10. Blood-gas Hb.doc
advertisement

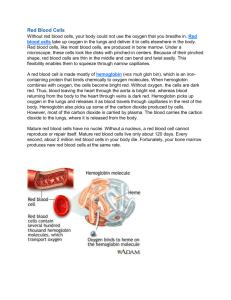
D’YOUVILLE COLLEGE BIOLOGY 108/508 - HUMAN ANATOMY & PHYSIOLOGY II LECTURE # 10 RESPIRATORY SYSTEM II GAS EXCHANGE 5. Alveolar Diffusion: • pulmonary ventilation objective: maintain steady-state gradients favoring diffusion of oxygen into blood and diffusion of carbon dioxide out of blood - atmospheric air pressure = 760 mm. Hg - PO2air = 150 mm. Hg (air contains approx. 20% oxygen) - PO2alveolar = 104 mm. Hg (outside air diluted with residual volume of lungs; PO2venous = 40 mm. Hg; thus, oxygen concentration gradient favoring uptake by blood (fig. 22 - 17) - PCO2air is negligible - PCO2alveolar = 40 mm. Hg (residual volume of lungs contains relatively high carbon dioxide concentration) - PCO2venous = 45 mm. Hg (blood returning from tissues); thus, carbon dioxide concentration gradient favoring carbon dioxide release by blood (fig. 22 - 17) - pressure gradient regulated (ventilation/perfusion coupling - fig. 22 - 19) 6. Blood Gas Transport: • carried out by red blood cells (erythrocytes) containing hemoglobin - hemoglobin contains 4 chains of amino acids (2 alpha and 2 beta polypeptides); each polypeptide chain has a non-amino acid grouping, heme (contains iron) (fig. 17 - 4) - iron of the heme loosely binds molecular oxygen in an easily reversible reaction called hemoglobin oxygenation HHb (reduced hemoglobin) + O2 <---> HbO2 (oxyhemoglobin) + H+ - hydrogen ion is buffered by bicarbonate ion in red cell cytoplasm: H+ + HCO3- (bicarbonate ion) <--------------------------> H2CO3 (carbonic acid) H2CO3 (carbonic acid)<-----------**-----------> CO2 (carbon dioxide) + H2O - ** = enzyme carbonic anhydrase required for reaction • 70% of carbon dioxide is transported in blood as bicarbonate ion; 30%: carbaminohemoglobin & dissolved CO2 - uptake of oxygen provides impetus (H+) for carbon dioxide release (in lungs where PO2 is high and PCO2 is low - fig. 22 - 22) - process reverses in tissues (where PO2 is low and PCO2 is high) Bio 108/508 lec. 10 - p. 2 • chloride shift: in lungs, bicarbonate, used up to buffer acidity from hemoglobin oxygenation, is replaced by uptake from plasma; acquired negative charge is balanced by chloride (Cl-) movement from red cell to plasma; reverse occurs in tissues Bio 108/508 lec. 10 - p. 3 7. Oxyhemoglobin Dissociation Curve: • records hemoglobin’s binding of oxygen at different PO2 values (fig. 22 - 20) - arterial portion: (high PO2 as in lungs) hemoglobin retains oxygen - venous portion: (lower PO2 as in tissues) hemoglobin displays sensitive response to dropping PO2 by releasing oxygen • Bohr effect: high/low PCO2 or low/high pH cause shift in hemoglobin’s response to oxygen levels (fine tuning Hb binding behavior - fig. 22 - 21) - high/low temperatures, other conditions have similar effect - pharmacological or pathological effects of carbon monoxide, oxidation, etc. compromise hemoglobin ability to bind O2 8. Regulation of Ventilation: a. Respiratory Centers: pontine center (pons) modifies activities of centers in medulla oblongata: dorsal respiratory group (DRG) receives sensory input & higher brain input and signals activity of ventral respiratory group (VRG) that sends output to breathing muscles (mostly diaphragm via phrenic nerve - fig. 22 - 23) - sensory inputs modify outputs of respiratory centers: b. Stretch Receptors: signals cause inhibition of inspiration when they are stretched by inflation (Hering-Breuer reflex) - protection against overinflation c. Chemoreceptors: found in carotid and aortic bodies of circulation and chemosensitive areas of medulla (figs. 22 - 24 & 22 - 26); respond to levels of carbon dioxide (PCO2), hydrogen ions (pH) and oxygen (PO2) of blood and/or cerebrospinal fluid; alterations in resp. rate or depth usually are mediated by PCO2 and pH in negative feedback loop (fig. 22 - 25)