Supplementary Material tumors: Clinical correlations in a single-centre patient cohort CDC73
advertisement

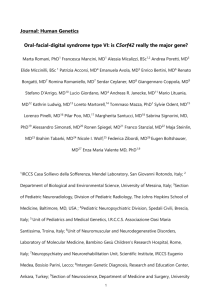
Supplementary Material CDC73 mutations and parafibromin immunohistochemistry in parathyroid tumors: Clinical correlations in a single-centre patient cohort Vito Guarnieri, Claudia Battista, Lucia Anna Muscarella, Michele Bisceglia, Danilo de Martino, Filomena Baorda, Evaristo Maiello, Leonardo D’Agruma, Iacopo Chiodini, Celeste Clemente, Salvatore Minisola, Elisabetta Romagnoli, Sabrina Corbetta, Raffaella Viti, Cristina Eller-Vainicher, Anna Spada, Michela Iacobellis, Nazzarena Malavolta, Massimo Carella, Lucie Canaff, Geoffrey N. Hendy, David E.C. Cole, Alfredo Scillitani Correspondence: Alfredo Scillitani, Endocrinology Unit, Ospedale “Casa Sollievo della Sofferenza”, Istituto di Ricovero e Cura a Carattere Scientifico, 71013 San Giovanni Rotondo (Foggia), Italy email: alscill@tin.it Tel: ++390882410625; Fax: ++390882410627 Supplementary Fig. 1 Analysis of allelic imbalance (loss of heterozygosity or LOH) at the CDC73 locus. Shown at the top is a physical map of the locus at 1p31.2, and location of LOH markers. Supplementary Methods LOH analysis was performed using the following markers flanking CDC73 [S1-S3]: D1S428, D1S412, D1S413, D1S2840 and D1S2794, as well as one intragenic intron 10 marker [S4]. PCR was performed in a 50 L reaction volume containing 5 L 10X PCR Buffer (Eppendorf), 0.25 nM dNTPs, 20 pmol of each primer, 1 U HotMaster Taq (Eppendorf) and 100 ng of DNA. Cycling conditions consisted of 40 cycles of the LMS2 (ABI Prism Linkage Mapping Set version 2) method performed on a GeneAmp PCR System 9700 (Applied Biosystems, Foster City, CA) for all markers. After capillary array electrophoresis and data reduction (ABI GeneScan and Genotyper Software 3.7 NT, Applied Biosystems, Foster City, CA), LOH was determined by allelic imbalance (AI) scoring. The AI was quantitated using the formula: (peak 1 height/peak2 height in tumour DNA)/(peak 1 height/peak 2 height in normal DNA), which is a more conservative criterion than sometimes suggested [S5]. LOH was assigned if the AI was 0.5 or less, while an AI between 0.5 and 0.65 was defined as borderline. ROH = Retention of Heterozygosity; NI = not informative. Supplementary References S1. J.D. Carpten, C.M. Robbins, A. Villablanca, L. Forsberg, S. Presciuttini, J. Bailey-Wilson, W.F. Simonds, E.M. Gillanders, A.M. Kennedy, J.D. Chen, S.K. Agarwal, R. Sood, M.P. Jones, T.Y. Moses, C. Haven, D. Petillo, P.D. Leotlela, B. Harding, D. Cameron, A.A. Pannett, A. Höög, H. Heath 3rd, L.A. James-Newton, B. Robinson, R.J. Zarbo, B.M. Cavaco, W. Wassif, N.D. Perrier, I.B. Rosen, U. Kristoffersson, P.D. Turnpenny, L.O. Farnebo, G.M. Besser, C.E. Jackson, H. Morreau, J.M. Trent, R.V. Thakker, S.J. Marx, B.T. Teh, C. Larsson, M.R. Hobbs, HRPT2, encoding parafibromin, is mutated in hyperparathyroidism-jaw tumor syndrome. Nature Genet 32, 676-80 (2002) S2. V.M. Howell, C.J. Haven, K. Kahnoski, S.K. Khoo, D. Petillo, J. Chen, G.J. Fleuren, B.G. Robinson, L.W. Delbridge, J. Philips, A.E. Nelson, U. Krause, K. Hammje, H. Dralle, C. HoangVu, O. Gimm, D.J. Marsh, H. Morreau, B.T. Teh, HRPT2 mutations are associated with malignancy in sporadic parathyroid tumours. J Med Genet 40, 657-63 (2003) S3. F. Cetani, E. Pardi, S. Borsari, P. Viacava, G. Dipollina, L. Cianferotti, E. Ambrogini, E. Gazzerro, G. Colussi, P. Berti, P. Miccoli, A. Pinchera, C. Marcocci, Genetic analysis of the HRPT2 gene in primary hyperparathyroidism: germline and somatic mutations in familial and sporadic parathyroid tumors. J Clin Endocrinol Metab 89, 5583-91 (2004) S4. T.M. Shattuck, S. Valimäki, T. Obara, R.D. Gaz, O.H. Clark, D. Shoback, M.E. Wierman, K. Tojo, C.M. Robbins, J.D. Carpten, L.O. Farnebo, C. Larsson, A. Arnold, Somatic and germ-line mutations of the HRPT2 gene in sporadic parathyroid carcinoma. N Engl J Med 349, 1722-29 (2003) S5. R.I. Skotheim, C.B. Diep, S.M. Kraggerud, K.S. Jakobsen, R.A. Lothe, Evaluation of loss of heterozygosity/allelic imbalance scoring in tumor DNA. Cancer Genet Cytogenet 127, 64-70 (2001)