manchester Children’s Hospital, which provides secondary (district) and tertiary (specialist) health services for Salford’s children and is the base for the Tiers 2/3 CAMHS team (see Section 5.2), is to close in 2008 and tertiary services to transfer to the central Manchester site. In response Salford PCT is planning a development of community based children’s health services building through the local investment finance trust (LIFT) redevelopment of community based facilities. The Pendleton LIFT centre will act as an important resource for Children’s Services across Salford and will be the base for the Tier 2 /3 CAMHS services. New hospital based services for children will also be developed on the Hope site as part of the Salford Health Improvement for Tomorrow (SHIFT) private finance initiative. The Education and Leisure Directorate work within a framework which promotes the empowerment of children and young people, their parents / carers and all learning settings. All teams within the Directorate from Early Years to the Youth Service, supports a capacity building strategy based on delegating resources to those working with children and young people, providing advice, guidance and training to those partners and challenging expectations and practice. While all teams contribute to this strategy, the Inclusion and Access Division provides a specific focus on supporting vulnerable young people in Salford. In promoting good mental health all primary, secondary and special schools have a vital role within the CAMHS strategy. The specific teams working with children / young people, parents / carers and learning settings includes educational welfare, educational inclusion, educational psychology and SEN support. The existing children’s division of Community and Social Services will be part of the Salford’s integrated children’s services. The initial focus will be around developing a common Identification Referral and Tracking system for Salford underpinned by a single assessment process. Initiatives such as Sure Start, Children’s Fund, Connexions will mean an increasing emphasis of preventative work within these services over time. 4 NEED 4.1 Needs Assessment Summary A quarter of Salford’s population is aged 19 or under. Around 4000 children or adolescents are likely to have some form of mental disorder in Salford Around 270 looked after children in Salford will have some form of mental disorder. Five of the six wards in Central locality are in the top 2% most deprived child poverty wards in the country. Younger People Just over a quarter (25.8%) of the population of Salford is aged 19 and under. In absolute terms, South locality has the largest population of people aged 19 and under. According to the 2001 Census approximately 19,500 people aged 19 and under lived in South locality, compared to around 13000 in both West and Central locality and 9000 in North locality. Central locality has the highest percentage of the population aged 19 and under (26.9%) and North Locality the lowest percentage of population aged 19 and under (24.1%). Figure 1. Figure 1: Localities - percentage aged 19 and under Localities - percentage of population aged 19 and under 27.5 Source: ONS - Census 2001 Percentage of locality population 27.0 26.5 26.0 25.5 25.0 24.5 24.0 23.5 23.0 22.5 Central locality North locality South locality West locality At an electoral ward level, Kersal (33.9%) has the highest percentage of population aged 19 and under. Along with Kersal, Little Hulton (30.3%), Broughton (29.7%), Winton (29.5%) and Irlam (28.5%) are the five electoral wards with the largest percentage of population aged 19 and under. Prevalence Of Mental Health Disorders In Children And Adolescents In Salford The ‘mental health of children and adolescents in Great Britain’1 states that among children aged 5–15 years, 9.5% had some form of mental disorder. 5% had clinically significant conduct disorders; 4% were assessed as having emotional disorders (anxiety and depression) and 1% were rated as hyperactive. The ‘less common’ disorders (autistic disorders, tics and eating disorders) were attributed to half a per cent of the population. If these prevalent rates are applied to the Salford population aged 5 to 19 it is estimated that around 4000 children and adolescents will some form of mental disorder, 2150 conduct disorders, 1700 emotional disorders, 430 hyperkinetic disorders and 215 less common disorders (Table 4). Table 1: Estimated numbers of children and adolescents in Salford with mental health problems (from national prevalence rates) 5-10 any 1400 Prevalence of mental disorder Conduct disorders 780 Emotional disorders: 560 Anxiety 525 Depression 35 Hyperkinetic 255 disorders Less common 85 disorders 11-15 1600 5 to 19 4085 910 810 675 260 200 2150 1720 1634 387 430 88 215 Prevalence Of Mental Health Disorders In Looked After Children The “Mental health of young people looked after by local authorities in England”2 estimates the prevalence of mental disorder among looked after children to be 45%, a rate over four times higher than that for young people generally. 37% of looked after children will have a clinically significant conduct disorder, 12% emotional disorder and 7% of looked after children will have a hyperkinetic disorder. A further 4% of looked after children will have a ‘less 1 Meltzer H, Gatward R. The mental health of children and adolescents in Great Britain. ONS. 1999 2 Meltzer H, Corbin T, Gatward R, Goodman R, Ford T. The Mental Health of young people looked after by local authorities in England. ONS. 2003. common’ disorder (such as pervasive developmental disorders, tics and eating disorders). If these prevalence rates are applied to the population of looked after children in Salford it would mean that approximately 270 looked after children in Salford will have some form of mental disorder. About 220 will have a clinically significant conduct disorder, 70 will have an emotional disorder and 40 will have a hyperkinetic disorder and around 25 looked after children will have one of the less common disorders. Table 2: Estimated numbers of looked after children and adolescents in Salford with mental health problems (from national prevalence rates) Prevalence of any mental disorder Conduct disorders Emotional disorders: Hyperkinetic disorders Less common disorders 5 to 19 270 220 70 40 25 Autistic Spectrum Disorders (ASD) Understanding of ASD is developing. It affects at least, 60 per 10,000 children under 8 years, of whom 10 to 30 have narrowly-defined autism. This national increase in prevalence is replicated in Salford. It is a developmental disorder in which the presentation varies with age and, in any one individual, varies over time. By adulthood about one third of individuals with ASDs have developed epilepsy. The association of ASDs with learning disability is not well understood and the risk of low IQ in ASDs may be lower than previously thought. Diagnostic instruments are being developed which mean more children and adolescents without learning disabilities are being identified on the autistic spectrum. Nevertheless a substantial number of children and adolescents with identified ASDs have learning disabilities. Many of these present with atypical ASDs, and there is a significant association with “challenging behaviour”. The high correlation between ASDs and learning disabilities means that this will have implications for all LD camhs provision, particularly as in combination these present a higher risk of challenging behaviours. Risk Factors Factors which increase the risk of developing mental health problems in childhood include: Family poverty Family discord or separation A parent with mental illness Parents who misuse drugs Chromosomal or other genetic abnormalities Brain damage in the child Physical, emotional or sexual abuse (including bullying or racism) Severe trauma The child having a learning disability, language or communication problem.3 Being a looked after child Chronic physical illness, especially that which includes physical disability and damage to the central nervous system These are risk and not causal factors. The extent to which any child experiencing these risks goes on to suffer a mental health problem will depend on a complex range of interactive issues. Child poverty Family poverty has been identified as a risk factor in developing a mental health problem.2 The Index of Multiple Deprivation 2000 (IMD 2000) measured derivation across six domains using a basket of indicators. Overall, Salford is the 28 th most deprived local authority in the country out of 354 local authorities. The Child Poverty Index score formed a part of the overall deprivation measure. In Salford, child poverty scores are worse than overall deprivation scores. Of 8414 electoral wards nationally, Ordsall was ranked the 12th most deprived ward in terms of child poverty. Blackfriars (21 st), Pendleton (54th), Broughton (135th) and Langworthy (153th) are in the top 2% of the most deprived child poverty wards. Additionally, Little Hulton (276th), Winton (479th) and Weaste and Seedley (656th) are in the most 10% of child poverty deprived wards. With five of the six wards in Central locality being in the top 2% most deprived child poverty wards in the country, this is by far the most deprived locality in Salford. Educational attainment The prevalence of mental disorders among children increases with a decrease in the educational level of the interviewed parent. 15% of children of parents with no educational qualifications had a mental disorder compared with 6% of those whose parent had at least a degree level qualification. 4 Department of Health. Child health in the community – a guide to good practice. NHS Executive.1996. 2 The University of Liverpool. Health Prospects for Young Citizens of the North West. A Special Report for the Regional Director of Public Health. 1998 4 Meltzer H, Gatward R. The mental health of children and adolescents in Great Britain. ONS. 1999 3 Taking the population as a whole, central locality has the highest percentage of residents with no qualifications (37.7%). West locality has the lowest percentage of residents with no qualifications (31.7%). Lone parent households The ONS survey ‘the mental health of children and adolescents in Great Britain’4 states that the children of lone parents were about twice as likely to have a mental health problem than those living with married or cohabiting couples: 16% compared to 8%. Across the whole of Salford, 8.6% of households are those with lone parents bringing up dependent children compared to 6.5% of households in England and Wales. Localitities: Percentage of lone parent households. Lo c a lit ie s - pe rc e nt a ge o f lo ne pa re nt ho us e ho lds 12 Percentage of households Sour ce: ONS - Census 2001 10 8 6 4 2 0 Central locality 4.2 North locality South locality West locality User Views There is a history of productive user involvement in adult mental health services. User involvement in Salford CAMHS services is much more patchy. Involving children and young people in the development of services for them is a key principle underpinning the work of the Salford Children’s Services Planning Forum and is becoming a key action area for all services to take forward. Through the Children’s Services Planning Forum the resource and intelligence within the city will be joined up to create a comprehensive strategy for involvement. Part of this will include the appointment of a worker to take the lead on developing local capacity for involvement work around health services. This individual represents a resource local CAMHS services will utilise. 4 Meltzer H, Gatward R. The mental health of children and adolescents in Great Britain. ONS. 1999 42nd Street (see section 5.1) was commissioned by Salford West Primary Care Group in 2000 to understand the mental health needs of young people in West Salford. (The project worked with young people aged 14 – 25.) The original remit was expanded to reflect the creation of Salford PCT in 2001 and the report ‘Under Pressure’ reflects the views of young people from across Salford. The report identified a number nationally recognised social factors that affect young people’s mental health needs (e.g. family life, abuse, crime, education, discrimination, drugs, etc.) and some that seemed to be of particular relevance to young men in Salford (e.g. macho masculine identities, poor economic opportunities and changing economic roles.) Some of the strategies these young people used to cope with these stresses (e.g. substance use and misuse, self harming and suicidal activity) may further exacerbate their mental health needs. The report made a number of recommendations relating to existing services: Establish peer support / mentoring system, including face-to-face and Internet services Increase range of flexible, young people friendly support services (e.g. out of hours, drop-ins, outreach and services sensitive to disability, gender, sexual identity and ethnicity issues Improve access to range of therapeutic and other support services as an alternative to / alongside medication Establish a city-wide multi-agency training programme around CAMHS for statutory and generic workers And some proposals for new services: System to promote young people’s participation in the development of services Further research into the needs of specific groups A CAMHS co-ordinator for Salford with a remit around mental health promotion Drop in Tiers 1-3 services, services with a focus on young men’s needs, interventions suitable for those wishing to start work Supported housing / rehab centres facilitating independent living of young people needing residential / inpatient care and a residential crisis centre for young people. In addition the Victims of Crime Partnership has involved young people in considering issues around domestic violence. One of the key messages coming out of this work is the desire for more counselling in schools. Some of these issues have already been addressed (see next section on Services) others need to be picked up in the actions falling out of this document. 5 SERVICES This section describes some current CAMHS services in Salford. A variety of models have been used to provide an overview of CAMHS services, each focuses on different of the overall provision and adds richness to the description of CAMHS services in Salford. It is not possible to describe every service in detail but a few have been highlighted where they are of particular relevance / interest. 5.1 North West Children’s Taskforce Model - PREVENTION The North West Children’s Taskforce’s guide for commissioners of CAMHS services published in early 2003 represented CAMHS services through the model below: There are clear links between this model and the 4 tier model (see section 5.2 – children with lower levels of need will tend to access lower tier services. However as the models have been developed from different starting points (one based on need, one based on the way the workforce is organised) it is not clear exactly how well they map together. For example do / should all children in the mental health difficulty category receive Tier 2 services or do / should some receive Tier 1 and some Tier 2 as well. All Children / young people Risk factors but not problem yet 100% Mental health difficulty 20% Mental health problem 10% Mental / psychiatric illness ? 2% Universal Services MH Promotion (and some primary prevention) Children and Young People at Risk – Targeted Services Primary Prevention & Early Intervention (and some secondary prevention) Secondary Intervention and Prevention (and some tertiary prevention) Tertiary Intervention and Prevention A strength of this model is that it describes services from the perspective of all children and young people, highlights the importance of the promotion of good mental health for children and young people and the fact that most children and young people who receive a mental health ‘intervention’ will receive it from their families, friends, communities and universal services (e.g. schools) rather than from targeted or specialist CAMHS services. 5.2 4 Tier Model - INTERVENTION A 4 tier model for CAMHS services was described in Together We Stand published by the Health Advisory Service in 1995. This model describes each service by considering by whom and how it is provided, with children and young people with more severe problems requiring input from a higher tier of service: Tier 1: Represents teachers, social workers, voluntary agencies and primary healthcare staff, etc. Tier 2: Represents CAMHS professionals (clinical psychologists, psychiatrists, nurses and other mental health workers) working as individuals with particular children and their families. Tier 3: Represents CAMHS professionals working in teams to deliver a multi-professional response to an individuals needs Tier 4: Represents highly specialised services such as inpatient facilities This is the nationally recognised model for CAMHS and allows comparison between Salford and other areas and a common language which reflects the concept of the graduated response used in education. 5.3 Description of Some Salford CAMHS Services PREVENTION In Salford there are a range of services that fall within the CAMHS health promotion / prevention remit, many of these are funded through the Salford Children’s Fund and a few are described below: World Wide Web Information around issues related to young people’s mental health is available on the World Wide Web, much in a form that is accessible to young people. www.ru-ok.com is a site that has been developed by mental health professionals locally and aims to help teenagers assess their strengths and weaknesses and access advice. Bullying Policies A survey of primary and secondary schools across England showed bullying is widespread with 44% of children reporting they had been bullied at some point and 27% reporting they had bullied others. It is slightly more common amongst boys than girls and decreases with age. Bullying can involve physical, mental or indirect (e.g. via gossip, emails, text messages, etc.) abuse. Victims may be reluctant to attend school and are often absent. They may be more anxious and insecure than others and being bullied may lead to anxiety, depression, loneliness and lack of trust in adult life and in extreme cases attempted suicide. Victims may present a variety of symptoms to health professionals, including fits, faints, vomiting, limb pains, paralysis, hyperventilation, visual symptoms, headaches, stomachaches, bed wetting, sleeping difficulties and sadness. Much of the work to tackle bullying is being driven nationally but led locally by schools. ‘Don’t suffer in Silence’ an anti-bullying pack has been circulated to all schools and offers practical advise on developing schools anti-bullying policies, through awareness raising and consultation, policy implementation, monitoring and evaluation. The pack promotes a range of good practice for example exploring issues within circle time, building ‘circles of friends’ around vulnerable pupils, setting up support groups, pupil volunteer ‘befrienders’, mediation by peers and adults, counsellor based services, assertiveness training and involving parents at various stages. Behaviour Education Support Teams (BEST) BEST teams have been set up as part of Salford’s Behavioural Improvement Programme which is part of the national strategy to reduce street crime. Set up in 4 secondary schools and their feeder primaries, multi-agency BEST teams offer intensive support to pupils, their teachers and families who are at most risk of non-attendance or exclusion from school. One member of these teams is a CAMHS professional and has a specific role about enabling appropriate access to CAMHS services. Triple P Parenting Parents have a strong influence on their child’s educational development, behaviour and mental health. People learn how to be parents from their families, their community, the media and occasionally from people who work in children’s services (e.g. GPs, health visitors, teachers, social workers, etc.) Currently a number of parenting techniques are taught by different staff in Salford (for example Webster Stratton and Parent Survival courses (used by the Child and Adolescent Mental Health team), Hanen (used by speech therapists), etc.) Processes such as participatory appraisal carried out with the public in a number of areas across the city (e.g. Seedley, Langworthy, Ordsall, Kersal and Charlestown) have shown Salford’s parents want themselves and their families to receive consistent parenting advice. The Children’s Fund in Salford has commissioned the PCT to lead a two year project that aims to trial a single, coherent parenting strategy, Triple P, within one area of the city (surrounding the schools that the Behaviour Education Support Teams work with.) Triple P is a comprehensive early intervention to support parenting and intervene effectively in the management of childhood behaviours. There are 5 levels of Triple P, level 1 provides all parents with basic parenting information and subsequent levels provide progressively more advice to parents and is increasingly targeted towards families with higher levels of concern and difficulty about their child’s behaviour. The Salford project will trial the use of the first 3 levels (the Webster Stratton programme will continue to be used for the highest level of need.) The project will entail understanding current parenting activity, identifying training needs, training staff in the Triple P approaches and then delivering Triple P parenting. Evaluation of the project is being led by the Clinical Psychology Research Department of Manchester University the evaluation will consider the value of using the Triple P approach in Salford. In addition the project will identify the barriers to using Triple P to provide a single coherent parenting strategy across the whole of Salford. To inform the evaluation of this project, teachers asked over 400 children to get their parents to complete questionnaire on their behavioural and emotional adjustment. Over 2/3 of the questionnaires were returned (60% from girl’s parents, 70% from boy’s) and this high response rate is felt to reflect the importance of the issue to parents and the approaches the researchers used to incentivise the children to take part. Salford Foundation – Pyramid Clubs Salford Foundation works to improve links between the business and education sectors of the city. Since its inception in 1991 the Foundation has developed and now runs a wide variety of volunteer schemes for example mentoring, Millenium Volunteers, New Deal mentoring for job seekers, peer mentoring in high schools, etc. A new scheme has recently been launched – Pyramid Clubs. This is a preventative approach targeted at 7-8 year olds. 10 primary schools within Salford have signed up to take part and professionals and parents will screen children to identify those who could be at risk of developing mental illness (e.g. low self-esteem, poor social skills, stressed, etc.) 10 children in each school will be invited to join a Pyramid Club which will be run by trained volunteers and, through fun and play, help the children develop confidence, friendships and coping skills. There is evidence that such approaches can improve the children’s well-being later in life. INTERVENTION Tier 1 in Salford In common with other areas Salford Tier 1 servcies are delivered by a variety of agencies: Health: GPs, health visitors, school nurses, community paediatricians, A&E staff, hospital doctors Social Services: Residential units, fieldwork teams, foster carers Education: High school counsellors, teachers, educational welfare service, education psychology service, special schools. 4 high schools in Salford also have recently put in place multi-agency Behaviour Education Support Teams which will provide early intervention for pupils who are showing signs of emotional behavioural problems or who are at risk of developing mental health problems. Other: Youth Offending Teams, Drug & Alcohol Teams, Charitable, Voluntary and Independent Sector Services There are also a number of more targeted Tier 1 services in Salford: ADD/ ADHD Family Support Centre – this is a charitable centre based in Little Hulton, Salford, which provides various services for families of children with attention deficit disorder and related syndromes from Greater Manchester. The services provided include advice, resources (books, video’s, etc.), trips and activities, group work, solicitors clinic, etc. Pro-Contact – Salford has the only Pro-contact centre in the North West of England. This relatively new independent service provides opportunities for supervised contact between children and parents who have been separated potentially as a result of offences which have been dealt with through the legal system. In addition to facilitating safe contact the service may provide assessment of needs and therapeutic intervention such as parenting, counselling and anger management. Relate – this is a charity that aims to support people to build better relationships through the provision of counselling services. In addition to counselling and psycho-sexual therapy services Relate provides a young person’s service to help young people come to terms with family break-up and re-organisations. Crossroads – this charity provides support to carers of dependent adults and children. In Salford it provides a well developed service, for example domiciliary respite care as well and activities, for children with chronic health conditions and challenging behaviours, co-ordinated with provision by all statutory agencies. Brief Intervention Team – this service provides a short-term, intensive solution focused approach for families in crisis with children at risk of being excluded from school or looked after by the Local Authority. The service is staffed by employees of the Local Education Authority and Social Services who use a clinic based approach, engaging with young people and families to look at how change can be effected. Tier 2 in Salford Most referrals from Tier 1 services to CAMHS Tier 2 / 3 services are from GPs, school nurses and social workers. A significant proportion of the children and young people will be known to other services, all should be known to education services, and may have a variety of related needs. The CAMHS professional will often need to discuss cases with the referrer to ensure the CAMHS response is in line with the clinical priority of the CAMHS issue. The services are primarily provided by clinical psychologists, but are also provided by psychiatrists, child psychotherapists, nurse practitioners and child mental health practitioners. The treatment / intervention used is based on the assessment of the child and their family’s needs and can include individual work with the child and the family, parent training and parenting groups. Core services are provided at the RMCH site however several projects have been funded which provide Tier 2 services in other settings, for example outreach work in Little Hulton, Lower Broughton, Ordsall and Eccles, Life Start parenting courses in a community setting for hard to reach families in a Sure Start area, clinical psychology input to the Diana team for home nursing of children with life limiting illnesses and school based services for children of refugees and asylum seekers (funded through Action for Children in Conflict.) Tier 3 in Salford Salford Tier 3 services are accessed by the same means as Tier 2 services. Tier 3 is delivered by psychiatrists, clinical psychologists, child psychotherapists, child mental health practitioners and nurses. The services comprises a comprehensive assessment and multi disciplinary intervention which is usually more intensive and / or for a longer period of time than for Tier 2. Specific elements of the service include referral onto more specialist services (e.g. early onset of psychosis, severe anorexia), the day unit (with CAMHS, education and social work input) and a 24hour on-call rota for emergencies. The Salford Therapeutic Advisory Referral Service for Looked After Children (STARLAC) improves access to Tiers 2 / 3 CAMHS services for looked after children and extends the consultation / training / support given to local foster carers and children’s residential units. Tier 4 for Salford Tier 4 services are commissioned on a large population basis, Salford’s services are commissioned as part of the Greater Manchester provision. NHS Tier 4 services in Greater Manchester include: ward 15, Booth Hall Hospital, Central Manchester and Manchester Children’s University Hospitals NHS Trust (for children under the age of 15) McGuiness Unit, Prestwich Hospital, Bolton, Salford and Trafford Mental Health Trust (for 13 –18 year olds) Salford Social Services also provides the Barton Moss secure unit for young offenders. Health / social care and education agencies have recently developed a tripartite funding protocol to place children and young people usually outside the area in independent sector provision if local services cannot meet their needs. 5.4 The ‘Dyson’ - PATHWAYS The ‘Dyson’ model, see below, was based on a model developed through the Salford Health Investment for Tomorrow project and has been developed to: describe all services (including health / local authority / voluntary sector) that are available to children and adolescents from Salford with mental health problems concentrate on the connections between the services be tested / challenged by services (initially the CAMHS strategy group) be used as a planning tool to help identify gaps and duplication. This model highlights the importance of understanding CAMHS as a whole system of services that need to work together as children and young people move from one part to another. It highlights the importance of the training / consultation / liaison role of the Tier 2 / 3 CAMHS professionals to assist the development of appropriate skills and competencies such that Tier 1 services can manage children and young people with low level needs and can quickly assess and identify those few who have high needs and need a more specialist input. The model also highlights the variety of routes into different services and the potential for children and young people to be stuck or going round in circles if there are not clear pathways into appropriate services for them – the ‘Dyson’ effect. Understanding the Dyson Diagram The model is a graphical representation of current CAMHS in Salford. A few examples of different services are listed in each category and links between the categories are shown. Broadly speaking services towards the bottom of the diagram represent ‘higher end’ services. The size of a box does not represent the importance of that service, the numbers or needs of its users or the resources it requires and the size of the arrows does not represent the numbers of referrals from one part of the system to another. Current CAMHS Services in Salford (Version 2.1) – the ‘Dyson’ model Universal Services (mainly open access) e.g. School Counselling, Social Work, 42nd Street, www, Parenting Groups, Anti Bullying Specialist CAMHS Intake Meeting Clinical Child Psychology e.g. Outpatient services, Clinics, Day Unit, STARLAC CAMHS Psychiatry e.g. Outpatient services, Clinics, Day Unit Tier 4 e.g. McGuiness Unit, Booth Hall, Independent Sector Outrach Services, Training, Networking & Liaison Outreach Services, Training, Networking & Liaison Targeted Services (mainly limited access) e.g. ADD / ADHD Centre, Crossroads, Brief Intrvntn Team, Relate, Pro-Contact Refe rers e.g. GPs, Soci al Work ers Authorities across the country are investing in Identification, Referral and Tracking schemes to improve co-ordination between partner agencies who are working with vulnerable children, young people and their families. A key element of this investment relates to the development of integrated IT systems. In Salford the system will be underpinned by the Family Action Model. This model aims to enable vulnerable families who fall below the threshold for social work intervention to access co-ordinated multi-agency services. Locality based FAM co-ordinators have been recruited and one of these will take a lead on ensuring CAMHS services are linked into this development. The CAMHS strategy group has agreed clear pathways into services need to be developed for children who are: disabled looked after having special / additional educational needs at risk of abuse or living with domestic violence in transition in a highly mobile families a young offender gay or lesbian in a family that is breaking up or having suffered a bereavement a carer having learning related difficulties out of education as well as those who have a diagnosed mental illness. The national CAMHS mapping exercise indicates that nationally 48% of Tier 2 / 3 staff time is spent in direct clinical contact, 20% on consultation, supervision and training and 22% on admin and case management. Salford CAMHS staff consult, train and liase with the following services: Social Services All residential units Fieldwork teams Foster carers Brief Intervention Team Education Most high schools Educational Welfare Education Psychology Special Schools Health Health visitors School nurses Community paediatricians Other Youth Offending Team Young Person’s Substance Misuse Team The Salford CAMHS tier 2/3 team also has strong links with the Manchester University Department of Child & Adolescent Psychiatry. These links mean staff are supported in a wide range of clinical research, training placements for psychiatrists, clinical psychologists, nurses and social workers are provided and various other education and training activities are developed and undertaken. Resources Invested in Salford CAMHS Due to the range of services that make up a comprehensive CAMHS service and the range of sources of funding it is difficult to identify the resources that are invested in Salford CAMHS services in their entirety. The table below provides some figures: Commissioning Organisation PCT – Core Contracts Service Provider Service Central Manchester and Manchester Children’s University Hospitals NHS Trust PCT – Non-NHS Salford City Council Small Grants Jewish Society Making Space Crossroads After Adoption Homestart Reserves Contribution to out of area placements STARLAC Cornerstone Crossroads 42nd St STARLAC Psychiatry –outpatients Psychiatry – inpatients Psychiatry – day care Psychology Outreach STARLAC Diana Nursing Child Protection ADD Centre Project Smile Family Support ADD Centre - PCT – Joint Finance PCT –Packages of Care Social Services – Core CAMHS Funding £000s 326 27 74 365 103 141 12 9 18 15 13 5 18 21 Notes Figures are estimates of 02/03 outturn. Accuracy of activity and costs needs to be clarified. Figures are 02/03 outturn Figures are 02/03 outturn 67 Figures are 02/03 outturn 40 Figures are 02/03 outturn Development Grant Education Authority Children’s Fund Total Child Psychotherapy Cornerstones 42nd St ADD / ADHD Centre Packages Inclusion and Access Division Projects specifically targeting mental health Educational Psychology, Education Inclusion, SEN, Educational Welfare Circle Time Training Young Runaways Triple P Child Witness Support Pyramid Trust 10 15 12 12 6 470 This is a cautious estimate of the time these teams spend dealing with CAMHS issues 29 Figures are 2003/4 97 allocations 115 27 36 6 ACTIONS 6.1 Recent Progress A number of actions for Salford were identified in the 1998 Salford and Trafford CAMHS Strategy, this section outlines recent progress against these actions: Action Progress 6.1.1. Ensure that the development of a Preventative Strategy for Children & Young People in Salford, and the roll-out of the Children’s Fund takes full account of the CAMHS agenda, especially tiers one and two Continue to develop training for first and second tier staff A written prevention strategy is being developed taking account of CAMHS issues. Prevention Strategy / Children's Fund coordinator is member of CAMHS Strategy group. 6.1.2. Focus on the further development of services to meet the needs of vulnerable groups including children looked after and young offenders. The Local Authority will focus its increased grant on these areas including such steps as the development of STARLAC, Cornerstones, and 42nd Street to ensure a range of responsive and supportive services. STARLAC social worker post in post. Cornerstones worker in post. YOT has link worker from core CAMHS service. Multi-disciplinary support is being offered to EBD schools and pupil support units. 6.1.3. In addition, the Local Authority will review the needs of an increasing number of children and young people looked after who present very challenging behaviour and cannot be cared for in a group. This is leading to an increasing number of placements with one-to-one supervision. Tri-partite funding panel established to consider how best to meet the needs of children with extreme complex needs. 6.1.4. Contribute to ongoing consideration of meeting the educational needs of children with learning disability (including autism and ADHD) and strengthening multi-agency responses to their needs. The ADHD Centre is working with the LEA in this area. 6.1.5. Enhance the diversity of skills Child psychotherapist in post. and therapies available, such as increasing the availability of child psychotherapy and play therapy 6.1.6. Establish CAMHS After Adoption support Will be taken forward using Adoption Support grant 6.1.7. Support voluntary organisations and partnerships which are contributing to service delivery and support especially for young people with emotional difficulties.(e.g. 42nd Street, Cornerstones, local ADHD Support Group) Links to Asylum Seeker team and Education services noted. Several voluntary sector providers are supported through links with core CAMHS services and the Strategy Group 6.1.8. Put in place steps to ensure that the development of services is based on evaluation of existing services. (Although some services are evaluated with inclusion of those using services in many areas of need and provision we are not currently able to identify outcomes for CAMHS provision. We have some good examples of individual project evaluation following on from the provision of training but have not yet created a single process for all CAMHS services. We will aim to use an evaluation group with user involvement in the future. 6.2 Actions to be Undertaken The actions the CAMHS Strategy group have identified as needing to be undertaken are listed below. A CAMHS co-ordinator is to be appointed by the PCT and Social Services to facilitate moving forward these actions. 6.2.1. 6.2.2. 6.2.3. Action detail Multi-agency commissioning arrangements terms of reference / membership of CAMHS strategy group to be reviewed possibility of a practitioners communications sub-group to be considered CAMHS co-ordinator to be appointed Information systems Tiers 2 / 3 IT systems to be developed Tiers 2 / 3 developments to link with Salford IRT work Clarify funding arrangements for CAMHS budgets Tiers 2 / 3 / 4 funding to be clarified to inform CMMCUHT / Salford PFI developments Future of joint finance budgets to be clarified Plans for investment of extra allocations to be firmed up 6.2.4. 6.2.5. 6.2.6. 6.2.7. 6.2.8. 6.2.9. 6.2.10. 6.2.11. 6.2.12. 6.2.13. 6.2.14. Develop user involvement role within commissioning cycle Element of extra allocation to be delegated to young people Young people to be involved in service performance management / quality monitoring Ensure Tri-Partite Funding Protocol (and other out of area placements) inform commissioning cycle Apparent gaps in service provision which lead to out of area placements to be clearly articulated Needs of children and young people with complex mental health problems to be articulated Multi agency service model to be developed Child protection CAMHS input into Salford child protection arrangements to be agreed Supporting Tier 1 service Tiers 2 / 3 support to be developed as other services develop (e.g. substance misuse service, ADHD service, LD service, etc.) Transition Scope of Tier 2/3 services to be reconsidered alongside national guidance Transition protocol to be agreed and implemented between CAMHS and Adult Mental Health services Clear pathways Articulate clear pathways through Salford services for ‘at risk’ groups Develop Family Action Model Access Ease access to CAMHS services for children and young people in PRUs Workforce Benchmark Salford CAMHS service workforce profile against national models to understand potential gaps Agree CAMHS service models with wider workforce especially considering role of speech therapists Pendleton Centre Design to be agreed Work to be underpinned by future service model for Tier 2 / 3 CAMHS service Special consideration to be given to service model underpinning the Day Unit Opportunities for Tier 4 to be maximised CMMCUHT and BSTMHP capital plans to be considered together Current hospital school service to be re-provided Role of school currently in providing services for children for whom no other local education service is suitable to be considered Plans to be developed to meet the need 6.2.15. 6.2.16. 6.2.17. 6.2.18. 6.2.19. 6.2.20. Future inpatient ward provision Service model for CAMHS provision to paediatric inpatient services at Hope Hospital to be agreed Learning Disability Service Develop integrated learning disability service, monitor and agree future development plans across agencies ASD Agree need / service model for services, link to LD service developments ADD / ADHD Agree need / service model for integrated service with voluntary sector and education Parenting Implement Triple P project and consider wider lessons for Salford Early Intervention in Psychosis Develop Salford services in line with regional and national guidance The table overleaf indicates how the above actions relate to the key themes coming out of local and national strategic vision. Theme Action Multi agency commissioning arrangements Information systems Budget clarification User involvement Tri-partite funding protocol Child protection Supporting Tier 1 Transition Pathways Access Workforce Pendleton centre design Tier 4 Opportunities Hospital School Service Inpatient ward provision Learning Disability Service ADD / ADHD ASD Parenting Early Intervention in Psychosis * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * *