HEV flowchart for Clinicians - Final.ppt
advertisement

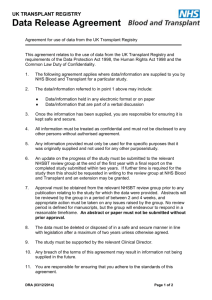
Clinical guidance for use of Hepatitis E virus (HEV) negative blood components HEV negative blood components are indicated in: • Patients awaiting solid organ transplant (SOT) – from 3 months prior to date of planned elective SOT or from the date of listing for a solid organ transplant. • Patients who have had SOT – for as long as the patient is taking immunosuppressants. • Patients with acute leukaemia – from diagnosis (unless/until decision made not to proceed with stem cell transplant). • Patients awaiting allogeneic stem cell transplant – from 3 months prior to the date of planned transplant and up to 6 months following transplant, or for as long as the patient is immunosuppressed. • Extra corporeal procedures – only included if within above indications. Indicate requirement on the patient record both in the clinical area and transfusion laboratory. Inform the transfusion laboratory if your patient requires HEV negative blood components If HEV components are not available, the laboratory staff will contact you to discuss the urgency. Can your patient wait for HEV negative blood components? Yes. Laboratory staff will order component from NHS Blood and Transplant and notify you when it is available No Transfuse a component that has not been tested for HEV Management in the transplant patient: • Confirm persistence by re-sampling for PCR and serology at one month. • Seek advice from virology/liver teams to assess liver morphology and fibrosis. • Consider immunosuppressant reduction as it is associated with improved chances of viral clearance. • If no clearance within 3 months, consider a 3 month course of Ribavirin (note: this use is off license). • If you suspect HEV transmission via stem cell transplant or blood component transfusion inform NHS Blood and Transplant immediately. Monitor the patient for features of hepatitis: Jaundice; Darkened urine; Tiredness; Nausea and vomiting; Abdominal pain; Rise in ALT or bilirubin NHS Blood and Transplant Patient Blood Management Team Version 1.1, March 2016 If clinical features present, send Hep E serology and PCR and if suggestive of active infection follow the guidance for management in the transplant patient