Treatment of Idiopathic Membranous Nephropathy
advertisement

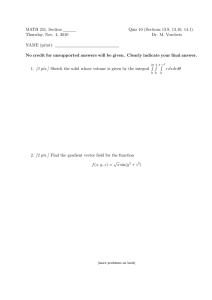
Treatment of Idiopathic Membranous Nephropathy Alexander Usorov, MD 4/21/09 Idiopathic MN Leading cause of Nephrotic syndrome in white adults Incidence rate has remained constant over 3 decades • As opposed to IgA Nephropathy and FSGS 2ry MN accounts for up to 1/3rd cases and a/w autoimmune dz (SLE, Hep B/C, NSAIDs, neoplasms) Both IMN and 2ry MN have similar clinical presentations • Therefore, r/o 2ry causes first Clinical Manifestations All ages (but rare in children) All races M>F 2:1 Peak incidence during 4th and 5th decade of life NS in 60-70% of pts at the time of presentation As per Dr. Cattran, about 60% of pts who present with subnephrotic-range proteinuria will progress to full NS within 1-2 years from presentation Microscopic hematuria in 30-40% Mostly normotensive pts (10-20 % with HTN) <20% of pts have significant renal insufficiency Natural History MN is a chronic dz with spontaneous remission and relapses The rule of 1/3rd: • • Spontaneous remission within the first 2 years after presentation Lower rates of spontaneous remission if pts present with higher degree of proteinuria (ie 8g/24hr) 2nd leading cause of ESRD among 1ry GNs Increased risk of thromboembolic and CV events Acute changes in proteinuria or rate of loss of renal fxn should raise the possibility of a superimposed event (RVT, crescentic GN, anti-GBM disease) Figure 1. (A and B) Light microscopy showing segmental sclerosis (arrow; A, periodic acid Schiff stain) and pinholes (arrow) along the glomerular basement membranes (B, silver stain) Fervenza, F. C. et al. Clin J Am Soc Nephrol 2008;3:905-919 Copyright ©2008 American Society of Nephrology (C and D) Immunofluorescence microscopy showing granular IgG (C) and C3 (D) along the capillary walls. (E) Electron microscopy showing subepithelial electron-dense deposits and basement membrane spikes (arrows) separating the deposits “Idiopathic” MN ? Ronco et al reviewed the rat model of Heymann nephritis and the role of alloimmunization as a new mechanism of MN in Seminars of Immunopathology 2007 Hypothesized that antibodies to neutral endopeptidases, aminopeptidase A, and dipeptidyl peptidase IV or DPPIV (all expressed in podocytes) are responsible for “Idiopathic” MN Salant’s presentation at ASN expanded on that idea • Could not find more info on this presentation Prognostic Factors Critical point When and what to use (conservative txt vs immunosuppressive txt) Allows to separate pts with good long-term renal survival from those who are likely to progress No specific markers available Current evidence does not support pathology as a helpful measure outside of making a diagnosis • • Not helpful in establishing prognosis Not helpful in prediciting response to immunosuppression Some evidence that urinary excretion ratios of a1microglubulin, b2-micro, IgM, IgG are helpful, but these tests are not routinely available Prognostic Factors Cont. Currently, the best model for ID of pts at risk was developed from Toronto Glomerulonephritis Registry Initial CrCl, the slope of CrCl, lowest level of proteinuria during a 6-mo observation period Has been validated in Italy and Finland Prognostic Factors Cont. Low risk for progression • • • Normal CrCl Proteinuria <4g/24hr Stable renal fxn during an observation period Medium risk (55% probability of developing CRI) • • • Normal CrCl Proteinuria >4g/24 hr but < 8g/24 hr Stable renal fxn during an observation period High risk (66-80% probability of progression to Chronic Renal Failure) • Persistent proteinuria >8g/24 hr independent of the degree of renal dysfxn Prognostic Factors Cont. Pts who were never nephrotic or who achieved CR (proteinuria < 0.3g/24hr with nl renal fxn) have an excellent long-term renal survival Troyanov, Cattran et al in KI 2004 found that in 350 MN pts with NS: • • 10-year renal survival was 100% in CR, 90% in PR (>50% reduction in proteinuria, >0.3g/24hr and <3.5g/24 hr), and 45% in no remission Loss of GFR: -1.5 ml/min/year in CR, -2 in PR, -10 in no remission Treatment Options Conservative (nonimmunosuppressive) Therapy Immunosuppressive therapy Conservative Therapy Restrict dietary protein intake (0.8g/kg ideal body weight per day, high quality protein) Low salt diet Target BP <125/75 mm Hg Control dyslipidemia with statins ACEI/ARB (weak evidence, largely inferential) Immunosuppressive Therapy Not used in low-risk group as side effects are likely to exceed the benefits Medium risk group first Steroids – monotherapy, no benefit Combined with cytotoxic agents: Ponticelli et al NEJM 1989 showed that 6-mo MTP IV + oral steroids alternating monthly with chlorambucil was superior to conservative txt in achieving CR (50% vs 7%) and PR (31% vs 24%) 10-year follow up showed that 8% of txt pts vs 40% of untxt pts reached ESRD Similar data with same cyclic steroid combo when chlorambucil was c/w cyclic steroids and oral cyclophosphamide. (Ponticelli et al JASN 1998) CR or PR in 82% vs 93% (P=0.116) Txt with CYC was a/w fewer side effects, but renal fxn was equally preserved for up to 3 years Recent trial by Jha et al JASN 2007 looked at 47 pts on 6-mo course of alternating prednisolone and CYC vs 49 pts with supporting txt: • • In txt group, 34 (15 CR + 19 PR) vs 16 (5 CR + 11 PR) 10-yr HD-free survival was 89% vs 65% with similar incidence of infections in both groups Long Term Adverse Effects for CYC Fertility Bladder carcinoma Myelodysplasia Risk of malignancy is not increased with cumulative CYC doses < 36 g, but increases significantly in pts with CYC doses > 36 g (Faurschou et al J. Rheumatology 2008) Cyclosporine Single RCT of 51 pts with MN Low-dose prednisone + CsA vs prednisone + placebo 26 weeks of txt 21/28 pts (78%) in CsA group vs 5/23 (22%) in placebo achieved PR or CR Relapse rate of 40% within 1 year of d/c of therapy • should not be considered failure of therapy as reintroduction of CsA or an alternative regimen can induce a remission Majority of CR occurs after > 6 mo of txt • If after 3-4 mo of CsA proteinuria is not significantly reduced, it is unlikely that CsA will be effective Prolonged low-dose CsA (1.5 mg/kg) has been suggested for long-term maintenance, with little risk for nephrotoxicity Tacrolimus Praga et al KI 2007 administered TAC monotherapy to 25 pts with nl renal fxn and mean proteinuria of 8 g/24 hr for 12 mo with a 6 mo taper vs 23 control pts. At 18 mo, the probability of remission was 94% in TAC group vs 35% in controls 2ry endpoint of 50% increase in SCr was reached by 6 control pts and 1 TAC pt Relapse rate of about 50% after withdrawal ? Low-dose maintenance long term High Risk for Progression Steroids – no benefit Combined with cytotoxic agents - no RCT available CsA – 1 RCT showing some benefit in 17 pts after 12 mo of txt (reduction in proteinuria and slope of renal fxn was reduced from -2.4 ml/min to -0.7 vs -2.2 to -2.1 in control group) with sustained results in 50% for 2 years after d/c of CsA MMF – possible benefit from 3g/day dosing New Therapies ACTH 2 studies by Berg (1 in pts with NS in 2004, and 1 in pts with MN in 1999) and a pilot study by Ponticelli et al AJKD 2006 16 pts were txt with MTP plus chlorambucil or CYC (group A) 16 pts were txt with ACTH 2 injections per week for 1 year (group B) Group A – 5 CR and 10 PR Group B – 10 CR and 4 PR Side effects a/w ACTH – dizziness, glucose intolerance, diarrhea, bronze-colored skin, which resolved after the end of therapy Rituximab Experimental data suggests that B-cell activation leads to IgG4 deposition along the GBM, which leads to injury to the membrane and thus proteinuria How about we selectively target B cells and halt the progression of these “autoantibodies”? Not a first line therapy Rituximab Cont A systematic review by Bomback et al in this month’s CJASN 21 studies were included in the final review • • 12 were single case reports 9 were case series ranging from 2 to 50 pts Both 1ry and 2ry MN pts were included Principally used as a 2nd line therapy except for one study Rituximab Cont Response rate was as follows CR 15-20% PR 35-40% Similar to RR for alkylating agents (CYC and chlorambucil) and CNIs (CsA and TAC) No direct comparisons to older therapy We need a well-designed RCT comparing rituximab to standard therapy such as Ponticelli’s regimen Rituximab – Future Questions Should rituximab be used as a first line therapy? • No data Optimal dosing regimen • • • Lymphoma protocol used for IMN by Remuzzi (375 mg/m2 weekly x4) Alternative progocol used by Fervenza’s (1 g on days 1 and 15) Titrating rituximab to circulating B cells used by Cravedi (1 st dose at 375 mg/m2, 2nd dose was given only if > 5 circulating B cells/mm3 were detected 1 week after txt) Long term risks and benefits? • • • No long-term data for rituximab in MN is available Recent reports of PML in MS pts Possible removal of pathogenic auto-Abs (kidneys from Heymann nephritis rats were transplanted into non-diseased rats and resolution of subepithelial deposits was seen)