Pathology of testis
Dr: Salah Ahmed
Cryptorchidism and Testicular Atrophy
Cryptorchidism:- failure of testicular descent into the scrotum
- Normally the testes descend from the coelomic cavity into the pelvis by the third
month of gestation and then through the inguinal canals into the scrotum during the
last 2 months of intrauterine life
- occurs in about 1% of the male population
- Approximately 10% of cases are bilateral
- in the majority of cases the cause is unknown but it may be due to:
1- hormonal abnormalities
2- intrinsic testicular abnormalities
3- mechanical problems (e.g., obstruction of the inguinal canal)
- Morphology: tubular atrophy usually accompanied by hyperplasia of Leydig cells
- complications: 1-testicular atrophy 2- sterility 3- malignant transformation
- treatment: orchiopexy (must be performed as soon as possible)
Testicular atrophy:- may be associated with :
1- orchitis , especially mumps orchitis
2- trauma
3- cryptorchidism
4- Klinefelter`s syndrome
5- chronic debilitating disease
6- old age
7- hormonal excess or deficiency ( liver cirrhosis, estrogen therapy, hypothalamus
or pituitary disorders )
8- radiation and chemotherapy
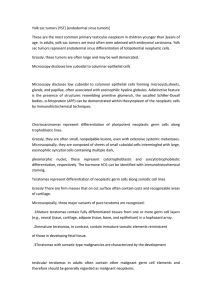
Atrophied testis secondary to cryptorchidism
Normal
testicular atrophy
Inflammatory Lesions
- Inflammatory lesions are more common in the epididymis than in the testis
- called orchitis, epididymitis, epididymo-orchitis
- associated with: 1- venereal disease
2- nonspecific infections:- usually secondary to UTI
- the infections reach the testes through the vas deferens or
lymphatics of the spermatic cord
3- mumps
4- tuberculosis
- C\F: fever, testicular swelling, tenderness
Testicular Neoplasms
- are the most important cause of firm, painless enlargement of the testis
- occur roughly in 5 per 100,000 males, with a peak incidence between 20 and 34
years
- include: 1- germ cell tumors
2- sex cord/stromal tumors (derived from Sertoli or Leydig cells)
- 95% of testicular tumors arise from germ cells, and always are malignant
- sex cord/stromal tumors are uncommon, usually benign
Germ cell tumors:
Pathogenesis:
- The cause of testicular tumors remains unknown but the risk increases in:
1- cryptorchidism
2- gonadal dysgenesis (Klinefelter`s , testicular feminization syndromes)
3- isochromosome of the short arm of chromosome 12
4- siblings of males with testicular cancer
5- contralateral testis (the other with cancer)
6- whites
- It is now widely believed that most testicular tumors arise from in situ lesions
(intratubular germ cell neoplasia) This lesion is present in cryptorchidism, dysgenetic
testes
Germ cell tumors include:
1- Seminomas: 1- classic seminomas:
- account for about 50% of testicular germ cell tumors
- They are histologically identical to ovarian dysgerminomas and to germinomas
occurring in the central nervous system
- Morphology:
- Large tumors may contain foci of necrosis, usually without
hemorrhage
- the cells express hCG
- metastases to regional lymph nodes
2- spermatocytic seminoma:
Seminoma
:- soft usually gray-white tumors
(nests of large cells with distinct borders, clear cytoplasm and round nuclei with
prominent nucleoli, separated by fibrous septa with lymphocytic infiltration)
- tend to occur in older patients than classic
- contain a mixture of medium-sized cells, large uninucleate or multinucleate tumor
cells, and small cells with round nuclei
- not associated with intratubular germ cell neoplasia
- metastases are rare, in contrast to classic
2- Embryonal carcinomas:
- Pure embryonal carcinomas comprise 2% to 3% of all testicular germ cell tumors
- most cases are mixed with other germ cell tumors (yolk sac carcinoma, teratoma,
choriocarcinoma)
- Morphology:
- ill-defined, invasive masses
- containing foci of hemorrhage and necrosis
- composed of large and primitive looking cells
- ill-defined mass
- composed of large and primitive looking cells, with basophilic cytoplasm, indistinct cell
borders, and large nuclei with prominent nucleoli in solid sheets, glandular pattern and irregular
papillae
3- Yolk sac tumors (endodermal sinus tumors):
- are the most common testicular tumors in children younger than 3 years
- In adults, yolk sac tumors are most often seen admixed with embryonal carcinoma.
- Morphology: - large and well demarcated
- A distinctive feature is the presence of structures resembling
primitive glomeruli called Schiller-Duvall bodies
- the tumor cells express α-fetoprotein (AFP)
microcystic tissue and a papillary structure resembling a developing
glomerulus. hyaline droplets of α-fetoprotein is present
4- Testicular choriocarcinomas:
- it is a rare tumor
- highly malignant tumor
- pure choriocarcinoma is rare, accounting < 1% of all germ cell tumors . More
common as mixed pattern
- Morphology: - Grossly, the tumors are often small, nonpalpable even with extensive
systemic metastases
- Microscopically, choriocarcinomas are composed of sheets of small
cells (cytotrophoblast) irregularly intermingled with large,
eosinophilic cells containing multiple dark nuclei (syncytiotrophoblast)
with hemorrhage
- The cells express hCG
Composed of small cells intermingled with large eosinophilic
cells with multiple nuclei
5- Testicular teratomas:
- Morphology: - tumors form firm masses that on cut surface often contain cysts
- three variants of teratoma:
a) Mature teratoma: contains fully differentiated tissues from one or more
germ cell layers (e.g., neural tissue, cartilage, adipose tissue, bone, epithelium)
b) Immature teratoma: contains immature elements (fetal tissue)
c) Teratoma with somatic-type malignancies: characterized by the
development of frank malignancy in preexisting teratomatous elements,
usually in the form of a squamous cell carcinoma or adenocarcinoma
- Pure teratomas in prepubertal males are usually benign
- In adults commonly are malignant, metastasize in as many as 37% of cases
6- Mixed germ cell tumors: account for approximately 40% of all testicular germ cell
neoplasms. Combinations of any of the described patterns may occur in mixed tumors, the
most common of which is a combination of teratoma, embryonal carcinoma, and yolk sac
tumors.
Mature teratoma
Testicular teratomas contain mature cells from endodermal, mesodermal, and ectodermal lines.
Pictured here are four different fields from the same tumor containing (A) neural (ectodermal),
(B) glandular (endodermal), (C) cartilaginous (mesodermal), and (D) squamous epithelial
elements
Clinical Features:
- Clinically, it is best to consider tumors under two categories:
1- Seminomas
2- nonseminomatous
- patients present most frequently with painless enlargement of the testis
1- Seminomas confined to the testis for prolonged intervals and may reach
considerable size before diagnosis
- Metastases are most commonly encountered in the iliac and para-aortic lymph
nodes
- Hematogenous metastases occur later (liver, lungs)
2- nonseminomatous tumors may have widespread metastases at diagnosis, in the
absence of a palpable testicular lesion
- tend to metastasize earlier, by both lymphatic and hematogenous routes
Stages:- Testicular germ cell neoplasms are staged as follows:
Stage I: Tumor confined to the testis II: Regional lymph node metastases only
III: lymph node and/or distant organ metastases
Thank you
Infertility
Mumps (unilateral / Bilateral)- temporary infertility. •
Cryptorchidism ( unilateral / bilateral). •
Chronic alcoholism ( Bilateral) •
Chronic Ischemia ( unilateral / bilateral) •
Chemotherapy or radiation ( Bilateral) •
Hydrocele and Varicocele
Klinefelter's syndrome : patient present with gyenecomastia. •
Sertoli cell-only syndrome : No Sperm-Producing Cells, tubules contain only Sertoli
cells.
•
 0
0