Correlates and predictors of recurrent depression 1
Correlates and Predictors of Recurrent Depression
Kathryn Fox
Research Mentors: Judy Garber, Ph.D., Matt Morris, M.S., and Chrystyna Kouros, Ph.D.
Correlates and predictors of recurrent depression 2
Abstract
Depression is a recurrent and debilitating disorder affecting nearly 340 million people
worldwide. The present study examined what differentiates individuals with a history of one or
more major depressive episodes (MDEs) from individuals who have never been depressed as
well as examine which of these differentiating factors predict subsequent depressive symptoms
during a six-month follow-up. Participants were 108 young adults, ages 18-30 years old. No
participant was in a current MDE at time one; 56 individuals had a history of one or more MDE
and 46 had no history of psychiatric diagnoses. Those with a history of depression had higher
rates of physical abuse in childhood, maladaptive coping styles, and stressors than the neverdepressed controls. At the follow-up, number of stressors, dysfunctional attitudes, maladaptive
coping, and some forms of early childhood maltreatment interacting with stress predicted
depressive symptoms.
Correlates and predictors of recurrent depression 3
Depression is a pervasive and debilitating disorder affecting nearly 340 million people
worldwide (Greden, 2001). The experience of one major depressive episode (MDE) is associated
with a variety of problems including absenteeism and decreased productivity at work, increased
mental health care costs, and familial problems. Major depression also is quite recurrent; at least
60% of people who have suffered from one episode of depression will have a second, 70% of
those who have had two depressive episodes will have a third, 90% of individuals who have had
three depressive episodes will have a fourth, and many of these individuals then go on to
experience repeated episodes throughout their lifetimes (DSM–IV–TR; American Psychiatric
Association, 2000). Moreover, this pattern of recurrence is frequently accompanied by increased
severity over time (Greden, 2001).
Evidence of an association between the experience of stressful life events and the onset
and recurrence of major depressive disorder (MDD) has been reported consistently (e.g.,
Kendler, Karkowski, & Prescott, 1999; Monroe & Harkness, 2005; Stroud, Davila, & Moyer,
2008). First episodes of MDD tend to be strongly associated with stressful life events (SLEs),
whereas the relation between SLEs and depression changes over the course of the disorder
(Monroe & Harkness, 2005; Morris, Ciesla, & Garber, 2010; Stroud et al., 2008). Several
explanations have been proposed to account for these alterations in the relation of stressful life
events to depression including the kindling hypothesis, stress autonomy, and stress sensitization
(Monroe & Harkness, 2005).
The kindling hypothesis stems from the “consistent empirical finding that the association
between major life stress and episode onset weakens from a first episode over successive
recurrences” (Monroe & Harkness, 2005, p. 420). In their meta-analysis of thirteen previous
Correlates and predictors of recurrent depression 4
studies examining the role of stress in precipitating MDEs, Stroud and colleagues (2008) found
that severe stressful life events were more likely to precipitate the first depressive episode as
compared to recurrences. Monroe & Harkness (2005) suggested two explanations for this
phenomenon: stress autonomy and stress sensitization. The stress autonomy hypothesis proposes
that the relation between stress levels and depression progressively diminishes with each MDE,
such that eventually depressive episodes occur seemingly unrelated to any known stressors. In
contrast, the stress sensitization hypothesis asserts that stressful events become increasingly more
capable of activating depressive symptoms, leading to the negative correlation between number
of depressive episodes experienced and the level of stress necessary to trigger an episode.
Therefore, the results from the meta-analysis by Stroud et al. (2008) can be explained either by
the diminishing association between stress and depression (i.e., stress autonomy) or by the
increased ability of minor stressors to predict depressive episodes (i.e. stress sensitization).
Morris and colleagues (2010) found evidence consistent with the stress sensitization
hypothesis through a “stress activation model.” According to this model, the relation between
stress and depressive symptoms strengthens with repeated episodes, such that the activation
threshold is lower at all levels of stress, ranging from major stressors to daily hassles. Morris et
al. reported a stronger positive correlation between stress levels and depressive symptoms as a
function of number of prior MDEs. That is, following the stress activation model, adolescents
who had experienced one or more prior MDEs became increasingly sensitized to both major and
minor stressors, leading to a greater number of potential depression-triggering events and a
higher level of depressive symptoms.
The relation between stress and depressive symptoms is not necessarily uni-directional
(Liu & Alloy, 2010). Not only do stressors affect depressive symptoms, but depressive
Correlates and predictors of recurrent depression 5
symptoms also affect the amount of stress experienced. That is, depressed individuals have been
found to generate some of the stressors they encounter (Hammen, 1991), possibly as a result of
maladaptive coping, personality characteristics, and dysfunctional social networks (Hankin &
Abramson, 2001; Harkness et al., 1999). Stressful life events can be categorized as independent
or dependent upon the individual’s behaviors. For example, an independent event might be “a
family member getting sick,” whereas a dependent event might be “getting fired from a job for
being late too often.” Harkness and colleagues (1999) found that both recurrently depressed and
never depressed individuals experienced the same number of independent SLEs, whereas
recurrently depressed participants experienced more dependent stressful events than the nondepressed controls. Interestingly, they found that only daily hassles, but not severe, dependent
SLEs occurred more frequently in the recurrent depressives.
Whether the stressors are dependent or independent, longitudinal studies are needed to
explore the prospective link between stressors and depression are needed to determine how these
relations unfold over time. A few studies have examined the longitudinal relation of stressful
events and depressive episodes (e.g., Kendler, Karkowsi, & Prescott, 1998; Morris et al., 2010).
In a sample of adult females, Kendler and colleagues (1998) found a significant temporal
association between the occurrence of stressful life events and the onset of major depression.
They examined the timing of the stressors to the nearest month, but did not examine the duration.
Furthermore, they only examined the onset of major depression in the month in which the
stressor occurred, due to the assumption that the depressogenic impact of stressful life events
occurs shortly after the event, thus not examining the time in which the stressors impact is
strongest as well as leaving out the possibility for a longer-lasting effect.
Correlates and predictors of recurrent depression 6
Adjusting for these problems, Morris et al. (2010) examined the predictive association of
total stress levels to depressive symptoms, on a week-to-week basis, avoiding the use of a fixed
risk period for the effect of the stressor on depressive symptoms. They found that the effect of
stressors on depressive symptoms peaked at two weeks and lasted up to 26 weeks. One aim of
the current study was to replicate these findings in a different sample.
A particularly salient negative life event is the experience of maltreatment during
childhood (Harkness, Bruce, & Lumley, 2006), including physical, emotional, and sexual abuse
and emotional or material neglect. These early life experiences likely create a diathesis that
leaves these individuals vulnerable to depression after future encounters with stress (Harkness, et
al., 2006; Morris et al., 2010). For example, in the retrospective study, Harkness and colleagues
found that participants with a history of child abuse experienced less threatening life events prior
to their first depressive episode than did controls, or those without this abuse experience.
Moreover, those with a history of child maltreatment reported higher threat levels to chronic
difficulties than others. Thus, this study demonstrated increased sensitivity to future stressors
among individuals with a history of maltreatment. For those without an abuse history, this
increased vulnerability only occurred after the occurrence of their first depressive episode.
Interestingly, Harkness et al. noted a stronger sensitization to independent than dependent life
events, highlighting that not only the generation of stressful events predicted recurrence, but also
sensitivity to independent life events. Although Harkness and colleagues (2006) noted that
previously abused individuals evidenced a higher vulnerability to stressful events, they did not
examine whether these individuals also differed with regard to other factors such as coping or
cognitions. Investigating the interplay among maladaptive coping, cognitions, and childhood
Correlates and predictors of recurrent depression 7
maltreatment could further differentiate those individuals who do and do not develop subsequent
depressive episodes.
Maladaptive coping responses to stress also have been found to be associated with
depression, particularly disengagement and involuntary engagement coping strategies (Compas
et al, 2001; Connor-Smith et al., 2000). Disengagement coping (e.g., avoidance, denial) tends to
reinforce individuals’ negative expectations by preventing the acquisition of counter-evidence
through experience. Involuntary engagement coping, characterized by rumination or emotional
numbing, also has been found to be positively correlated with depression severity and recurrence
(Nolen-Hoeksema, 2000).
In contrast, primary control coping, involving problem solving and other active coping
strategies aimed at taking control of a stressful event, is related to lower levels of internalizing
and externalizing symptoms (Compas et al., 2001; Connor-Smith et al., 2000). Similarly,
secondary control coping, in which individuals try to adapt to a situation through cognitive
reframing, acceptance, or distraction, is negatively correlated with levels of both internalizing
and externalizing symptoms (Connor-Smith et al., 2000). Although prior research has
demonstrated significant concurrent relations among these various forms of coping and
depressive symptoms, longitudinal designs are needed to explore the direction of association
between coping and adjustment (Compas et al., 2001).
Finally, dysfunctional attitudes are a cognitive vulnerability, which also correlate with
depression and recurrence. Beck (2008) has argued that early adverse events foster negative
attitudes and biases that are then assimilated into self-schemas, which consist of various attitudes
and beliefs about the self, the world, and future. Examples of dysfunctional attitudes linked with
depression include “I am nothing if a person I love doesn’t like me” or “If I fail at my work, then
Correlates and predictors of recurrent depression 8
I am a failure as a person.” These maladaptive attitudes can affect how individuals appraise and
process new information and consequently increase the likelihood of subsequent depression.
Over time, such beliefs are reinforced through repeated use and eventually become resistant to
change. Accordingly, people with dysfunctional attitudes who react negatively to life events are
at increased risk for depression. Although dysfunctional attitudes are correlated with depression
severity (Scott et al., 1995), when individuals with this cognitive vulnerability are not
experiencing depressive symptoms, they are indistinguishable from those without the
vulnerability (Monroe & Harkness, 2005). Once confronted with a stressor, however, these
individuals are more likely to develop depressive symptoms.
The current study examined the following research questions and hypotheses. First, what
differentiates individuals who have experienced a prior major depressive episode (MDE) from
those without a history of depression? In particular, we compared individuals with and without a
history of depressed with regard to the number of stressful life events in the last six months,
coping styles, dysfunctional attitudes, and history of maltreatment during childhood. We
predicted that individuals with a history of mood disorders would report significantly more
negative life events, greater use of both disengagement and involuntary engagement coping and
less primary and secondary control coping, more dysfunctional attitudes, and greater
maltreatment during childhood.
Second, we were explored whether there was a predictive relation between stress and
depression severity? Following the methodology used by Morris et al. (2010), we examined the
relation of total level of stressors to depressive symptoms over time to determine when the
predictive relation between the two was strongest. We expected that high levels of stress would
Correlates and predictors of recurrent depression 9
significantly predict elevations in depression severity, and would be strongest at around seven to
eight weeks, as had been found previously.
Finally, what variables will predict depressive symptoms over time? We hypothesized
that history of childhood abuse, use of maladaptive coping styles, and high levels of
dysfunctional attitudes, would predict higher levels of depressive symptoms at the six-month
follow-up, controlling for Time 1 depressive symptoms.
Method
Participants. Participants were 108 young adults ages 18-30 years old (mean age = 22.97,
SD = 3.87) who were involved in a larger study examining the relations among stress, cortisol,
and history of depression. Of the 108 participants, 56 (52%) had a history of at least one MDE
and 46 had no history of psychiatric diagnoses; in the prior history group, 17 were males (15.7%)
and 39 were females (36.11%); the never depressed group consisted of 20 males (18.5%) and 26
females (24%). Participants were recruited through the Vanderbilt University subject pool, and
flyers around campus and in the local community. Potential participants were screened regarding
their current and past psychiatric disorders using the Mood Disorders and PTSD sections of the
Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I; First et al., 1996).
Inclusion criteria were either a history of one or more prior major depressive episodes or
no history of an MDE. Exclusion criteria were: (a) currently meets criteria for an MDE, (b)
current or past post-traumatic stress disorder (PTSD) or bipolar disorder. These were assessed
using the relevant sections of the SCID. Eligible individuals then were asked to complete a
battery of questionnaires and to come to the lab to participate in an experiment. Only those
measures used in the present study are described here.
Correlates and predictors of recurrent depression 10
Measures. Participants completed the following measures at the first assessment (Time
1): (a) the Response to Stress Questionnaire (RSQ; Connor-Smith, Compas, Wadsworth,
Thomsen, & Saltzman, 2000) consisting of 57 items assessing what participants do, think, and
feel in response to stressors (i.e., assessing utilization of voluntary and involuntary coping
strategies) on a 4-point scale of “not at all” to “a lot,” the measure received a Cronbach’s alpha
of .862 in our sample; (b) the Events Scale (ES; Compas, Davis, Forsythe, & Wagner, 1987)
assessing 90 events, both positive and negative, experienced in the previous six months as well
as their perceived valence, on a 7-point scale ranging from very negative to very positive; (c) the
Childhood Trauma Questionnaire (CTQ; Bernstein et al., 1994) a 28 item self-report
retrospective measure assessing the frequency of different types of abuse on a 5-point scale from
“never true” to “very often true” and demonstrates good reliability and validity, the measure
received a Cronbach’s alpha of .690 in our sample; (d) the Dysfunctional Attitudes Scale (DAS;
Weissman & Beck, 1978), a 40-item self-report measure of attitudes and beliefs about the self
and others, the measure received a Cronbach’s alpha of .764 in our sample; (e) the Structured
Clinical Interview for the DSM (SCID-1; Mood Disorders Section; PTSD); (f) Beck Depression
Inventory, second edition (BDI-II; Beck, Steer, & Brown, 1996) a 21 assessing self-reported
depressive symptoms in the two weeks prior to baseline the measure received a Cronbach’s alpha
of .845 in our sample; and (g) the Hamilton Rating Scale for Depression (HRSD; Hamilton,
1960) a 21-item clinician-administered questionnaire assessing the severity of participants’
depressive symptoms in the week prior to the baseline, the measure received a Cronbach’s alpha
of .728 in our sample.
Follow-up. All participants were contacted approximately eight months (mean = 35.6
weeks; SD = 9.03) after their Time 1 assessment. They then filled out two online questionnaires:
Correlates and predictors of recurrent depression 11
the Events Scale (ES) and the Beck Depression Inventory, second edition (BDI-II). The ES was
measured the number of life events experienced since the Time 1 assessment and the perceived
valence of those events.
We then conducted phone interviews in which we asked participants about all events that
they had rated as negative on the ES and inquired about the onset and the duration of the event.
In contrast to previous studies assessing the time period of stressors (e.g., Kendler et al., 1999),
we did not merely look at the month of the stressor, but rather, we assessed the specific week so
that we could get a more accurate indication of when the stressor occurred in relation to
subsequent depressive symptoms. We then administered the mood, mania, and PTSD sections of
the SCID-I (First et al., 1996). Participants were compensated $10 for their time.
To assess participants’ depressive symptoms, we utilized the Depression Symptom
Rating (DSR) scale from the Longitudinal Interval Follow-up Evaluation (LIFE, Keller et al.,
1987). DSR scores are based on the number of depressive symptoms and the extent of
impairment, and can range from few or no depressive symptoms (DSR score of 1-2) to a full
diagnosis of a major depressive episode (DSR score of 5 or 6), thus providing an index of
depression that is both dimensional and categorical. Examining changes in DSR scores allowed
us to analyze weekly fluctuations in depressive symptoms and to better track the disorder in
participants. Subthreshold depressive episodes have been shown to be associated with increased
experience of prior and future MDEs (Sherbourne et al., 1994).
Results
What differentiates young adults who have and have not experienced a past major
depressive episode (MDE) from never depressed individuals? We conducted a multivariate
analysis of covariance (MANCOVA) using current depressive symptoms as the covariate.
Correlates and predictors of recurrent depression 12
Separate analyses were conducted for the measures of life events (negative, positive), abuse (e.g.,
physical, sexual, neglect), coping (e.g., primary, secondary, disengaged), and an ANCOVA on
dysfunctional attitudes.
The groups differed significantly on current depressive symptoms as measured by both
self-report and clinical interview (see Table 1). Controlling for current level of depressive
symptoms, previously depressed participants reported significantly lower total desirability scores
for both negative [F(1, 98) = 7.98, p = .006] and positive life events [F(1, 98) = 4.52, p = .036]
occurring in the previous 6 months. They also reported significantly lower levels of secondary
control coping, greater levels of involuntary engagement and involuntary disengagement coping,
and greater levels of childhood physical abuse compared to the never depressed controls. No
significant difference was found for dysfunctional attitudes [F(1, 98) = .98, p = .324]. However,
when not controlling for current depressive symptoms, previously depressed participants
reported significantly more dysfunctional attitudes than controls.
Follow-Up: Preliminary analyses. Of the 102 young adults assessed at baseline, 68
(67%) were reassessed at follow-up; 17 participants could not be located and 16 declined to
participate in the follow-up. Of the 102 follow-up participants, 32 (47%) had a prior history
depression at baseline; 43 (63%) were female. The mean age of this follow-up sample was 23.39
(SD = 3.88) and mean SES level was 54.05 (SD = 12.10). The mean number of weeks spent in
the study was 35.16 (SD = 9.03). By the end of the follow-up, 8 participants had experienced one
MDE and 1 participant had experienced two MDEs.
To address the hypotheses regarding within- and between-individual change
simultaneously, we specified a series of multilevel models using SAS PROC MIXED (SAS
Institute, 1996) consisting of a within-person (i.e., level-1) submodel describing how each
Correlates and predictors of recurrent depression 13
individual changed over time and a between-person (i.e., level-2) submodel describing how these
changes varied across individuals (see Bryk & Raudenbush, 1992; Singer & Willett, 2003).
Before fitting models including substantive predictors, we ran an unconditional means model
with no predictors to describe and partition the outcome variation across participants without
regard to time. This model stipulates that an individual’s DSR score at a given time point
deviates from their true mean by a level-1 residual, and that this true mean deviates from the
population average true mean by a level-2 residual. Results revealed that DSR scores had a nonzero intercept (B = 1.24, t = 21.11, p <.001), and that there was significant variation in DSR
scores within (B = .49, z = 34.12, p < .001) and between (B = .22, z = 5.43, p < .001) individuals.
The intraclass correlation coefficient indicated that 31% of the total variation in DSR scores
could be explained by differences between participants, suggesting empirical nesting of the data.
Next, we ran an unconditional growth model with time (a within-subject variable
indicating number of weeks in the study) as a predictor to determine whether there was
significant variation in DSR scores across both individuals and time. This model stipulates that
an individual’s DSR score at a given time point deviates from their true linear change trajectory
by a level-1 residual, and that this true linear trajectory deviates from the population average true
trajectory by a level-2 residual. Results revealed that the average trajectory for DSR scores
during the follow-up period had a significant positive slope (B = .001, t = 9.14, p < .001),
indicating that participants’ DSR scores increased over time. Moreover, there was significant
variation within individuals around their true change trajectories (B = .47, z = 34.11, p < .001) as
well as significant inter-individual variation in slopes (B = .22, t = 5.45, p < .001).
Taken together, these results point to nesting of the data and suggest that sufficient
heterogeneity exists to examine substantive level-1 and level-2 predictors. Ignoring individual
Correlates and predictors of recurrent depression 14
characteristics that contribute to response patterns over time as well as the effects of state
dependence would result in biased variability estimates and inflated Type I error rates. In this
situation, a multilevel analytic approach is warranted. All time-varying predictors were personcentered (i.e., the means of these variables equaled zero for each person) at Level 1 for this and
all subsequent analyses, This decision was made on both theoretical and statistical grounds
(Kreft, de Leeuw, & Aiken, 1995); this centering approach was intended to remove any betweenperson variance and prevent them from correlating with individual intercepts or between-person
factors (Schwartz & Stone, 1998). Including person-centered predictors allows the estimate of
the individual intercepts to be treated as a random effect by ensuring that the estimates of timevarying predictors represent purely within-person effects.
Preliminary analyses of covariates revealed risk (number of prior MDEs experienced
assessed at baseline) was significantly correlated with DSR scores (B = .04, t = 2.97, p = .004)
but not total stress levels. In addition, week significantly correlated with DSR scores (B = .001, t
= 9.14, p < .001) and total stress levels (B = .16, t = 19.62, p < .001). Sex, age, and SES were not
significantly correlated with DSR scores or total stress levels. All covariates were included in
subsequent analyses.
Is there a predictive relation between stress levels and depressive symptoms? The
specification of time-varying predictors such as lagged effects helps to clarify the temporal
ordering of events. To test whether and to what extent stress levels predicted subsequent
depressive symptoms, we ran a series of lagged effects models varying the lag interval n. The
full model was as follows:
Dep ti 00 10 Dep (t n )i 20 Stress (t n )i u 0i rti
Correlates and predictors of recurrent depression 15
In this equation, the term Dep denotes an individual’s DSR score and Stress denotes that
individual’s total level of stress. Thus, Depti indicates the DSR score at time t for person i. Terms
with subscript (t - n) were effects of the nth week prior to Depti. To protect against Type I error,
we only interpreted results if they were significant at the p < .01 level.
Results indicated that the optimal lag (i.e., strongest predictive association) between total
stress level and depressive symptoms was seven weeks. At this interval, the effect of stress levels
on depressive symptoms was estimated as 0.03 (p < .001). Stress remained a significant predictor
of higher levels of DSR scores up to a lag of 14 weeks (see Figure 1). For all subsequent
analyses, Level 1 predictors (i.e., stress and DSR scores) were lagged 7 weeks behind the
dependent variable (i.e. DSR scores).
Predictors of DSR scores. Multilevel modeling was used to assess the predictive ability
of each of the variables. We examined each of the key predictors on change in DSR scores over
the follow up, controlling for the following covariates [i.e., sex, age, SES, prior MDEs, total
stress levels (lagged at 7 weeks), DSR scores (lagged at 7 weeks)]. Theses analyses, therefore,
are testing whether the key predictors (e.g., dysfunctional attitudes, coping, trauma) moderated
the rate of change in DSR scores over the follow-up period. The key predictors also were
included as moderators of the relation between DSR scores and stress levels (lagged 7-weeks).
Dysfunctional attitudes significantly predicted DSR trajectories B = .0004, t(1858) =
5.89, p < .0001; that is, DSR scores increased at a faster rate at higher levels of dysfunctional
attitudes. Dysfunctional attitudes also significantly moderated the relation between DSR scores
and stress levels 7-week prior, B = .001, t (1858) = 4.24, p < .0001.
Coping predicted the slope of depressive symptoms. Secondary control coping negatively
predicted change in depressive symptoms [B = -0. 21, t(1858) = -6.46, p = .0001], whereas
Correlates and predictors of recurrent depression 16
voluntary disengagement coping, [B = .26, t (1858) = 4.08, p < .001], involuntary engagement
coping [B = .14, t(1858) = 3.62, p = .0003], and involuntary disengagement coping [B = .02,
t(1858) = 3.92, p < .0001] predicted faster rates of change in depressive symptoms during the
follow-up, above and beyond the covariates. Primary control coping did not significantly predict
DSR scores after including the covariates.
Secondary control coping and involuntary disengagement coping also moderated the
relation between total stress levels and DSR scores 7 weeks later. The relation between stress and
depressive symptoms was weaker at higher levels of secondary control coping [B = -.41, t (1858)
= -4.74, p < .0001]. In contrast, the relation between stress and depressive symptoms was
stronger (i.e., more positive) at higher levels of involuntary disengagement coping [B = .77, t
(1858) = 5.84, p < .0001].
With regard to early childhood maltreatment, none of the trauma subscales showed a
significant direct association with changes in DSR scores after including covariates. We next
examined whether early maltreatment moderated the relation between total stress levels and DSR
scores 7 weeks later; these analyses examined whether childhood trauma functioned as a
relatively stable vulnerability factor that predicted depressive symptoms when triggered by
ongoing life stress. The Emotional Abuse X Stress Level interaction significantly predicted DSR
scores, B = .01, t (1834) = 7.37, p < .0001. That is, the relation between stress and depressive
symptoms 7-weeks later was stronger (i.e., more positive) at higher levels of emotional abuse.
This interaction is depicted in Figure 2. Simple slope analyses revealed that higher stress levels
were associated with higher DSR scores for participants who reported more emotional abuse
during childhood (B = .06, t = 9.40, p < .0001). For those who reported low emotional abuse
during childhood, the relation of stress levels to DSR scores was not significant.
Correlates and predictors of recurrent depression 17
We next examined whether the Stress X Week interaction significantly predicted DSR
scores as a function of different types of maltreatment. The Stress X Week X Emotional Abuse
interaction was significant. Simple slope analyses revealed that the Stress X Week interaction
was significant for both higher [B = .003, t(1832) = 4.06, p < .0001] and lower levels of
emotional abuse [B = -.003, t(1832) = -5.36, p < .0001]. Among individuals with greater
emotional abuse, higher stress levels were associated with increases in DSR scores over time [B
= .02, t(1832) = 5.71, p < .0001]; lower stress levels were not associated with change in DSR
scores over time. Among individuals who experienced less emotional abuse, lower stress levels
were associated with change in DSR scores over time [B = .02, t(1832) = 6.54, p < .0001],
whereas higher stress levels were not associated with change in DSR scores (see Figure 3).
The Stress X Week X Emotional Neglect interaction also was significant. Simple slope
analyses revealed that the Stress X Week interaction was significant at lower levels of emotional
neglect [B = -.002, t(1832) = -4.12, p < .0001], but not at higher levels of emotional neglect (see
Figure 4). Among individuals with higher levels of emotional neglect, both higher [B = .01,
t(1832) = 2.80, p = .005] and lower stress levels (B = .02, t(1832) = 4.83, p < .0001) were
associated with increases in DSR scores over time. Among individuals with lower levels of
emotional neglect, lower stress levels were associated with increases in DSR scores over time (B
= .02, t(1832) = 4.92, p < .0001), whereas higher stress levels were not associated with change in
DSR scores over time.
Finally, we found a significant Stress X Week X Sexual Abuse interaction. The Stress X
Week interaction was significant at higher levels of sexual abuse [B = -.002, t(1832) = -5.01, p <
.0001], but not at lower levels of sexual abuse. Among individuals with a history of more sexual
abuse, both higher [B = .01, t(1832) = 2.61, p = .009] and lower stress levels [B = .03, t(1832) =
Correlates and predictors of recurrent depression 18
7.77, p < .0001] were associated with increases in DSR scores over time. Among individuals
with a history of less sexual abuse, neither lower nor higher stress levels were associated with
increases in DSR scores over time. This interaction is depicted in Figure 5.
Discussion
Several interesting findings emerged regarding correlates and predictors of depression in
young adults. The first aim of this study was to examine what differentiated people with and
without a history of mood problems. We found that individuals who had previously experienced
a major depressive episode (MDE) reported a higher incidence of early physical abuse, more
recent stress, and more maladaptive coping styles. Other studies similarly have shown that
individuals with a history of abuse are more vulnerable to depression than those in the general
population (e.g., Harkness et al., 2006). Additionally, previously depressed individuals rated life
events as more negative and less positive than never-depressed controls. This finding is
consistent with the notion that previously depressed individual perceive events more negatively
than do others, suggesting that stressors may pose a greater threat for those individuals.
With regard to coping responses to stress, previously depressed individuals also reported
significantly higher levels of involuntary engagement and involuntary disengagement responses
to stress and lower levels of primary control coping. These results are consistent with the
findings of Compas and colleagues (2001) that primary control coping was correlated with lower
levels of internalizing symptoms, whereas disengagement coping strategies (e.g., avoidance or
withdrawal) were associated with higher levels of internalizing symptoms.
Regarding dysfunctional attitudes, individuals with a prior history of depression had
significantly higher scores on the DAS compared to never depressed controls, although this
difference was no longer significant when current level of depressive symptoms were controlled.
Correlates and predictors of recurrent depression 19
Thus, the residual depressive symptoms of those with a history of depression may serve to
maintain dysfunctional attitudes even when they are not experiencing a full depressive episode.
Although some studies have shown that residual depressive symptoms are linked with more
negative cognitions even after the depressive episode has remitted, other studies have found that
the attitudes and beliefs of these individuals return to “normal” between episodes (Abela &
Hankin, 2008). The current results are more consistent with the view that in formerly depressed
individuals, levels of residual depressive symptoms are associated with levels of dysfunctional
attitudes. The direction of this relation, however, cannot be determined from these crosssectional analyses.
Predicting Depressive Symptoms
The second purpose of this study was to explore predictors of depressive symptoms
during a six to eight month follow-up. Results indicated that risk, defined by the number of prior
MDEs experienced before the baseline assessment, predicted subsequent depressive symptom
rating (DSR) scores. This finding is consistent with other studies showing that depression is a
recurrent disorder (e.g., Harkness et al., 1999; Kendler et al., 1998; Monroe & Harkness, 2005).
We then examined the predictive relation between total stress levels and depressive
symptoms using lagged effects models. Following the method used by Morris et al. (2010), we
did not make assumptions about the time period in which stress would have the strongest relation
to DSR scores. Rather, we explored at which time period the association between stress and
depressive symptoms was strongest, and found that the prediction of depressive symptoms from
total stress levels was strongest at seven weeks, and continued to predict DSR scores for up to 14
weeks. In addition, week significantly correlated with DSR scores and total stress levels.
Correlates and predictors of recurrent depression 20
These timing results differed somewhat from those of Morris et al. (2010) who found that
the predictive relation between stress and depressive symptoms peaked ta two weeks and
remained significant for up to 26 weeks. This difference may be due to the methods used to
assess life events. Whereas Morris and colleagues used a Life Events Interview and assessed
events occurring during the previous year, the present study used a self-report checklist, which
assessed events occurring between Time 1 and the follow-up evaluation, which was about 35
weeks, or about 8 months after the initial assessment. Whereas the relatively shorter time period
in the current study may have allowed for better memory and dating of events, the interview
method used by Morris et al. was based on the composite memory of two people (i.e.,
adolescent, mother) for recalling stressors and their time periods. Additionally, time, specified by
one-week intervals, significantly predicted DSR scores and total stress levels, although it is
possible that this correlation was partially due to memory of participants for the time closest to
the interview.
Next, we examined whether variables assessed at Time 1 predicted depressive symptoms
over the follow-up period. Consistent with the literature (e.g., Abela & Hankin, 2008), we found
that high levels of dysfunctional attitudes significantly predicted a faster increase in DSR scores.
Moreover, dysfunctional attitudes moderated the relation between DSR scores and stress levels,
such that the relation between stress and depression was stronger at higher levels of
dysfunctional attitudes. Given that dysfunctional attitudes were present both at the baseline and
follow-up, however, it is not possible to determine the direction of this relation; that is, we do not
know if dysfunctional attitudes preceded the first episode or if they resulted from a “scar” from
the prior episode (Zeiss & Lewinsohn, 1987). Nevertheless, the presence of these dysfunctional
attitudes predicted DSR scores over time.
Correlates and predictors of recurrent depression 21
Additionally, the coping subscales significantly predicted change in DSR scores in the
expected direction. Consistent with Compas et al. (2001), secondary control coping predicted a
decrease in depressive symptoms over time. In contrast, involuntary engagement and
disengagement strategies significantly predicted faster rates of change (i.e., growth) in DSR
scores. Furthermore, secondary control coping and involuntary disengagement coping both
acted as moderators of the relation between total stress and depressive symptoms. At higher
levels of secondary control coping, the relation between stress and depression was weaker,
whereas at higher levels of involuntary disengagement, the relation between stress and
depression was stronger.
With regard to history of maltreatment, no main effects of childhood abuse predicted
subsequent depressive symptoms, but the interaction of emotional abuse and recent stressful
events significantly predicted DSR scores. That is, the relation between stress and depression
was significant for those with a history of emotional abuse, but not for those without an
emotional abuse history. Thus, consistent with Harkness and colleagues (2006), we found that
some forms of early childhood maltreatment were related to subsequent depressive symptoms
Finally, we found that the interactions of stress and week on DSR scores were
significantly moderated by different types of abuse. Among children who had experienced high
levels of emotional abuse, high levels of stress predicted change in DSR score over time. In
contrast, among those with less emotional abuse, only lower levels of stress were associated with
increases in DSR scores over time. Second, our findings show that among those experiencing
high levels of emotional neglect, both high and low levels of stress predicted increases in DSR
scores over time. However, among those with lower levels of emotional neglect, only lower
stress levels were associated with increases in DSR scores over time, whereas higher stress levels
Correlates and predictors of recurrent depression 22
were not associated with change. Third, the stress by week interaction significantly predicted
increases in DSR scores over time at both high and low levels of stress among those with high
levels of sexual abuse; yet, among those with lower levels of sexual abuse, neither lower nor
higher stress levels were associated with increases in DSR scores over time. Thus, consistent
with Harkness and colleague (2006), we found that some forms of early childhood maltreatment
were related to depressive symptoms as young adults. It appears that experiencing abuse may
differentially affect the experience of both high and low levels of stress, having different
consequences for future depressive symptoms.
The current study contributed to the literature on recurrent depression in a several ways.
First, we affirmed previous research noting the association between depression, dysfunctional
attitudes, stressful life events, maladaptive coping styles, and history of abuse. We also noted
the role of stress, dysfunctional attitudes, involuntary engagement coping, involuntary
disengagement coping, and the interaction of emotional abuse and stress in predicting subsequent
depressive symptoms. Although previous studies have examined the relation of these variables
to depressive symptoms, the current prospective study highlighted their predictive value, and
possible points for intervention.
Limitations of the current study provide directions fur future research. First, the time
frame between completion of the self-report measures and the interview was not always
consistent across participants. Second, although participants knew that they had experienced
certain stressors, some were uncertain of the exact start or duration of the event, resulting in their
guessing or choosing an arbitrary date. Future studies might have participants keep a daily or
weekly diary to record the stressors they encounter, and to rate how negative those stressors are
(Liu & Aloy, 2010).
Correlates and predictors of recurrent depression 23
Third, life events checklists tend to be less informative than stress interviews regarding
the onset and offset of events (Hammen et al., 2005). The use of these scales limits our ability to
thoroughly assess important aspects of stressful events including the type of events,
dependence/independence of the events, acute versus chronic, major versus minor, and the
objective impact of the event on participants. Therefore, future studies of stress and recurrent
depression should consider using life events interviews rather than or in addition to checklists.
Fourth, the current prospective study examined subthreshold levels of depressive
symptoms. This allowed us to better examine the full continuum of depression over time. A
larger sample is needed, however, to investigate predictors of onsets of recurrent depressive
episodes.
Finally, clinical implications of this study should be mentioned. To detect individuals
who are at risk for recurrent depression, clinicians should assess their history of maltreatment,
current coping style, and levels and types of stress. Once identified, then interventions can be
implemented that directly treat an individual’s specific vulnerabilities and prevent the
development of full depressive episodes
Correlates and predictors of recurrent depression 24
References
Abela, J. R. Z. & Hankin, B. L. (2007). Cognitive vulnerability to depression in children and
adolescents: A developmental psychopathology perspective. In J. Abela & B. Hankin
(Eds.), Handbook of depression in children and adolescents, (pp. 35-78). NY: Guilford.
Beck, A. T. (2008). The evolution of the cognitive model of depression and its neurobiological
correlates. American Journal of Psychiatry, 165, 969-977.
Beck, A.T., Steer, R.A., & Brown, G.K. (1996). Manual for the Beck Depression Inventory-II.
San Antonio, TX: Psychological Corporation.
Bylsma, L. M., Morris, B. H., Rottenberg, J. (2007). A meta-analysis of emotional reactivity in
major depressive disorder. Clinical Psychology Review, 28, 676-691.
Bryk, A. S., & Raudenbush, S. W. (1992). Hierarchical linear models: Applications and data
analysis methods. Thousand Oaks, CA: Sage
Burcusa, S. L & Iacono, W. G. (2007). Risk for recurrence in depression. Clinical Psychology
Review, 27, 959-985.
Compas, B. E, Connor-Smith, J. K., Saltzman, H., Thomsen, A. H. Wadsworth, M. E. (2001).
Coping with stress during childhood and adolescence: Problems, progress and potential in
theory and research. Psychological Bulletin, 127, 87-127.
Compas, B.E., Davis, G.E., Forsythe, C.J., & Wagner, B.M. (1987). Assessment of major and
daily stressful events during adolescence: The adolescent perceived events scale. Journal
of Consulting and Clinical Psychology, 55, 534-541.
Connor-Smith, J. K., Compas, B. E., Wadsworth, M. E., Thomsen, A. H., & Saltzman, H.
(2000). Responses to stress in adolescence: Measurement of coping and involuntary stress
responses. Journal of Consulting and Clinical Psychology, 68, 976–992
Correlates and predictors of recurrent depression 25
First, M.B., Spitzer, R.L., Gibbon, M., & Williams, J.B.W. (1997). User’s guide for the
Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) - Clinician Version.
Washington, DC: American Psychiatric Press.
Hamilton, M. (1960). A rating scale for depression. Journal of Neurology, Neurosurgery, and
Psychiatry, 23, 56-62.
Hankin, B. L., & Abramson, L. (2001). Development of gender differences in depression: An
elaborated cognitive vulnerability-transactional stress theory. Psychological Bulletin, 127,
773–796.
Harkness, K. L., Bruce, A. E. & Lumley, M. N. (2006). The role of childhood abuse and neglect
in the sensitization to stressful life events in adolescent depression. Journal of abnormal
psychology, 115, 4, 730-741.
Harkness KL, Monroe SM, Simons AD, Thase M. (1999). The generation of life events in
recurrent and non-recurrent depression. Psychological Medicine, 29, 135–44.
Kendler, K. S., Karkowski, L. M., & Prescott, C. A. (1999). Causal relationship between
stressful life events and the onset of major depression. American Journal of Psychiatry,
156, 837–841.
Kendler, K., Karkowski, L. M., & Prescott, C. (1998). Stressful life events and major depression:
Risk period, long-term contextual threat, and diagnostic specificity. Journal of Nervous
and Mental Disorders, 186, 661– 669.
Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. (1993). The Trier Social Stress Test: A tool
for investigating psychobiological stress responses in a laboratory setting.
Neuropsychology, 28, 76-81.
Kreft, I. G. G., Jan de Leeuw, J., & Aiken, L. S. (1995). The effect of different forms of
Correlates and predictors of recurrent depression 26
centering in hierarchical linear models. Multivariate Behavioral Research, 30, 1–21.
Liu, R.T., & Alloy, L.B. (2010) Stress generation in depression: A systematic review of the
empirical literature and recommendations for future study. Clinical Psychology Review,
30, 582–593
Marschall, D.E., Sanftner, J., & Tangney, J.P. (1994). State Shame and Guilt Scale. Fairfax, VA:
George Mason University.
Monroe, S. M. & Harkness, K. L. (2005). Life stress, the “kindling” hypothesis, and the
recurrence of depression: Considerations from a life stress perspective. Psychological
Review, 112, 417-445.
Morris, B. H., Bylsma, L. M., and Rottenberg, J. (2009). Does emotion predict the course of
major depressive disorder? A review of prospective studies. British Journal of Clinical
Psychology, 48, 255-273.
Morris, M.C., Ciesla, J.A., & Garber, J. (2010). A prospective study of stress autonomy versus
stress sensitization in adolescents at varied risk for depression, Journal of Abnormal
Psychology, 119, 341-354.
Nolen-Hoeksema, S. (2000). The role of rumination in depressive disorders and mixed
anxiety/depressive symptoms. Journal of Abnormal Psychology, 109, 504–511.
Rusting, C. L., & Larsen, R. J. (1997). Extraversion, neuroticism, and susceptibility to positive
and negative affect: A test of two theoretical models. Personality and Individual
Differences, 22, 607-612.
Schwartz, J. E., & Stone, A. A. (1998). Strategies for analyzing ecological momentary
assessment data. Health Psychology, 17, 6–16.
Scott, J., Williams, J. M. G., Brittlebank, A., and Ferrier, N. (1995). The relationship between
Correlates and predictors of recurrent depression 27
premorbid neuroticism, cognitive dysfunction and persistence of depression: a 1-year
follow-up. Journal of Affective Disorders, 33, 167-172.
Sherbourne, C. D., Wells, K. B., Hays, R. D., Rogers, W., Burnam, M. A., & Judd, L. L. (1994).
Subthreshold depression and depressive disorder: Clinical characteristics of general
medical and mental healthy specialty outpatients. American Journal of Psychiatry, 151,
1777–1784.
Singer, J. D., & Willett, J. B. (2003). Applied longitudinal data analysis: Modeling change and
event occurrence. New York, NY: Oxford University Press.
Stroud, C. B., Davila, J., & Moyer, A. (2008). The relationship between stress and depression in
first onsets versus recurrences: A meta-analytic review Journal of Abnormal Psychology,
117, 206–213.
Watson, D., Clark, L. A., & Tellegen, A. (1988). Development and validation of brief measures
of positive and negative affect: The PANAS scales. Journal of Personality and Social
Psychology, 54, 1063-1070.
Weissman, A., & Beck, A. T. (1978, November). Development and validation of the
Dysfunctional Attitudes Scale: A preliminary analysis. Paper presented at the annual
meeting of the American Educational Research Association, Toronto, Ontario, Canada.
Zeiss, A. M., and Lewinsohn, P. M. (1987). Enduring deficits after remissions of depression: A
test of the scar hypothesis. Behavior Research and Therapy, 26 (2) 151-158.
Zobel, A. W., Nickel, T., Sonntag, A., Uhr, M., Holsboer, F., & Ising, M. (2001). Cortisol
response in the combined dexamethasone/CRH test as predictor of relapse in patients with
remitted depression: A prospective study. Journal of Psychiatric Research, 35, 83-94.
Correlates and predictors of recurrent depression 28
Table 1. Means and standard deviations of study variables of individuals with a prior major
depressive episode (MDE) and those who were never depressed
Prior Depression
Never Depressed
M (SD)
M (SD)
F
Beck Depression Inventory
8.23 (5.94)
3.22 (3.32)
6.05*
Hamilton Depression Rating Scale
5.86 (4.24)
2.22 (2.35)
24.49***
M (SD)
M (SD)
Fa
Negative Events
-36.64 (17.84)
-23.89 (13.02)
7.98**
Positive Events
57.65 (15.13)
66.76 (20.40)
4.52*
Primary Control
.20 (.04)
.22 (.04)
7.36**
Secondary Control
.23 (.06)
.27 (.04)
3.76~
Voluntary Disengagement
.14 (.03)
.13 (.02)
.62
Involuntary Engagement
.27 (.05)
.23 (.04)
6.78*
Involuntary Disengagement
.17 (.03)
.15 (.03)
5.09*
Physical Abuse
6.38 (2.29)
5.59 (1.09)
6.79*
Sexual Abuse
5.50 (1.55)
5.41 (2.24)
.47
Emotional Abuse
7.87 (4.03)
7.15 (2.15)
.51
Emotional Neglect
7.64 (3.08)
7.41 (2.83)
.05
Physical Neglect
5.95 (1.74)
5.65 (1.29)
1.37
131.47 (27.63)
117.91 (22.99)
.98
Life Events Desirability Scores
Responses to Stress (Coping)
History of Maltreatment
Dysfunctional Attitudes
~p < .10; *p < .05; **p < .01; ***p < .001;
a
Results of ANCOVAs with depressive symptoms as the covariate.
Correlates and predictors of recurrent depression 29
Variable
1
2
3
4
5
6
7
8
1. MDD Hx
2. Sex
.14
3. Age
.08
-.02
4. SES
.14
.13
-.21
5. BDI-II
.46***
.07
.01
-.05
6. HRSD
7. Primary
Control
8. Secondary
Control
9. Disengage
.46***
.19
-.08
.01
.70***
-.32***
.14
-.12
.03
-.44***
-.20*
-.39***
-.07
.03
-.004
-.59***
-.52***
.36***
-.09
.08
.13
.29**
-0.001
-.56***
-.26*
.07
9
10
11
12
13
14
15
16
17
18
10. Invol Eng
.43***
.09
.003
-.01
.50***
.51***
-.47***
-.84***
.02
11. Invol
Disengage
.35***
-.12
0.02
-.12
.56***
.35***
-.70***
-.65***
.29**
.49***
12. Emotion
Abuse
.11
0.04
0.18
.02
.20*
.10
-.03
-.26**
.19
.14
.11
13. Physical
Abuse
.21*
.01
-.14
.07
.03
-.03
.45***
-.19
.08
.16
.01
.45**
14. Sexual
Abuse
.02
.10
.05
.02
.04
.18
-0.03
.13
-.07
-.13
.12
-.11
-.03
15. Emotion
Neglect
.04
.03
-.12
.14
.04
.12
.59***
.42***
.17
.11
.04
.59***
.42***
0.17
16. Physical
Neglect
.10
.04
-.23*
.05
.00
-.02
.52***
.60***
.20*
.55***
-.09
.52***
.60***
.20*
.55***
.26**
-.07
-.29**
.18
-.23*
.58***
- .38***
-.60***
.34***
.49***
.46***
.36***
.20*
-.03
.23*
.13
18. Negative
Events
-.45***
-.06
.03
.02
-.56***
-.51***
.44***
.58***
-.18
-.57***
-.50***
-.18
-.04
-.18
-.26*
-.16
-.47***
19. Positive
Events
-.25*
.06
-.27**
.06
-.24*
-0.14
.28**
.32**
-.35***
-.18
-.34**
-.02
.03
-.03
-.05
.11
-.21*
.11
Mean
0.55
0.64
22.97
54.89
5.97
4.22
0.21
0.25
0.14
0.25
0.16
4.22
7.54
6.02
5.46
7.53
-32.47
61.8
S.D.
0.50
0.48
3.87
11.24
5.51
3.94
0.04
0.05
0.03
0.05
0.03
3.94
3.31
1.88
1.89
2.95
17.61
18.21
17. DAS
MDD = Major Depressive Disorder; SES = Socioeconomic Status; Beck Depression Inventory; HRSD = Hamilton Rating Scale for
Depression; Invol = Involuntary; Eng or Engage = Engagement; Disengage = Disengagement; Emotion = Emotional; DAS = Dysfunctional
Attitudes Scale; S.D. = Standard Deviation
Correlates and predictors of recurrent depression 30
Table 3. Dysfunctional attitudes significantly predicted (p < .05) DSR scores over the follow-up,
controlling for covariates [sex, age, SES, week, Prior MDEs, total stress levels (lagged 7
weeks), DSR scores (lagged 7 weeks)].
Predictors
B (SE)
Intercept
1.30 (.63)*
Sex
.13 (.12)
Age
.02 (.02)
SES
-.01 (.01)
Week
-.04 (.01)***
Prior MDEs
.03 (.01)*
Prior Stress
-.06 (.02)**
Prior Depression
-.14 (.03)***
Dysfunctional Attitudes
-.003 (.002)
Week X Dysfunctional Attitudes
.0004 (.00)***
Prior Stress X Dysfunctional Attitudes
.0006 (.0001)***
*p < .05; ** p < .01; ***p< .001.
Note: Intercept represents DSR score at Week 0 (i.e., week before follow-up period) when all
covariates are equal to zero.
Correlates and predictors of recurrent depression 31
Table 4. Secondary control coping significantly (p<.05) predicted DSR scores over the followup, controlling for covariates [sex, age, SES, week, prior MDEs, total stress levels (lagged 7
weeks), DSR scores (lagged 7 weeks)].
Predictors
B (SE)
Intercept
.67 (.62)
Sex
.10 (.12)
Age
.10 (.02)
SES
-.01 (.01)
Week
.10 (.01)***
Prior MDEs
.03 (.01)~
Prior Stress
.11 (.02)***
Prior Depression
-.14 (.03)**
Secondary Control
2.05 (1.37)
Week X Secondary Control
-.20 (.03)***
Prior Stress X Secondary Control
-.41 (.09)***
~p < .10; *p < .05; ** p < .01; ***p< .001
Note: Intercept represents DSR score at Week 0 (i.e., week before follow-up period) when all
covariates are equal to zero.
Correlates and predictors of recurrent depression 32
Table 5: Involuntary engagement coping significantly (p<.05) predicted DSR scores over the
follow-up, controlling for covariates [sex, age, SES, week, prior MDEs, total stress levels
(lagged 7 weeks), DSR scores (lagged 7 weeks)].
Predictors
B (SE)
Intercept
1.22 (.63)~
Sex
.09 (.12)
Age
.004 (.02)
SES
-.01 (.01)
Week
-.02 (.009)*
Prior MDEs
.03 (.01)*
Prior Stress
.003(.03)
Prior Depression
-.10 (.03)***
Involuntary Engagement
.002 (1.56)
Week X Involuntary Engagement
.14 (.04)***
Stress X Involuntary Engagement
.07 (.09)
~p < .10; *p < .05; ** p < .01; ***p< .001
Note: Intercept represents DSR score at Week 0 (i.e., week before follow-up period) when all
covariates are equal to zero.
Correlates and predictors of recurrent depression 33
Table 6. Involuntary disengagement significantly (p<.05) predicted DSR scores over the followup, controlling for covariates [sex, age, SES, week, prior MDEs, total stress levels (lagged 7
weeks), DSR scores (lagged 7 weeks)].
Predictors
B (SE)
Intercept
1.23 (.61)*
Sex
.11 (.13)
Age
.001 (.02)
SES
-.005 (.01)
Week
-.02 (.01)*
Prior MDEs
.03 (.01)~
Prior Stress
-.11 (.02)***
Prior Depression
-.14 (.03)***
Involuntary Disengagement
-.40 (2.22)
Week X Involuntary Disengagement
.21 (.05)***
Prior Stress X Involuntary Disengagement
.77 (.14)***
~p < .10; *p < .05; ** p < .01; ***p< .001
Note: Intercept represents DSR score at Week 0 (i.e., week before follow-up period) when all
covariates are equal to zero.
Correlates and predictors of recurrent depression 34
Table 7. Emotional Abuse X Prior Stress significantly (p<.001) predicted DSR scores over the
follow-up, controlling for covariates [sex, age, SES, week, prior MDEs, total stress levels
(lagged 7 weeks), DSR scores (lagged 7 weeks)].
Predictors
B (SE)
Intercept
1.06 (.57)~
Sex
.11 (.13)
Age
.01 (.02)
SES
-.01 (.01)
Week
.01 (.00)~
Prior MDEs
.03 (.01)*
Prior Stress
-.06 (.01)***
Prior Depression
-.14 (.03)***
Emotional Abuse
-.01 (.03)
Week X Emotional Abuse
.00 (.00)
Prior Stress X Emotional Abuse
.01 (.00)***
~p < .10; *p < .05; ** p < .01; ***p< .001.
Correlates and predictors of recurrent depression 35
Lagged Effects of Stress on Depression
Relation of Stress to
Depression(B)
0.04
0.035
0.03
0.025
0.02
0.015
0.01
0.005
0
1
3
5
7
9
11
13
15
Weeks (lagged)
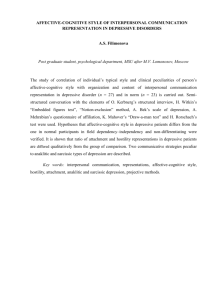
Figure 1. The strongest predictive association between total stress level and depressive
symptoms was seven weeks. At this interval, the effect of stress levels on depressive symptoms
was estimated as 0.03 (p < .001). Stress remained a significant predictor of increases in DSR
scores up to a lag of 14 weeks
Correlates and predictors of recurrent depression 36
Figure 2
Depression Symptom Ratings (DSR)
3
2 .5
2
High Emotional
Abuse
1 .5
***
1
0 .5
0
Low
High
Stress Level
Low Emotional Abuse
Correlates and predictors of recurrent depression 37
Figure 3. Emotional Abuse X Prior Stress X Week interaction
High Emotional Abuse
Depression Symptom Ratings (DSR)
3
***
2.5
2
High Stress
1.5
Low Stress
1
0.5
0
Weeks
Low Emotional Abuse
Depression Symptom Ratings (DSR)
3
2.5
***
High Stress
2
Low Stress
1.5
1
0.5
0
Weeks
Correlates and predictors of recurrent depression 38
Figure 4. Emotional Neglect X Prior Stress x Week interaction:
High Emotional Neglect
Depression Symptom Ratings (DSR)
3
2.5
High Stress
**
2
Low Stress
***
1.5
1
0.5
0
Weeks
Low Emotional Neglect
Depression Symptom Ratings (DSR)
3
2.5
***
2
High Stress
Low Stress
1.5
1
0.5
0
Weeks
Correlates and predictors of recurrent depression 39
Figure 5. Sexual Abuse X Prior Stress x Week interaction:
High Sexual Abuse
Depression Symptom Ratings (DSR)
3
2.5
2
***
High Stress
**
Low Stress
1.5
1
0.5
0
Weeks
Low Sexual Abuse
Depression Symptom Ratings (DSR)
3
2.5
High Stress
2
Low Stress
1.5
1
0.5
0
Weeks