Cardiovasc. Res. 66 213-221 (2005).doc
advertisement
.doc")
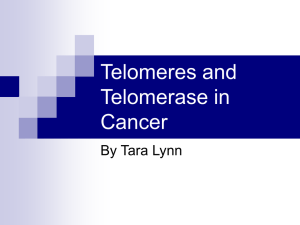
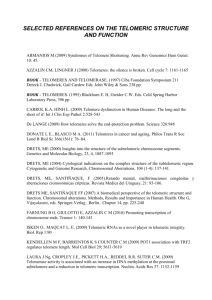
1 Aging, Telomeres and Atherosclerosis María Dolores Edo and Vicente Andrés1 Laboratory of Vascular Biology, Department of Molecular and Cellular Pathology and Therapy, Instituto de Biomedicina de Valencia-CSIC, 46010 Valencia, Spain KEY WORDS: Aging, telomeres, telomerase, atherosclerosis, hypertension, diabetes WORD COUNT: 8123 1 Corresponding autor: Laboratory of Vascular Biology Department of Molecular and Cellular Pathology and Therapy Instituto de Biomedicina de Valencia C/Jaime Roig 11, 46010 Valencia (Spain) Tel: +34-96-3391752 FAX: +34-96-3391751 E-mail: vandres@ibv.csic.es 2 SUMMARY Although the level and pace of population aging display high geographical variability, virtually all countries have been experiencing growth in their elderly population, particularly in developed nations. The US Census Bureau has estimated that aged population will rise steeply during the next decades. Because the morbidity and mortality associated with cardiovascular disease is so profound within the elderly, understanding the physiologic and molecular aspects of vascular aging is of up most importance. Mounting evidence suggests that the gradual shortening of telomeres during ageing is an important factor in the pathogenesis of atherosclerosis and associated disease. Here we review our current knowledge on the molecular mechanisms controlling telomere length in vascular cells, the importance of telomeres in vascular pathobiology as learnt from both human and animal studies, and potential applications of these findings to improve therapeutic angiogenesis. 3 1. Introduction Aging is a major risk factor for atherosclerosis and associated disease. [1,2] Population aging is decidedly increasing, particularly in developed countries. For example, data from the US Census Bureau estimate that the population over the age of 65 years will represent 20% in US and 25% in Europe. [3] Thus, a major challenge is to unravel the molecular mechanisms contributing to ageing to help implement novel preventive strategies and therapeutic approaches to reduce the impact of cardiovascular disease within the elderly. Because atherosclerosis is the most frequent cause of myocardial infarction (MI) and stroke, this review will focus on age-dependent structural and functional alterations of the vessel wall, and on the interrelationships between telomeres and atherosclerosis. Telomere alterations in hypertensive and diabetic patients will be also discussed, as these individuals are at higher risk of cardiovascular disease. During the last decades, human and animal studies have identified cardiovascular risk factors and molecular networks that control atheroma progression, including both adaptive and innate immune mechanisms. [1,2,4-7] Endothelial dysfunction induced by a variety of atherogenic stimuli (i. e., hyperlipemia, hypertension, diabetes, cigarette smoking) is at the onset of atherosclerosis at sites of predisposition to atheroma formation. Adhesion of circulating leukocytes to the damaged endothelium leads to the formation of fatty streaks, an early form of atherosclerotic lesion enriched in highly proliferative macrophages that avidly uptake lipoproteins to become lipid-laden foam cells. Activated intimal immune cells abundantly secrete inflammatory mediators that promote the proliferation and migration of the underlying medial smooth muscle cells (SMCs), thus further contributing to atheroma progression. [1,2,8,9] Rupture or erosion of advanced atherosclerotic lesions can lead to thrombus formation and myocardial infarction (MI) or stroke. Whether pathological alterations in the aged vessel wall result from the cumulative damage imposed by atherogenic stimuli, a consequence of age-dependent intrinsic vascular alterations, or a combination of both remains controversial. Old rabbits fed a low-dose hypercholesterolemic diet 4 (0.25% cholesterol) for 2 and 18 months developed more atherosclerosis than did young counterparts. [10,11] However, old rabbits exposed for 2 months to 1% cholesterol feeding displayed reduced aortic atherosclerosis compared with juvenile counterparts. [12] Of note in this regard, young and old rabbits receiving for 2 months the 1% cholesterol diet averaged plasma cholesterol levels of 1747-2488 mg/dL, [12] while animals challenged for the same period of time with 0.25% cholesterol diet averaged 148-178 mg/dL. [11] Thus, age-dependent intrinsic alterations in the vessel wall appear to increase the susceptibility to atherosclerosis in aged rabbits subjected to a mildly atherogenic stimulus. In contrast, the predisposition to atherosclerosis upon extreme dietary hypercholesterolemia is significantly higher in young rabbits. It has been recently shown that despite showing similar alterations in lipid profile, senescence-accelerated prone mice (SAM-P), which age at an accelerated rate, are more susceptible to early diet-induced atherosclerosis than senescence-accelerated resistant mice (SAM-R), which age normally. [13] Because mice in this study were fed for 17 weeks a Western-type diet containing only 0.15% cholesterol, it would very informative to investigate the atherogenic response of SAM-P and SAMR mice under a highly atherogenic dietary regime (i. e., 1% cholesterol). Rauscher et al. found that, compared with BM-derived progenitor cells from young atherosclerosis-free apolipoprotein E (apoE)-null mice, cells obtained from old atherosclerotic counterparts were much less effective at preventing atherosclerosis when transplanted into apoE recipients. [14] The authors suggested that age-dependent progenitor cell deficits, by impairing arterial cell repair and rejuvenation, may contribute to the development of atherosclerosis. Likewise, it has been suggested that aging exacerbates negative remodeling and impairs endothelial regeneration after balloon injury. [15] 5 2. Structural and functional vascular alterations during ageing A sustained effort has been taken in the Baltimore Longitudinal Study on Ageing (BLSA) in order to characterize the effects of ageing on multiple aspects of cardiovascular structure and function in a single population. [16] Relevant conclusions from this, as well other studies in humans and animal models, will be summarized below. Age-associated changes of the artery wall, such as luminal dilation, intimal and medial thickening (wall thickening), vascular stiffness and endothelial dysfunction, are quite similar in humans, rodents and nonhuman primates. [17,18] 1.1. Wall thickening. Wall thickening and dilatation are prominent structural features of aged large elastic arteries. [19] Postmortem studies have shown that age-dependent aortic wall thickening consists mainly of intimal thickening, [20] and non invasive measurements in BLSA individuals showed a thickness increment of 2-to-3-fold between 20 and 90 years of age. Arterial wall thickening occurs in both aged atherosclerotic and atherosclerosis-free arteries in humans and experimental animal, suggesting that arterial thickening is an intrinsic age-associated process independent of atherosclerosis that may predispose to future risk of cardiovascular disease. [20,21] Cellular, enzymatic and molecular mechanisms underlying progressive intimal and medial thickening have been studied largely in rodents. The thickened intima in old rats is enriched in matrix molecules (i. e. collagen, fibronectin and proteoglycans) and SMCs. In addition, the aged intima exhibits increased immunostaining for transforming growth factor beta (TGF-), interstitial cell adhesion molecule (ICAM-1), the zinc-dependent endopeptidase type-2 metalloproteinase (MMP-2) and its activator, membrane type metalloproteinase-1. Remarkably, the results of tissue culture and rat carotid balloon angioplasty studies suggest that chemotactic invasion of SMCs to the intimal layer through the basement membrane requires activated MMP-2 and type IV collagenase activity potentially derived from cytokine stimulated vascular SMC. [22,23] This reflects a chronically enhanced level of cytokine stimulation and an exaggerated chemotaxis and 6 proliferative response to growth factors, such as PDGF. [24,25] On the other hand, although the antiproliferative actions of TGF- decrease with age, [26] TGF- suppresses the activity of proteases and activates tissue inhibitors of MMPs as well as the synthesis of extracellular matrix proteins. Indeed, TGF- accumulation in the intima of older rats may be related to age-associated increase in arterial fibronectin and collagen. [18,27] Upregulation of angiotensin converting enzyme (ACE) activity has been observed in the aorta of old rats, and this correlates with increased level of angiotensin II. [28] Angiotensin II, in turn, is able to regulate TGF- and fibronectin expression. [29] 1.2. Wall stiffness. Age-associated increase in intima/media thickening is accompanied by both luminal dilatation and a reduction in compliance or distensibility, resulting in increased vessel stiffness. [21] Although age-associated increase in arterial stiffness has been observed in individuals with little or no atherosclerosis, [30] recent data emerging from epidemiological studies indicate that increased large vessel stiffening also occurs in the context of atherosclerosis and diabetes. [31,32] The total mucopolysaccharide content of the interstitial matrix is unaltered with aging, however aged arteries display increased chondroitin sulphate and heparin sulphate levels, and reduced hyaluronate and chondroitin content. [33] The distribution of unstretched collagen also changes with age, and it has been proposed that age-associated changes in collagen involve a decrease in the coiling and twisting of molecular chains and a reduction in effective chain length. [34] Regarding elastin fibrils, their glycoprotein component decreases and eventually disappears with aging. In aged rats, elastin becomes frayed, and its calcium content increases. The increased mineralization of elastin with aging is associated with an increase in the content of more polar amino acids. [19] 7 As the wall of large arteries become stiffer, central systolic arterial pressure raises, diastolic arterial pressure decreases, and the pulse pressure increases. These findings suggest that altered structure/function resulting from stiffness of the vessel wall is a risk factor for future vascular events, independently of the associated increase in systolic and pulse pressures. [21] In addition to structural properties, arterial stiffness in vivo is determined by vascular smooth muscle contractile tonus, which is controlled in part by neurohumoral factors (catecholamines, angiotensin, etc) and by the SMC calcium balance. [19] 1.3. Endothelial dysfunction. Aging enhances the expression of adhesion molecules in the rat aorta, [18] and increases monocyte adherence to the endothelium of the rabbit aorta. [35] Moreover, aged rodents show increased vascular permeability, [36] and the intima of older rabbits accumulates glycosaminoglycans, [35] which play an important role in regulating vascular permeability. In addition, aging elevates nitrite and nitrate levels in plasma, [37] and nitricoxidedependent endothelial vasodilatation is attenuated by reduction in nitric oxide in the aged aorta. [38,39] 3. Telomere biology Eukaryotic telomeres prevent the recognition of chromosomal ends as double stranded DNA breaks thus preserving genome integrity and stability. Telomeres are specialized DNA-protein complexes located at both ends of linear chromosomes. As depicted in Fig. 1A, telomeric DNA consists of non-coding double-stranded repeats of G-rich tandem sequences (TTAGGG in humans) that extend several thousand base pairs and end in a 3' single-stranded overhang. Conventional DNA polymerases are unable to synthesize telomeric DNA, an activity that requires specialized telomere-associated proteins (i. e., telomerase, TRAF1, TRAF2, Ku86, etc). The enzyme 8 telomerase has a catalytic telomerase reverse transcriptase (TERT) component and a telomerase RNA (Terc) that provides a template for new telomeric DNA synthesis. Telomere homeostasis depends on several factors, including the precise composition of telomere-associated proteins, the level of telomerase activity, and telomere length itself. [40,41] Cells with sufficiently long telomeres do not require telomerase activity, but lack of telomerase activity in cells with critically short telomeres leads to chromosomal fusions, replicative senescence, and apoptosis (Fig. 1B). Telomerase expression and activity and telomere length are tissue and developmentally regulated in several species, including humans. [42-45] In general, these parameters are greater during embryonic development and become low or undetectable after birth, although significant differences in adult tissues have been reported. For instance, human telomeres shorten at an estimated rate of 29-60 bp/year in liver, renal cortex and spleen, but telomere length is maintained in cerebral cortex. [46] Notably, human premature aging syndromes (i. e., Werner syndrome, ataxia telangectasia, dyskeratosis congenita) are characterized by an accelerated rate of telomere attrition (Figure 1B). Progressive telomere shortening in cell culture and during ageing of the whole organism is a characteristic of most adult somatic cells, which exhibit low or absent telomerase activity. [47-49] Of note in this regard, human TERT (hTERT) is alternatively spliced in specific patterns by different tissue types during development, and this mechanism often leads to the expression of hTERT protein lacking functional reverse transcriptase domains. [50] In contrast to adult somatic cells, the extended proliferative capacity of germ and tumor cells correlates with the maintenance of high telomerase activity and long telomeres. Indeed, ectopic TERT overexpression inhibits replicative senescence and extends the lifespan of numerous cell types, including SMCs and endothelial cells (ECs) (Table). By comparing the chronological changes in the expression of cell cycle and apoptosis-related genes in hTERT transduced human normal fibroblasts and ECs, Kumazaki et al. suggested that cell-type specific differential gene 9 expression after telomerase activation may be important to acquire telomere-maintenance capacity and immortality. [51] Telomere length displays individual differences in both rodents [44,45] and humans. [46,5254] Since Okuda et al found high variability of telomeric DNA length in white blood cells (WBCs), umbilical artery and skin from donor newborns independently of gender, they suggested that genetic and environmental determinants that start exerting their effect during embryonic development are key determinants of telomere length. [52] Further support to the notion that telomere size is familial has arisen from human studies in twins. [53,55] By measuring terminal restriction fragment (TRF) length in WBC DNA taken from individuals from a family-based cohort, Nawrot et al. concluded that inheritance of telomere length is linked to X chromosome. [56] 4. The importance of telomeres in vascular pathobiology In the next sections, we will discuss tissue culture, animal and human studies that highlight the importance of telomeres in vascular pathobiology, including recent insights into the mechanisms that alter telomere homeostasis in response to several stimuli with relevance in atherosclerosis (i. e., estrogens, oxidative stress, hypertension and diabetes) (Table and Fig. 1 and 2). The role of telomeres on cardiac pathobiology has been comprehensively discussed elsewhere. [57,58] 4.1. Telomeres and estrogens. Indirect effects on lipoprotein metabolism and direct actions on vascular ECs and SMCs are thought to contribute to the cardioprotective effects of estrogens in premenopausal women. [59-62] It is noteworthy that human and animal studies have shown higher telomerase activity and a decelerated rate of age-dependent telomere exhaustion resulting in greater telomere lengths in females than in males, [43,45,55,56,63,64] and these sex differences 10 might be directly related to estrogen-dependent activation of endothelial telomerase via phosphoinositol 3-kinase (PI3K)/Akt and nitric oxide signaling. First, estrogen upregulates hTERT mRNA, and this correlates with direct and indirect effects on the hTERT promoter (specific binding of 17-estradiol to an imperfect palindromic estrogen-responsive element, and 17estradiol-dependent induction of c-Myc/Max binding to E-boxes, respectively). [65] Second, nitric oxide production may contribute to telomerase activation in vascular ECs. [66,67] Third, treatment of human ECs with estrogen activates the PI3K/Akt pathway, [66] which in turn leads to hTERT phosphorylation and activation. [68] In contrast, either overexpression of dominant negative Akt or PI3K inhibition attenuate telomerase activity in ECs, [69] and Akt inactivation by proatherogenic oxidized low density lipoproteins impairs telomerase activity in ECs. [69] Collectively, these studies suggest that a positive effect of PI3K/Akt on telomerase expression and activity may contribute to the maintenance of EC integrity and function. Contrary to this notion, Miyauchi et al. recently reported that constitutive activation of Akt promotes senescence-like arrest of human EC growth via a p53/p21-dependent pathway. [70] Additional studies are thus required to clarify the links between telomere function, PI3K/Aht signaling and EC pathobiology. 4.2. Telomeres and oxidative stress. Accumulation of oxidative damage is thought to play an important role in aging and associated diseases. [71] Mounting evidence implicating oxidative stress in telomere dysfunction include the following: 1) Chronic oxidative stress induces a rapid and sustained decrease in TERT activity and accelerates telomere attrition in human umbilical vein ECs (HUVECs); [72] 2) maximum levels of glutathione coincide with a peak of telomerase activity in proliferating 3T3 fibroblasts; moreover, glutathione depletion decreases by 60% telomerase activity, and restitution of glutathione levels restores telomerase activity; [73] 3) agedependent telomere shortening in HUVECs is slowed down by Asc2P, and oxidation-resistant derivative of vitamin C which reduced by 53% the level of proatherogenic reactive oxygen 11 intermediates; [74] 3) oxidized low density lipoproteins inhibit EC telomerase activity; [69] 4) oxidative stress induced in human ECs by exposure to H2O2 leads to translocation of both endogenous and overexpressed hTERT from the nucleus into the cytosol via Src kinase familydependent phosphorylation of hTERT tyrosine 707, which reduces the antiapoptotic capacity of TERT; [75] furthermore, reduction of intracellular reactive oxygen species formation by the antioxidant N-cetylcysteine prevented mitochondrial damage and delayed nuclear export of TERT protein, loss of TERT activity and the onset of replicative senescence; [76] and 5) formation of 8oxo-7,8-dhydro-2’-deoxyguanosine at the GGG triplet in the telomeric DNA sequence may be a mechanism facilitating telomere shortening induced by oxidative stress. [77] 4.3. Role of telomeres in vascular pathobiology: Evidence from human studies 4.3.1. Atherosclerosis. By inducing replicative senescence, age-dependent telomere erosion is likely to contribute to progressive endothelial dysfunction and atherosclerosis. Indeed, a characteristic senescent phenotype is observed in the endothelium of atherosclerotic lesions. [78] Of note, overexpression of a dominant-negative mutant of telomere repeat binding factor 2 (TRF2) induces senescence in human aortic EC cultures, and TERT transduction can prevent replicative senescence of these cells. [78] Both telomere shortening and increased frequency of aneuploidy is observed in ECs from the aged abdominal aorta. [79] Remarkably, endothelial telomere erosion occurs at a greater rate in the iliac arteries versus iliac veins (102 bp/yr vs. 47 bp/yr, respectively), and age-dependent intimal telomere attrition is greater in the iliac artery compared to the internal thoracic artery (147 bp/yr vs. 87 bp/yr, respectively), [80] a vessel subjected to a reduced amount of hemodynamic stress. Okuda et al. also reported increased age-dependent telomere ablation in both the intima and media of the distal versus proximal abdominal aorta, and found an inverse correlation between atherosclerotic grade and telomere length (although this relationship was not 12 statistically significant after adjustment for age). [81] Taken together, these studies suggest a higher rate of telomere shortening in aged vascular beds with increased shear wall stress and enhanced cellular turnover. Because leukocytes are key players during atherosclerosis, [1,2,6,7] several studies have compared telomere length in WBC from healthy controls and cardiovascular patients. Patients with vascular dementia, a disorder that is frequently associated with cerebrovascular atherosclerosis and stroke, have significantly shorter telomeres in WBCs compared with 3 age-matched control groups, namely cognitively competent patients suffering from cerebrovascular or cardiovascular disease alone, patients with probable Alzheimer's dementia, and apparently healthy control subjects. [82] After adjustment for age and sex, leukocyte average telomere length in 10 patients suffering severe coronary artery disease (CAD) was significantly reduced compared with 20 controls with normal coronary angiograms. [83] In a larger study including 180 controls and 203 cases of premature MI, age- and sex-adjusted mean TRF length of controls was significantly larger than that of patients, and subjects with shorter than average telomeres had between 2.8- and 3.2fold higher risk of MI. [84] Likewise, analysis of telomere length in blood DNA from 143 normal unrelated individuals over 60 years of age disclosed an association between shorter telomeres and poorer survival that was partly attributed to a 3.18-fold mortality rate from heart disease and a 8.54-fold higher mortality rate from infectious disease. [85] 4.3.2. Hypertension and diabetes. Hypertensive patients are more prone to atherosclerotic lesions and acute ischemic events that normotensive individuals. [5] Analysis of 49 twin pairs (38 males and 60 females within 18 and 44 years of age) revealed a positive correlation between WBC TRF and diastolic blood pressure. [55] Because TRF length and systolic blood pressure were inversely associated, telomere length seems to negative correlate with pulse pressure. Notably, the link between TRF length and pulse pressure was independent of gender and both parameters appeared 13 highly heritable. Benetos et al. also investigated WBC telomere length and blood pressure parameters that are associated with stiffness of large arteries (pulse pressure and pulse wave velocity) in individuals who were not under antihypertensive medications (120 men, 73 women, mean age of 56±11 years). [64] While telomere length negatively correlated with age in both sexes, multivariate analysis showed that telomere shortening significantly contributes to increased pulse pressure and pulse wave velocity only in men. In both studies, women showed age-adjusted longer telomeres, suggesting that biological aging is slowed down in women. More recently, Benetos et al. examined the relationship between WBC telomere length and carotid artery atherosclerosis in 163 treated hypertensive men who were volunteers for a free medical examination. [86] They found that telomere length was shorter in hypertensive men with carotid artery plaques versus hypertensive men without plaques (8.17+/-0.07 kb versus 8.46+/-0.07 kb; p<0.01), and multivariate analysis revealed that, in addition to age, telomere length significantly predicts the presence of carotid artery atherosclerosis. The prevalence of both microvascular and macrovascular disease is significantly increased in diabetic patients. [4] Telomere length in WBCs from insulin-dependent diabetes mellitus patients is reduced compared with age-matched nondiabetic subjects. [87] This parameter was similar in non insulin-dependent diabetes mellitus patients and nondiabetic controls, suggesting that telomere erosion only occurs in a subset of WBCs that play a role in the pathogenesis of insulin-dependent diabetes mellitus. Further support implicating telomere exhaustion as a mechanism contributing to coronary atherosclerosis under some circumstances of metabolic disorders arises from the observation that hypercholesterolemic and diabetic CAD patients display shorter telomeres in peripheral blood mononuclear cells than healthy controls. [88] 4.3.3. Neovascularization. Proliferation of vasa vasorum promotes atherosclerosis. [89] On the other hand, therapeutic neovascularization is essential for the restoration of blood flow into 14 ischemic territories in the adult organism, which depends on the development of new collateral vessels from established vascular networks (angiogenesis) and on de novo vessel formation by endothelial progenitor cells (vasculogenesis). [90] Using an experimental model of limb ischemia, Rivard et al demonstrated and impairment of angiogenesis in old versus young rabbits. [91] They also showed diminished expression of the angiogenic cytokine vascular endothelial growth factor (VEGF) with ageing, and old rabbits exposed to exogenous VEGF exhibited a similar increase in blood pressure ratio, angiographic score, and capillary density than did young counterparts. Thus, VEGF downregulation might be critical for age-dependent impairment of angiogenesis in response to ischemia, and this may result from reduced activity of the transcription factor hypoxia-inducible 1 (HIF-1). [92] Remarkably, whereas both angiogenic cytokines VEGF and fibroblast growth factor-2 (FGF-2) elicited a mitogenic response in cultured HUVECs, only FGF-2 induced the upregulation of hTERT mRNA and enzymatic activity and delayed the appearance of a senescent phenotype. [93,94] Because of these differences, it would be interesting to compare the angiogenic response elicited by exogenous FGF-2 and VEGF in old rabbits. Overexpression of hTERT in human dermal microvascular ECs (HDMECs) augments their capacity to form more durable microvascular structures when subcutaneously xenografted in severe combined immunodeficiency mice. [95] Similarly, hTERT gene transfer into human endothelial progenitor cells improves their proliferative and migratory activity, enhances survival, and augments neovascularization when applied in a murine hindlimb ischemia model. [96] Recruitment of SMCs and pericytes into new capillaries composed by a monolayer of ECs is important for their stabilization and maturation into fully functional vessels. Hypoxia is a major angiogenic stimulus that induces TERT protein expression and phosphorylation in cultured SMCs. [97] Telomerase inhibition shortened the life span of hypoxic cultures, and constitutive TERT expression extended life span under normoxia, suggesting that hypoxia-mediated telomerase 15 activation promotes long-term SMC growth. It remains to be established if chronic hypoxia can induce endothelial telomerase activity. The importance of telomerase in angiogenesis is further emphasized by the progressive induction of hTERT mRNA expression in human ECs of newly formed vessels within tumors. [98] Endothelial hTERT expression was observed in 29%, 56% and 100% of low-grade astrocytomas, anaplastic astrocytomas and advanced glioblastomas multiforme, respectively. While the proliferation rate and hTERT mRNA expression are dissociated in human ECs from low-grade and anaplastic astrocytomas, high proliferation rate and hTERT mRNA level positively correlated in glioblastomas multiforme. Remarkably, hTERT mRNA and protein expression and telomerase activity are induced in EC cultures exposed to diffusible factor(s) produced by glioblastoma cells. [99] 4.4. Role of telomeres in vascular pathobiology: Lessons learnt from animal studies Terc-deficient mice have been a valuable tool to investigate at the organismal level the role of telomere homeostasis. [100-107] In spite of Terc inactivation, the breeding of successive generations of Terc-null mice is needed to reach critically short telomeres leading to abnormal chromosome end-to-end fusions and symptoms of premature aging and disease, such as infertility, graying of hair, alopecia, impaired wound healing, small intestine and spleen atrophy, reduced proliferation of T and B lymphocytes, and hematopoietic disorders. Furthermore, late-generation Terc-null mice display reduced lifespan. We will review in the next sections studies in Terc-null mice and spontaneously hypertensive rats that link telomeres and vascular pathobiology (Fig. 2). 4.4.1. Atherosclerosis. Because age-dependent telomere shortening is more prominent in human arteries subjected to a higher atherogenic hemodynamic stress, and individuals with shorter telomere length in WBC present a higher prevalence of arterial lesions and higher risk of 16 cardiovascular disease mortality (see above), it is tempting to speculate that telomere exhaustion may be a primary abnormality that renders the organism more susceptible to cardiovascular risk factors. Alternatively, reduced telomere length in these scenarios may simply reflect augmented cell turnover induced by the chronic inflammatory response underlying atherosclerosis. Our recent studies using genetically-modified mice seem to support the latter. [107] We found that lategeneration mice doubly deficient for Terc and apoE (Terc/apoE-KO) have shorter telomeres and are protected from diet-induced atherosclerosis compared with atherosclerosis-prone apoE-null counterparts with an intact Terc gene. This beneficial effect of telomere exhaustion could not be attributed to reduced hypercholestrolemia, and was correlated with a significant inhibition in the proliferative capacity of lymphocytes and macrophages. It is worth recognizing the limitations of these animal models, therefore prospective epidemiological studies are warranted to assess whether WBC telomere length at birth can predict the risk of developing CAD in adulthood independently of known cardiovascular risk factors. Another important issue when interpreting the atheroprotective role of telomere exhaustion in hypercholesterolemic Terc/apoE-KO mice is that human ageing is associated with telomere erosion in most somatic cells, [48,49] yet atherosclerosis is more prevalent within the elderly. These seemingly conflicting findings might be reconciled accepting that accumulation of cellular damage imposed by prolonged exposure to cardiovascular risk factors may ultimately prevail over protective mechanisms such as telomere shortening. 4. 4.2. Neovascularization. Telomere exhaustion in late generation Terc-null mice leads to a sharp decrease in angiogenesis in both Matrigel implants and murine melanoma grafts, and diminished tumor cell proliferation, increased tumor cell apoptosis, and a lower tumor growth rate. [104] Given the data implicating neointimal angiogenesis as a mechanism contributing to atheroma growth, [89] it will be instructive to examine the effect of telomere shortening on neointimal vasa vasorum density. 17 4.4.3. Hypertension. In the aorta of spontaneously hypertensive rats, but not in other tissues, telomerase is activated before the onset of hypertension, and telomeres are lengthened both in vivo and in cultured SMCs from these animals. [108] Downregulation of telomerase by TERT antisense RNA delivery arrested the increased proliferation of spontaneously hypertensive rat vascular SMCs and induced apoptosis by a mechanism that can be reversed by p53 overexpression and worsened by lowering p53. The authors concluded that selective TERT activation and subsequent telomere lengthening in aortic medial SMCs is the driving force for the imbalance between cell proliferation and apoptosis that ultimately results in the vascular remodeling seen in genetic hypertension. Hamet et al. observed in the kidney of spontaneously hypertensive rats a transient hyperplasic response during the first 2 weeks of postnatal life that was absent in age-matched normotensive controls. [109] Because shorter telomeres are detected in the kidney of spontaneously hypertensive rats at all ages examined, the authors suggested that kidney cells from these animals are subjected to increased turnover, potentially leading to their accelerated aging. 5. Telomerase gene transfer for therapeutic revascularization By analizing the offspring obtained by mating heterozygous Terc+/- mice and late-generation Terc-null mice, which have short telomeres, unstable chromosomes and signs of premature aging, Samper et al. demonstrated that critically short telomeres can become fully functional by restoration of telomerase. [110] Because age-dependent telomere erosion may compromise the reestablishment of adequate blood supply into ischemic territories by limiting de novo vessel formation, telomerase gene transfer appears an attractive strategy to boost therapeutic neovascularization. It has been shown that ex vivo expanded human endothelial progenitor cells enhance therapeutic neovascularization in animals, [111] and in vivo transplantation of hTERTtransduced endothelial progenitors increased capillary density and limb salvage in a murine model 18 of hindlimb ischemia. [96] In contrast, although TERT overexpression in murine hematopoietic stem cells prevented telomere loss in these cells during serial transplantation, this strategy did not extend their transplantation capacity, [112] suggesting that telomere-independent barriers may limit the transplantation capacity of hematopoietic stem cells. McKee et al. have provided evidence that hTERT transduction may be an appropriate strategy for the production of tissue-engineered human arteries for bypass surgery. [113] Compared with control cells, passaged human aortic SMCs overexpressing hTERT maintained telomere length, disclosed extended lifespan, and retained a normal morphology and a differentiated, non-malignant phenotype at late-passage. Remarkably, engineered vessels containing HUVECs and hTERT-transduced SMCs showed improved cellular viability and were mechanically and architecturally and superior to vessels generated from non-transduced SMCs. 6. Concluding remarks Several mechanisms contribute to age-dependent telomere exhaustion, including low telomerase activity, an imbalance in the relative level of telomere-associated proteins, or a combination of these factors. By imposing replicative senescence, apoptosis, and chromosome abnormalities, telomere dysfunction is thought to contribute to aging and associated disorders, including cardiovascular disease. A high degree of individual variability is observed in telomere length, which seems to be controlled by both genetic and environmental factors. It is remarkable that telomere exhaustion is delayed in women compared to age-matched men, and this gender difference may be related to estrogen-dependent induction of telomerase activity. Thus, comparably longer telomeres by estrogen action may contribute to the lower incidence of cardiovascular disease in premenopausal women. Recent human studies have shown shorter telomeres in human arterial tissue from atherosclerosis-prone vascular beds and in WBCs from hypertensive, diabetic and CAD patients, 19 and this is associated with an increased risk of cardiovascular disease mortality. However, it remains to be established whether telomere erosion is cause or consequence of these disorders. Indeed, studies in genetically-modified mice demonstrate that telomere erosion protects against diet-induced atherosclerosis. Thus, prospective epidemiological studies are necessary to ascertain whether telomere shortening is an independent cardiovascular risk factor. Moreover, further basic research is needed to gain mechanistic insight into the role of telomerase and additional telomereassociated proteins in cardiovascular pathobiology and to apply this knowledge for therapeutic applications. 20 Acknowledgements We thank M. J. Andrés-Manzano for preparing the figures. Work in the laboratory of V.A. is supported in part by the Ministry of Education and Science of Spain and Fondo Europeo de Desarrollo Regional (grants SAF2001-2358, SAF2002-1443), and from Instituto de Salud Carlos III (Red de Centros C03/01). M.D.E. is the recipient of a predoctoral fellowship from Generalitat Valenciana (Spain). 21 Table 1: Cell culture studies implicating telomere length and telomerase in vascular pathobiology Cell Type Main Findings Hypoxia-induced telomerase activation in human SMCs correlates with increased cellular proliferation Smooth Telomerase activity correlates with proliferation of primary SMCs, muscle cell and its inhibition attenuates hyperplastic growth (SMC) Endothelial cell (EC) Refs. [97] [108,114] hTERT forced overexpression extends the lifespan of rat SMCs [113] Telomere attrition correlates with limited proliferative capacity of passaged human ECs [80,115] Telomerase ectopic overexpression or inhibition affect the lifespan of human aortic ECs [78,116] Constitutive hTERT expression enhances the regenerative capacity of endothelial progenitor cells [96] FGF-2, but not VEGF, upregulates telomerase activity and delays the onset of senescence in HUVECs [93,94] Estrogen activates the PI3K/Akt pathway in human ECs, and Akt activation upregulates human telomerase activity; in contrast, PI3K inhibition and dominant negative Akt mutant significantly reduce telomerase activity in EC cultures [66,68,69] Telomerase activity and nitric oxide production are induced by estrogen in vascular ECs [66,67] Oxidized low density lipoproteins diminish Akt and telomerase activity in ECs [69] Chronic oxidative stress compromises telomere integrity and accelerates the onset of senescence in human ECs [72] Antioxidants inhibit nuclear export of TERT and delay replicative senescence of human ECs [76] 22 REFERENCES [1]. Lusis AJ. Atherosclerosis. Nature 2000;407:233-241. [2]. Ross R. Atherosclerosis: an inflammatory disease. N Engl J Med 1999;340:115-126. [3]. Kinsella K, Velkoff VA. An aging world: 2001. US Census Bureau, Series P95/01-1 2001; http://www.census.gov/prod/2001pubs/p95-01-1.pdf. [4]. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. Jama 2002;287:2570-2581. [5]. MacMahon S, Peto R, Cutler J, et al. Blood pressure, stroke, and coronary heart disease. Part 1, Prolonged differences in blood pressure: prospective observational studies corrected for the regression dilution bias. Lancet 1990;335:765-774. [6]. Binder CJ, Chang MK, Shaw PX, et al. Innate and acquired immunity in atherogenesis. Nat Med 2002;8:1218-1226. [7]. Greaves DR, Channon KM. Inflammation and immune responses in atherosclerosis. Trends Immunol 2002;23:535-541. [8]. Rivard A, Andrés V. Vascular smooth muscle cell proliferation in the pathogenesis of atherosclerotic cardiovascular diseases. Histol Histopathol 2000;15:557-571. [9]. Dzau VJ, Braun-Dullaeus RC, Sedding DG. Vascular proliferation and atherosclerosis: new perspectives and therapeutic strategies. Nat Med 2002;8:12491256. [10]. Spagnoli LG, Orlandi A, Mauriello A, et al. Aging and atherosclerosis in the rabbit. 1. Distribution, prevalence and morphology of atherosclerotic lesions. Atherosclerosis 1991;89:11-24. [11]. Orlandi A, Marcellini M, Spagnoli LG. Aging influences development and progression of early aortic atherosclerotic lesions in cholesterol-fed rabbits. Arterioscler Thromb Vasc Biol 2000;20:1123-1136. 23 [12]. Cortés MJ, Díez-Juan A, Pérez P, Pérez-Roger I, Arroyo-Pellicer R, Andrés V. Increased early atherogenesis in young versus old hypercholesterolemic rabbits by a mechanism independent of arterial cell proliferation. FEBS Letters 2002;522:99-103. [13]. Fenton M, Huang HL, Hong Y, Hawe E, Kurz DJ, Erusalimsky JD. Early atherogenesis in sensescence-accelerated mice. Exp Gerontol 2004;39:115-122. [14]. Rauscher FM, Goldschmidt-Clermont PJ, Davis BH, et al. Aging, progenitor cell exhaustion, and atherosclerosis. Circulation 2003;108:457-463. [15]. Torella D, Leosco D, Indolfi C, et al. Aging exacerbates negative remodeling and impairs endothelial regeneration after balloon injury. Am J Physiol Heart Circ Physiol 2004:In press. [16]. Fleg JL, O'Connor F, Gerstenblith G, et al. Impact of age on the cardiovascular response to dynamic upright exercise in healthy men and women. J Appl Physiol 1995;78:890-900. [17]. Michel JB, Heudes D, Michel O, et al. Effect of chronic ANG I-converting enzyme inhibition on aging processes. II. Large arteries. Am J Physiol 1994;267:124-135. [18]. Li Z, Froehlich J, Galis ZS, Lakatta EG. Increased expression of matrix metalloproteinase-2 in the thickened intima of aged rats. Hypertension 1999;33:116123. [19]. Lakatta EG. Cardiovascular regulatory mechanisms in advanced age. Physiol Rev 1993;73:413-467. [20]. Virmani R, Avolio AP, Mergner WJ, et al. Effect of aging on aortic morphology in populations with high and low prevalence of hypertension and atherosclerosis. Comparison between occidental and Chinese communities. Am J Pathol 1991;139:1119-1129. 24 [21]. Lakatta EG. Arterial and cardiac aging: major shareholders in cardiovascular disease enterprises: Part III: cellular and molecular clues to heart and arterial aging. Circulation 2003;107:490-497. [22]. Cheng L, Mantile G, Pauly R, et al. Adenovirus-mediated gene transfer of the human tissue inhibitor of metalloproteinase-2 blocks vascular smooth muscle cell invasiveness in vitro and modulates neointimal development in vivo. Circulation 1998;98:2195-2201. [23]. Pauly RR, Passaniti A, Bilato C, et al. Migration of cultured vascular smooth muscle cells through a basement membrane barrier requires type IV collagenase activity and is inhibited by cellular differentiation. Circ Res 1994;75:41-54. [24]. Pauly RR, Passaniti A, Crow M, et al. Experimental models that mimic the differentiation and dedifferentiation of vascular cells. Circulation 1992;86:68-73. [25]. McCaffrey TA, Nicholson AC, Szabo PE, Weksler ME, Weksler BB. Aging and arteriosclerosis. The increased proliferation of arterial smooth muscle cells isolated from old rats is associated with increased platelet-derived growth factor-like activity. J Exp Med 1988;167:163-174. [26]. McCaffrey TA, Falcone DJ. Evidence for an age-related dysfunction in the antiproliferative response to transforming growth factor-beta in vascular smooth muscle cells. Mol Biol Cell 1993;4:315-322. [27]. Takasaki I, Chobanian AV, Sarzani R, Brecher P. Effect of hypertension on fibronectin expression in the rat aorta. J Biol Chem 1990;265:21935-21939. [28]. Challah M, Nadaud S, Philippe M, et al. Circulating and cellular markers of endothelial dysfunction with aging in rats. Am J Physiol 1997;273:1941-1948. [29]. Crawford DC, Chobanian AV, Brecher P. Angiotensin II induces fibronectin expression asscoiated with cardiac fibrosis in the rat. Circ Res 1994;74:727-739. 25 [30]. Avolio A. Genetic and environmental factors in the function and structure of the arterial wall. Hypertension 1995;26:34-37. [31]. Dart AM, Kingwell BA. Pulse pressure--a review of mechanisms and clinical relevance. J Am Coll Cardiol 2001;37:975-984. [32]. Blacher J, Asmar R, Djane S, London GM, Safar ME. Aortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patients. Hypertension 1999;33:11111117. [33]. Kaplan D, Meyer K. Mucopolysaccharides of aorta at various ages. Proc Soc Exp Biol Med 1960;105:78-81. [34]. Harding SE, Jones SM, O'Gara P, del Monte F, Vescovo G, Poole-Wilson PA. Isolated ventricular myocytes from failing and non-failing human heart; the relation of age and clinical status of patients to isoproterenol response. J Mol Cell Cardiol 1992;24:549-564. [35]. Orlandi A, Marcellini M, Spagnoli LG. Aging influences development and progression of early aortic atherosclerotic rabbitslesions in cholesterol-fed. Arterioscler Thromb Vasc Biol 2000;20:1123-1136. [36]. Belmin J, Corman B, Merval R, Tedgui A. Age-related changes in endothelial permeability and distribution volume of albumin in rat aorta. Am J Physiol 1993;264:679-685. [37]. Cernadas MR, Sanchez de Miguel L, Garcia-Duran M, et al. Expression of constitutive and inducible nitric oxide synthases in the vascular wall of young and aging rats. Circ Res 1998;83:279-286. [38]. Asai K, Kudej RK, Shen YT, et al. Peripheral vascular endothelial dysfunction and apoptosis in old monkeys. Arterioscler Thromb Vasc Biol 2000;20:1493-1499. 26 [39]. Hongo K, Nakagomi T, Kassell NF, et al. Effects of aging and hypertension on endothelium-dependent vascular relaxation in rat carotid artery. Stroke 1988;19:892897. [40]. Blackburn EH. Switching and signaling at the telomere. Cell 2001;106:661-673. [41]. Blasco MA. Mammalian telomeres and telomerase: why they matter for cancer and aging. Eur J Cell Biol 2003;82:441-446. [42]. Borges A, Liew CC. Telomerase activity during cardiac development. J Mol Cell Cardiol 1997;29:2717-2724. [43]. Cherif H, Tarry JL, Ozanne SE, Hales CN. Ageing and telomeres: a study into organand gender-specific telomere shortening. Nucleic Acids Res 2003;31:1576-1583. [44]. Prowse KR, Greider CW. Developmental and tissue-specific regulation of mouse telomerase and telomere length. Proc Natl Acad Sci U S A 1995;92:4818-4822. [45]. Coviello-McLaughlin GM, Prowse KR. Telomere length regulation during postnatal development and ageing in Mus spretus. Nucleic Acids Res 1997;25:3051-3058. [46]. Takubo K, Izumiyama-Shimomura N, Honma N, et al. Telomere lengths are characteristic in each human individual. Exp Gerontol 2002;37:523-531. [47]. Autexier C, Greider CW. Telomerase and cancer: revisiting the telomere hypothesis. Trends Biochem Sci 1996;21:387-391. [48]. Collins K, Mitchell JR. Telomerase in the human organism. Oncogene 2002;21:564579. [49]. Wright WE, Shay JW. Cellular senescence as a tumor-protection mechanism: the essential role of counting. Curr Opin Genet Dev 2001;11:98-103. [50]. Ulaner GA, Hu JF, Vu TH, Giudice LC, Hoffman AR. Tissue-specific alternate splicing of human telomerase reverse transcriptase (hTERT) influences telomere lengths during human development. Int J Cancer 2001;91:644-649. 27 [51]. Kumazaki T, Hiyama K, Takahashi T, et al. Differential gene expressions during immortalization of normal human fibroblasts and endothelial cells transfected with human telomerase reverse transcriptase gene. Int J Oncol 2004;24:1435-1442. [52]. Okuda K, Bardeguez A, Gardner JP, et al. Telomere length in the newborn. Pediatr Res 2002;52:377-381. [53]. Slagboom PE, Droog S, Boomsma DI. Genetic determination of telomere size in humans: a twin study of three age groups. Am J Hum Genet 1994;55:876-882. [54]. Friedrich U, Griese E, Schwab M, Fritz P, Thon K, Klotz U. Telomere length in different tissues of elderly patients. Mech Ageing Dev 2000;119:89-99. [55]. Jeanclos E, Schork NJ, Kyvik KO, Kimura M, Skurnick JH, Aviv A. Telomere length inversely correlates with pulse pressure and is highly familial. Hypertension 2000;36:195-200. [56]. Nawrot TS, Staessen JA, Gardner JP, Aviv A. Telomere length and possible link to X chromosome. Lancet 2004;363:507-510. [57]. Oh H, Schneider MD. The emerging role of telomerase in cardiac muscle cell growth and survival. J Mol Cell Cardiol 2002;34:717-724. [58]. Serrano AL, Andrés V. Telomeres and cardiovascular disease: does size matter? Circ Res 2004;94:575-584. [59]. Farhat MY, Lavigne MC, Ramwell PW. The vascular protective effects of estrogen. Faseb J 1996;10:615-624. [60]. Nathan L, Chaudhuri G. Estrogens and atherosclerosis. Annu Rev Pharmacol Toxicol 1997;37:477-515. [61]. Mendelsohn ME, Karas RH. The protective effects of estrogen on the cardiovascular system. N Engl J Med 1999;340:1801-1811. 28 [62]. Dubey RK, Jackson EK. Estrogen-induced cardiorenal protection: potential cellular, biochemical, and molecular mechanisms. Am J Physiol Renal Physiol 2001;280:F365-388. [63]. Leri A, Malhotra A, Liew CC, Kajstura J, Anversa P. Telomerase activity in rat cardiac myocytes is age and gender dependent. J Mol Cell Cardiol 2000;32:385-390. [64]. Benetos A, Okuda K, Lajemi M, et al. Telomere length as an indicator of biological aging: The gender effect and relation with pulse pressure and pulse wave velocity. Hypertension 2001;37:381-385. [65]. Kyo S, Takakura M, Kanaya T, et al. Estrogen activates telomerase. Cancer Res 1999;59:5917-5921. [66]. Simoncini T, Hafezi-Moghadam A, Brazil DP, Ley K, Chin WW, Liao JK. Interaction of oestrogen receptor with the regulatory subunit of phosphatidylinositol3-OH kinase. Nature 2000;407:538-541. [67]. Vasa M, Breitschopf K, Zeiher AM, Dimmeler S. Nitric oxide activates telomerase and delays endothelial cell senescence. Circ Res 2000;87:540-542. [68]. Kang SS, Kwon T, Kwon DY, Do SI. Akt protein kinase enhances human telomerase activity through phosphorylation of telomerase reverse transcriptase subunit. J Biol Chem 1999;274:13085-13090. [69]. Breitschopf K, Zeiher AM, Dimmeler S. Pro-atherogenic factors induce telomerase inactivation in endothelial cells through an Akt-dependent mechanism. FEBS Lett 2001;493:21-25. [70]. Miyauchi H, Minamino T, Tateno K, Kunieda T, Toko H, Komuro I. Akt negatively regulates the in vitro lifespan of human endothelial cells via a p53/p21-dependent pathway. Embo J 2004;23:212-220. 29 [71]. Finkel T, Holbrook NJ. Oxidants, oxidative stress and the biology of ageing. Nature 2000;408:239-247. [72]. Kurz DJ, Decary S, Hong Y, Trivier E, Akhmedov A, Erusalimsky JD. Chronic oxidative stress compromises telomere integrity and accelerates the onset of senescence in human endothelial cells. J Cell Sci 2004;117:2417-2426. [73]. Borras C, Esteve JM, Vina JR, Sastre J, Vina J, Pallardo FV. Glutathione regulates telomerase activity in 3T3 fibroblasts. J Biol Chem 2004. [74]. Furumoto K, Inoue E, Nagao N, Hiyama E, Miwa N. Age-dependent telomere shortening is slowed down by enrichment of intracellular vitamin C via suppression of oxidative stress. Life Sci 1998;63:935-948. [75]. Haendeler J, Hoffmann J, Brandes RP, Zeiher AM, Dimmeler S. Hydrogen peroxide triggers nuclear export of telomerase reverse transcriptase via Src kinase familydependent phosphorylation of tyrosine 707. Mol Cell Biol 2003;23:4598-4610. [76]. Haendeler J, Hoffmann J, Diehl JF, et al. Antioxidants inhibit nuclear export of telomerase reverse transcriptase and delay replicative senescence of endothelial cells. Circ Res 2004;94:768-775. [77]. Kawanishi S, Oikawa S. Mechanism of Telomere Shortening by Oxidative Stress. Ann N Y Acad Sci 2004;1019:278-284. [78]. Minamino T, Miyauchi H, Yoshida T, Ishida Y, H. Y, Komuro I. Endothelial cell senescence in human atherosclerosis. Role of telomere in endothelial dysfunction. Circulation 2002;105:1541-1544. [79]. Aviv H, Khan MY, Skurnick J, et al. Age dependent aneuploidy and telomere length of the human vascular endothelium. Atherosclerosis 2001;159:281-287. [80]. Chang E, Harley CB. Telomere length and replicative aging in human vascular tissues. Proc Natl Acad Sci USA 1995;92:11190-11194. 30 [81]. Okuda K, Khan MY, Skurnick J, Kimura M, Aviv H, Aviv A. Telomere attrition of the human abdominal aorta: relationships with age and atherosclerosis. Atherosclerosis 2000;152:391-398. [82]. von Zglinicki T, Serra V, Lorenz M, et al. Short telomeres in patients with vascular dementia: an indicator of low antioxidative capacity and a possible risk factor? Lab Invest 2000;80:1739-1747. [83]. Samani NJ, Boultby R, Butler R, Thompson JR, Goodall AH. Telomere shortening in atherosclerosis. Lancet 2001;358:472-473. [84]. Brouilette S, Singh RK, Thompson JR, Goodall AH, Samani NJ. White cell telomere length and risk of premature myocardial infarction. Arterioscler Thromb Vasc Biol 2003. [85]. Cawthon RM, Smith KR, O'Brien E, Sivatchenko A, Kerber RA. Association between telomere length in blood and mortality in people aged 60 years or older. Lancet 2003;361:393-395. [86]. Benetos A, Gardner JP, Zureik M, et al. Short telomeres are associated with increased carotid atherosclerosis in hypertensive subjects. Hypertension 2004;43:182-185. [87]. Jeanclos E, Krolewski A, Skurnick J, et al. Shortened telomere length in white blood cells of patients with IDDM. Diabetes 1998;47:482-486. [88]. Obana N, Takagi S, Kinouchi Y, et al. Telomere shortening of peripheral blood mononuclear cells in coronary disease patients with metabolic disorders. Intern Med 2003;42:150-153. [89]. Isner JM. Cancer and atherosclerosis: the broad mandate of angiogenesis. Circulation 1999;99:1653-1655. [90]. Carmeliet P. Angiogenesis in health and disease. Nat Med 2003;9:653-660. 31 [91]. Rivard A, Fabre JE, Silver M, et al. Age-dependent impairment of angiogenesis. Circulation 1999;99:111-120. [92]. Rivard A, Berthou-Soulie L, Principe N, et al. Age-dependent defect in vascular endothelial growth factor expression is associated with reduced hypoxia-inducible factor 1 activity. J Biol Chem 2000;275:29643-29647. [93]. Kurz DJ, Hong Y, Trivier E, et al. Fibroblast growth factor-2, but not vascular endothelial growth factor, upregulates telomerase activity in human endothelial cells. Arterioscler Thromb Vasc Biol 2003;23:748-754. [94]. Trivier E, Kurz DJ, Hong Y, Huang HL, Erusalimsky JD. Differential Regulation of Telomerase in Endothelial Cells by Fibroblast Growth Factor-2 and Vascular Endothelial Growth Factor-A: Association with Replicative Life Span. Ann N Y Acad Sci 2004;1019:111-115. [95]. Yang J, Nagavarapu U, Relloma K, et al. Telomerized human microvasculature is functional in vivo. Nat Biotechnol 2001;19:219-224. [96]. Murasawa S, Llevadot P, Silver M, Isner JM, Losordo DW, Asahara T. Constitutive human telomerase reverse transcriptase expression enhances regenerative properties of endothelial progenitor cells. Circulation 2002;106:1133-1139. [97]. Minamino T, Mitsialis SA, Kourembanas S. Hypoxia extends the life span of vascular smooths muscle cells through telomerase activation. Mol Cell Biol 2001;21:33363342. [98]. Pallini R, Pierconti F, Falchetti ML, et al. Evidence for telomerase involvement in the angiogenesis of astrocytic tumors: expression of human telomerase reverse transcriptase messenger RNA by vascular endothelial cells. J Neurosurg 2001;94:961971. 32 [99]. Falchetti ML, Pierconti F, Casalbore P, et al. Glioblastoma induces vascular endothelial cells to express telomerase in vitro. Cancer Res 2003;63:3750-3754. [100]. Blasco MA, Lee HW, Hande MP, et al. Telomere shortening and tumor formation by mouse cells lacking telomerase RNA. Cell 1997;91:25-34. [101]. Lee HW, Blasco MA, Gottlieb GJ, Horner JW, 2nd, Greider CW, DePinho RA. Essential role of mouse telomerase in highly proliferative organs. Nature 1998;392:569-574. [102]. Rudolph KL, Chang S, Lee HW, et al. Longevity, stress response, and cancer in aging telomerase-deficient mice. Cell 1999;96:701-712. [103]. Herrera E, Samper E, Martin-Caballero J, Flores JM, Lee HW, Blasco MA. Disease states associated with telomerase deficiency appear earlier in mice with short telomeres. Embo J 1999;18:2950-2960. [104]. Franco S, Segura I, Riese HH, Blasco MA. Decreased B16F10 melanoma growth and impaired vascularization in telomerase-deficient mice with critically short telomeres. Cancer Res 2002;62:552-559. [105]. Leri A, Franco S, Zacheo A, et al. Ablation of telomerase and telomere loss leads to cardiac dilatation and heart failure associated with p53 upregulation. Embo J 2003;22:131-139. [106]. Wong KK, Maser RS, Bachoo RM, et al. Telomere dysfunction and Atm deficiency compromises organ homeostasis and accelerates ageing. Nature 2003;421:643-648. [107]. Poch E, Carbonell P, Franco S, Díez-Juan A, Blasco MA, Andrés V. Short telomeres protect from diet-induced atherosclerosis in apolipoprotein E-null mice. FASEB J 2004;18:418-420. 33 [108]. Cao Y, Li H, Mu F-T, Ebisui O, Funder JW, Liu J-P. Telomerase activation causes vascular smooth muscle cell proliferation in genetic hypertension. FASEB J 2002;16:96-98. [109]. Hamet P, Thorin-Trescases N, Moreau P, et al. Workshop: excess growth and apoptosis: is hypertension a case of accelerated aging of cardiovascular cells? Hypertension 2001;37:760-766. [110]. Samper E, Flores JM, Blasco MA. Restoration of telomerase activity rescues chromosomal instability and premature aging in Terc-/- mice with short telomeres. EMBO Rep 2001;2:800-807. [111]. Kalka C, Masuda H, Takahashi T, et al. Transplantation of ex vivo expanded endothelial progenitor cells for therapeutic neovascularization. Proc Natl Acad Sci U S A 2000;97:3422-3427. [112]. Allsopp RC, Morin GB, Horner JW, DePinho R, Harley CB, Weissman IL. Effect of TERT over-expression on the long-term transplantation capacity of hematopoietic stem cells. Nat Med 2003;9:369-371. [113]. McKee JA, Banik SS, Boyer MJ, et al. Human arteries engineered in vitro. EMBO Rep 2003;4:633-638. [114]. Minamino T, Kourembanas S. Mechanisms of telomerase induction during vascular smooth muscle cell proliferation. Circ Res 2001;89:237-243. [115]. Hastings R, Qureshi M, Verma R, Lacy PS, Williams B. Telomere attrition and accumulation of senescent cells in cultured human endothelial cells. Cell Prolif 2004;37:317-324. [116]. Yang J, Chang E, Cherry AM, et al. Human endothelial cell life extension by telomerase expression. J Biol Chem 1999;274:26141-26148. 34 A TELOMERE-ASSOCIATED PROTEINS p-arms TERT, hPOT1, TRAF1, TRAF2, TANK1, TANK2, TIN2, hRAP1, RAD50, NBS1, MRE11, Ku86, DNA-PKcs q-arms TERT Human: ~10 Kb Mouse: ~40 Kb C TTAGGG TTAGGGTTAGGG CAAUCCCAAUC AATCCC Telomeric DNA Telomerase activity Telomere length Germ cell line Tumors Immortal cells High Somatic tissues Primary cells Human premature aging syndromes Telomerase RNA (Terc) TELOMERE MAINTENANCE Genomic stability High proliferative capacity TELOMERE DYSFUNCTION Low or absent Chromosomal abnormalities Genomic instability Growth arrest, apoptosis Number of cell divisions or Age Figure 1: Telomere integrity and cellular homeostasis. A. Left: Schematic showing telomeres (black circles) at both ends of chromosomes. Right: Enlargement of the telomere showing the human telomeric DNA tandem repeat sequence, the telomeric RNA component (Terc), the catalytic telomerase reverse transcriptase (TERT) subunit, and additional telomerase-associated proteins. B. Telomere attrition occurs progressively in somatic cells with each mitotic cycle during normal aging and passage in culture, due in part to low or absent telomerase activity. In contrast, high telomerase activity in germ and tumor cells allows the maintenance of telomere integrity and an extended proliferative capacity. Accelerated telomere erosion is a characteristic of several human premature aging syndromes (i. e., Werner syndrome, ataxia telangectasia, dyskeratosis congenita). 35 HUMAN STUDIES • Coronary and carotid arteriosclerosis 83,86 • Premature myocardial infarction 84 • Hypercholesterolemia and diabetes mellitus 87,88 • Hypertension 55,64,86 BLOOD CIRCULATING LEUKOCYTES Telomere shortening Vessels subjected to higher atherogenic hemodynamic stress 78,80 ARTERIAL TISSUE Greater age-related telomere shortening ANIMAL STUDIES Spontaneously hypertensive rats AORTA / KIDNEY • Activation of telomerase and telomere lengthening in aorta before onset of hypertension 108 • Telomere attrition in the kidney 109 Lategeneration Terc-null mice (with critically short telomeres) ARTERIAL TISSUE • Reduced atherogenesis when combined with apoE-null genotype 107 • Attenuated angiogenesis 104 Figure 2: Telomeres and telomerase in atherosclerosis and hypertension. Human (left) and animal (right) studies that have implicated telomere length and telomerase activity in atherosclerosis and hypertension are summarized. Successive generations of Terc-null mice are necessary to reach critically short telomeres and associated diseases. Reference numbers are shown in parenthesis.