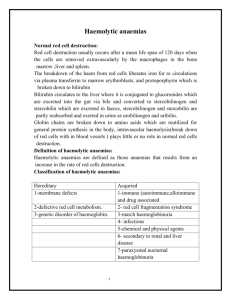
Acquired Haemolytic anaemia
advertisement

Acquired Haemolytic anaemia http://www.usmlemcq.com/ Acquired Haemolytic Anaemia Immune 1.Autoimmune *warm Ab *cold Ab Non Immune 1.Mechanical *March haemoglobinuria *Prosthetic heart valves 2.Alloimmune *Transfusion rn *HDN 3.Infections *Malaria *Clostridium welchii 4.Burns 5.Drugs *Dapsone 6.PNH 2.MAHA http://www.usmlemcq.com/ 18 year old girl C/O - fever, yellow discolouration of eyes and abdominal pain – 2 weeks O/E – Pale ++ , Icteric +, Spleen – 1cm 1. How would you confirm haemolysis? 2. What are the possible causes? http://www.usmlemcq.com/ Warm autoimmune haemolytic anaemia Antibodies optimally active at 370. IgG Causes *Idiopathic *secondary SLE CLL Lymphomas Drugs- Methyl dopa http://www.usmlemcq.com/ Warm autoimmune haemolytic anaemia cont. Pathogenesis IgG antibodies are present on the red cells, some of them also bind complement(C3) Red cells are destroyed mainly in the RE system (preferentially spleen) http://www.usmlemcq.com/ Warm autoimmune haemolytic anaemia cont. Clinical features Haemolytic anaemia Jaundice Splenomegaly Investigations Reticulocytosis Spherocytes Increased serum bilirubin Positive direct coomb test http://www.usmlemcq.com/ Warm autoimmune haemolytic anaemia cont. Treatment Corticosteroids Splenectomy Immunosuppresives- Azathioprine Folic acid Treat underlying cause http://www.usmlemcq.com/ Cold autoimmune haemolytic anaemia Auto antibodies (IgM) that react best at temp. <370 (0-40) Causes *Idiopathic (CHAD) *secondary Mycoplasma Infectious mononucleosis Lymphoma SLE http://www.usmlemcq.com/ Cold autoimmune haemolytic anaemia cont. Investigations Anaemia with red cell agglutinates Macrocytosis Reticulocytosis Positive direct coomb test Features of IV haemolysis http://www.usmlemcq.com/ RBC – 1.1x1012/l HB - 6.2g/dl MCV – 112fl Cold autoimmune haemolytic anaemia cont. Clinical features Some have acute IV haemolysis & Hburia in cold weather but maintain a normal Hb in warm weather Others have a compensated chronic haemolysis with a mild to moderate reduction of Hb. Acrocyanosis, Raynauds phenomenon due to agglutinates. Spleen may not be enlarged http://www.usmlemcq.com/ Cold autoimmune haemolytic anaemia cont. Investigations Anaemia with red cell agglutinates Macrocytosis Reticulocytosis Positive direct coomb test Features of IV haemolysis http://www.usmlemcq.com/ Cold autoimmune haemolytic anaemia cont. Treatment Avoid cold May need blood transfusions Rituximab (monoclonal anti CD20) Chlorambucil Plasmapheresis has been used Corticosteroids and splenectomy are rarely of any benefit http://www.usmlemcq.com/ Allo immune http://www.usmlemcq.com/ ABO & Rh incompatibilty Haemolytic transfusion reactions may be immediate or delayed. Immediate life threatening reactions associated with massive IV haemolysis is seen with complement activating antibodies of IgM & IgG classes(ABO antibodies) Severity of the reaction depends on the recipient’s titre of antibody http://www.usmlemcq.com/ ABO & Rh incompatibilty cont. Extra vascular haemolytic transfusion reactions are seen with the immune antibodies( IgG, unable to bind complement). The only feature may be unexplained anaemia with jaundice http://www.usmlemcq.com/ Non immune causes of haemolysis Mechanical causes of haemolysis Red cells may be injured by excess physical trauma as they circulate through the vascular system. http://www.usmlemcq.com/ Mechanical haemolytic anaemia Cardiac – Occasional complication of open heart surgical procedures eg. valve prostheses. In severe cases marked anaemia with intravascular haemolysis. March haemoglobinuria – Hbnaemia & Hburia following strenuous exercise in healthy young adult males. Traumatic effect on the blood within vessels of sole. soldiers, athletes, karatekas. http://www.usmlemcq.com/ Microangiopathic haemolytic anaemia Mechanical haemolytic anaemia in which the red cell fragmentation is due to contact between red cells & abnormal intima of partly thrombosed, narrowed, or necrotic small vessels. http://www.usmlemcq.com/ Microangiopathic haemolytic anaemia With associated thrombocytopaenia 1.Disseminated intravascular coagulation 2.Haemolytic uraemic syndrome 3.Thrombotic thrombocytopaenic purpura 4. HELLP syndrome http://www.usmlemcq.com/ DIC Widespread intra vascular coagulation induced by pro coagulants (that overcome the natural anti coagulant mechanisms), resulting in the formation of thrombin. These pro coagulants may be produced in the blood or introduced from out side the circulatory system egsnake venom This results inFormation of micro thrombi Ischemia Consumption of platelets & clotting factors Bleeding http://www.usmlemcq.com/ DIC cont. Causes *Trauma *Cancers *Bacteraemia *Severe Haemorrhage *Obstetric & surgical events http://www.usmlemcq.com/ DIC cont. Investigations Fragmented red cells Low platelet count Prolongation of PT, aPTT, TT, Low fibrinogen Elevated FDP, D dimers http://www.usmlemcq.com/ HUS-TTP Initially described as two distinct entities but thereafter thought to be two ends of the same spectrum. ? Two distinct entities Formation of platelet thrombi (hyaline thrombi) in terminal arterioles & capillaries. Microangiopathic haemolytic anaemia with Thrombocytopaenia http://www.usmlemcq.com/ HUS-TTP Clinical features Fever Neurological symptoms Renal failure + MAHA Thrombocytopenia Coagulation screen – NORMAL LDH - high http://www.usmlemcq.com/ Causes of HUS E.Coli o157 toxin Shigella dysenteriae http://www.usmlemcq.com/ TTP Pathogenesis Presence of abnormal vwf (platelet adhesion) Deficiency of vwf cleaving proteases ADAMTS-13 Increase in vwf activity, platelet aggregation Microthrombi formation http://www.usmlemcq.com/ Causes of TTP Inherited deficiency of ADAMTS 13 • Present in neonatal period Acquired deficiency of ADAMTS 13 • Drugs- clopidogrel, ticlopidine, ciclosporine • Post transplant • Pregnancy • SLE http://www.usmlemcq.com/ TTP Treatment Plasma exchange FFP/CPP Steroids / immunosuppresion Platelets not given Rituximab http://www.usmlemcq.com/ HELLP syndrome HELLP syndrome occurs in approximately 0.2 to 0.6 % of all pregnancies. Pre eclampsia occurs in 5 to 7 % percent of pregnancies. Superimposed HELLP syndrome develops in 4 to 12 percent of women with pre eclampsia or eclampsia. http://www.usmlemcq.com/ HELLP The pathogenesis of HELLP is not well understood. Findings are attributed to abnormal vascular tone, vasospasm and coagulation defects. No common precipitating factor has been found. Some insult that leads to microvascular endothelial damage and intravascular platelet activation. Platelet activation, causing vasospasm, platelet agglutination and aggregation, and further endothelial damage. Fibrin forms networks in the small bld vsl. Liver appears to be the main site of this process This cascade is only terminated with delivery. http://www.usmlemcq.com/ HELLP MAHA. Elevated liver enzyme levels are thought to be secondary to obstruction of hepatic blood flow by fibrin deposits in the sinusoids. This obstruction leads to periportal necrosis and, in severe cases, intrahepatic haemorrhage, subcapsular hematoma or hepatic rupture. The thrombocytopenia has been attributed to increased consumption and/or destruction of platelets. http://www.usmlemcq.com/ HELLP PT, APTT, Fbrinogen usually normal DIC is also seen in about 20% of all women with HELLP syndrome Fibrinogen <3g/l in this setting suspect DIC http://www.usmlemcq.com/ Infections Malaria – anaemia is often only mild *can be severe esp.with falciparum infections *Blackwater fever rare but serious complication, seen in endemic areas & in those who have repeated attacks. Pptd by antimalarial drugs. *Diagnosis by demonstrating the parasite. *Antigen tests http://www.usmlemcq.com/ Infections Clostridium welchii – due to direct action of toxin *mostly post abortal or puerperal infections *Intra vascular spherocytic anaemia, retic count not very high http://www.usmlemcq.com/ Drugs Due to direct toxic effects in normal subjects *Sulphasalazine Haemolysis in subjects with metabolic abnormality G6PD def *Primaquine, Nitrofurantoin Due to a immune mechanism *Quinine, Penicillin, Sulphonamides Toxins – Snake bite http://www.usmlemcq.com/ Paroxysmal Nocturnal Haemoglobinuria Acquired chronic intra vascular haemolysis May have thrombosis and pancytopenia Nonmalignant clonal expansion of one or several hematopoietic stem cells that have acquired a somatic mutation of PIGA Affected stem cells are deficient in glycosyl phosphatidylinositol–anchored proteins (GPI-APs) http://www.usmlemcq.com/ http://www.usmlemcq.com/ Urine haemosiderin HAM test Flow cytometry for GPI –AP LDH Transfusion Iron replacement http://www.usmlemcq.com/ 14 year old boy C/O - fever, yellow discolouration of eyes and abdominal pain – 2 weeks O/E – Pale ++ , Icteric +, Spleen – 1cm What are the first line investigations? http://www.usmlemcq.com/