Mites of Medical Importance
advertisement

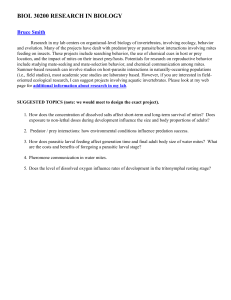
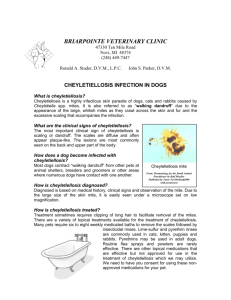
MITES Of Medical Importance MITES (Acari) • Free-living • Predacious • Parasitic (endo/ecto) • How can they be distinguished from ticks? Effects on Humans • Dermatitis or other tissue damage. • Loss of blood or other tissue fluids. • Transfer of pathogenic agents. • Strong allergic reactions ($10 billion each yr.) • Livestock: skin damage as much as $45 million worth each year. General Life Cycle • Egg • Prelarva • Hexopod larvae – May or may not feed. • Nymph – May or may not feed. – Protonymph, Deutonymph, Tritonymph • Adult – May take one or several meals. Acariasis • Infestation with mites (or ticks) • Some possible sites of infestation: – Respiratory passages and lungs. – External, inner and middle ear – Nasal passages – On and in the skin Sarcoptidae “Scabies Mites” • Sarcoptes scabiei • Also called the “itch mite” of humans • It causes the “Seven Year Itch” or “Norwegian Itch” • Not Vectors of any disease. Distribution • Worldwide • All races and socioeconomic classes • All climates • 300 million cases annually! Behavior • Burrowing initially occurs in thinner skin of the body. – Bend of knee and elbow. – Webbing between fingers and folds of the wrist. – Genitalia and buttocks. – Breasts. – Bony projects (Norwegian scabies). Life Cycle Transmission • Spread by ovigerous female mites through: – Personal (prolonged close) contact – Occasionally by infested sheets (rare). – Touching or shaking hands (unlikely). – Sexual activity. – Among children (outbreaks). – Mites can survive up to 24 hours off host. Recognition of Scabies • Females narrow twisting tunnels. • Feces in tunnels may be visible through skin. • Severe itching (reaction to proteins) • Genital lesions. • Large rashes on body. • Sores on body from scratching. • Patients often dirty. Scabies Rash Rash Continued • First time: 4-6 weeks incubation. • Second time: 2-4 days (reinfection). • Development of severe pruritus – Scratching at night, after hot baths. • Secondary infection – Boils – Pustules • Crusted Scabies: highly contagious (rare) Diagnosis • Scraping of skin • Ink on skin • Put on tetracycline • Infestation – Most 1-15 adults – Avg. 11 adults – 3% have more than 50 – More than 1000! (Norwegian). Treatment • Lindane lotion for 12 hours. – Don’t shower first! – Shower first, treat later (Norwegian) • Sulphur Preparations (Mitigal) – 1 treatment 100% effective, but mild dermatitis. • Modern acaracide (insecticides) – 5% permethrin cream (Elimite, Lyclear) – 1% aqueous malathion. – 1% Kwell lotion Trombiculidae “Scrub Typhus and Chigger Mites” • Around 3000 spp. Worldwide. • 20 spp. Medically important (attack people). • We will discuss 3 of the species. Chigger Mites “Harvest Mites or Red Bugs” • (1) Trombicula alfreddugesi • Distribution – Continental U.S. from New England to California (not north of Nebraska) – Second growth cutover areas – Moist microenv. Within grassy, weedy or wooded areas, especially wild berry patches. • Seasonality – Active May-September US distribution of chiggers - other areas also have focally high populations The Culprit Larval chigger mite Life Cycle • Egg Larvae (parasitic stage) 2 nymph stages Adult. • Require humidity and a vertebrate host for larval stage. • Tissue feeders. • Digestive juices secreted into host – Reaction around chigger – Non-burrowing Medical Importance • Stay on host a couple of days. • Itching occurs 3-6 hours after exposure. • More of a nuisance due to intense irritation. • Treatment: – Bathing – Antiseptic Chigger Mites “Harvest Mites or Red Bugs” • (2) Trombicula splenden • Distribution – Same story as T. alfreddugesi, but has a more southern distribution. • Seasonality – Active May-September for sure, but most likely is active longer or all year round. Chigger Protection • Stay out of areas where chiggers are likely to be present including woodlots, pastures, roadside ditches or other areas with tall grasses and weeds. Chiggers are especially common in moist low-lying areas. • Wear loose-fitting clothing and avoid sitting or reclining on the ground when camping, picnicking or working outdoors. • Apply a repellent containing DEET (N,N-diethyl-metatoluamide) to shoes, socks and trousers before entering chigger-infested areas. Chigger Protection • Immediately after possible exposure to chiggers take a bath, thoroughly scrubbing the body with hot soapy water. This will kill or dislodge many of the chiggers. • When bites begin to itch, apply rubbing alcohol, followed by one of the non-prescription local anesthetics. A baking soda paste, calamine lotion or product such as "After-Bite" also will help reduce discomfort. • Avoid scratching bites since this only increases irritation and may lead to secondary infection of the bite. • Where chiggers are a problem in landscapes, keep lawns and shrubbery well manicured especially in areas adjacent to dwellings. Eliminate tall grasses and weeds. Chiggers also can be reduced by spraying infested foliage with carbaryl (Sevin), chlorpyrifos (Dursban) or diazinon. Scrub Typhus “Japanese River Fever” • Vector species: – Leptotrombidium deliense – L. akamushi (Japan) – L. fletcheri (Malaysia) • Pathogen: – Orientia tsutsugamushi (rickettsia) Scrub Typhus Reservoir – mites Zoonotic: humans are accidental hosts Transovarial transmission (also co-feeding transmission). Distribution – Japan, SE Asia and islands of Indian Ocean and SW Pacific, coastal North Queensland, Australia History: WWII (1939-45) incidence in troops in the AsiaPacific area was second only to malaria. Epidemiology • People infected folling bite of larval mite. – Visiting or working in mite islands. • Associated with fringe habitats – Habitats separating two major vegetation zones – Areas often heavily populated with rodent host. • Risk of transmission often related to habitat diversity. – Number of areas of different types of vegetation. Life Cycle Signs and Treatment • Abrupt onset of high fever (104-105°F), severe headache, myalgia, and eschar with tender regional lymphadenopathy. • Approximately 35% of patients develop a centrifugal macular rash on the trunk. • A small number of patients have CNS involvement, with tremors, nervousness, slurred speech, nuchal rigidity, or deafness during, the second week of the disease. • Treat with antibiotics such as Tetracycline, Doxycycline, Chloramphenicol. (14 days) Control/Prevention • Repellents: – DEET, dibutyl phthalate, dimethyl carbamate or benzyl benzoate. • Insecticides • Protective clothing – Permethrin on clothes. • Mechanical control Miscellaneous Mites • (1) Ornithonyssus bacoti (Tropical rat mite). • (2) Ornithonyssus sylviarum (Northern fowl mite). • (3) Dermanyssus gallinae (Chicken mite). • (4) Liponyssoides sanguineus (House mouse mite). • (5) Pyemotes tritci (Straw itch mite). • (6) Tyrophagus putrescentiae (Grocers itch mite). • (7) Cheyletiella spp. (Cheyletiellid mites) Demodicidae “Follicle Mites” • Tenth to a fourth of a mm long. • 2 species: – Demodex folliculorum – Demodex brevis Dermatitis • • • • • • Very common Usually on skin of face, especially the eyelash and nose. 20% of individuals age 10-20 years is infested. 100% of the aged have them. In most cases they seem to be beneficial to us. Saprophytic mites are benign except when they invade the dermis, causing dermatitis. – Acne – Eyelashes fall out – Invade living tissue (rare). Pyroglyphidae “House-Dust Mites” • 2 species we are concerned with: Dermatophagoides pteronyssinos (European House Dust Mite) Dermatophagoides farinae (American House Dust Mite) Biology • Dust: – Prefer mattress dust – Find in dust samples – Find in furniture and carpets • More abundant in older homes • Humidity: – 75% relative humidity is optimum. – 40-50% relative humidity is minimal. • Not common in more arid parts of the country. Biology Continued • Females lay 1-3 eggs/day. • Eggs hatch after 6-12 days. • Egg Larvae Nymph (2 instars) Adult. • Life cycle takes 3-4 weeks • Adults live for 1-2 months. • Typically 300 mites per/gram of house dust. – Under ideal conditions (5000 mites/gram dust) – Record (15,600 mites/gram dust) – Above 100 mites/gram dust is considered a risk. Allergies • The exoskeleton and body parts have a common antigen. • People who are allergic to dust are also allergic to mites. • Have been linked to respiratory disease such as asthma. • Treatment/Control – Severe allergy: can receive a series of injections (desensitizing vaccine) – Enclose mattress and pillows with plastic – Wash bedding above temp 55C or dry-cleaning – Leave electric blanket switched on max for 6 hours or more during the day. Interesting Facts • House dust mites cause 25% of all allergies and 50% of all asthmatic diseases are traceable to house dust mites. Areas at highest risk for dust mite problems.