SPM 200 Clinical Skills Lab 3 IV’s Daryl P. Lofaso, M.Ed, RRT
advertisement

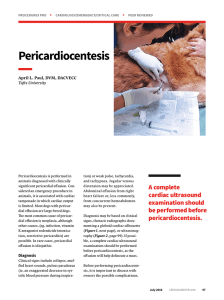
SPM 200 Clinical Skills Lab 3 IV’s Daryl P. Lofaso, M.Ed, RRT Indications for IV Indications: Intravenous access to patient’s circulatory system. Administration of Meds. & Fluids, as well as blood collection Contraindications: IV access should be attempted as distal as possible. Avoid veins that cross over joints, local infection/injury Extremities with renal shunts or fistulas Common IV sites IV catheter Size Age < 1 year: 22, 24 gauge (g) 1-8 years: 18, 20, 22 gauges > 8 years: 16. 18, 20 gauges IV Procedure Use universal precautions (glove and eye protection) Allergies (betadine or latex) Explain procedure to Pt. Prepare all material Select vein. Apply tourniquet above the elbow. Prepare site IV Procedure (cont.) Warn the pt of possible pain Bevel up at 30 degree above horizontal Look for flashback of blood into catheter Upon seeing flashback, advance catheter another millimeter or two Advance the sheath completely into the vein and release tourniquet IV Procedure (cont.) Connect the IV tubing/heplock Secure catheter and tubing Dispose of needles in sharps container Document the IV site, catheter size and date on the patient’s chart Risks to YOU Risks after needle Sticks Exposure Hepatitis B: 6 - 30% Hepatitis C: HIV: 3 - 10% 0.3 % Other blood borne pathogens Steps to prevent needle sticks Wear gloves Do Not Bend or Break Needles Never RECAP!!! If you must, use the One Handed technique Take your time Dispose of contaminated needles immediately in puncture-resistant containers ACCIDENTAL NEEDLE STICKS Immediately wash injured area. Report all needle sticks immediately to your instructor or immediate supervisor. Complete an incident report and report to employee health or ED. Determine if the needle was clean or dirty. Cleansing wound with antiseptic. Request that the identified patient be tested for Hepatitis B surface antigen and HIV antibodies. Have your blood tested for Hepatitis B and HIV antibodies as soon as possible. Begin drug treatment (if necessary) & counseling. How to calculate patient’s fluid rate Maintenance Fluid: Adult or Peds Fluid Disturbances Isotonic Imbalances Fluid volume deficit Losses from GI Loss of plasma or whole blood Fever Diuretics Fluid volume excess CHF Renal Failure Cirrhosis of liver Fluid Disturbances Osmolar Imbalances Hyperosmolar imbalance Diabetic ketoacidosis Osmotic diuresis Hypoosmolar imbalance SIADH Excess water intake (cont.) Electrolyte Imbalances Hyponatrema Hypernatrema Hypokalemia Hypocalcemia Hypercalcemia Hypomagnesemia Hypermagnesemia Risk Factors for Fluid, Electrolyte, and Acid-Base Imbalances Age Chronic disease Crush or head injuries or burns Therapies CA or Cardiovascular disease (CHF) Trauma Very old or very young Diuretics, steroids, IV therapy, TPN Gastrointestinal losses Gastroenteritis, NG Suction or fistulas