Online data supplement
advertisement

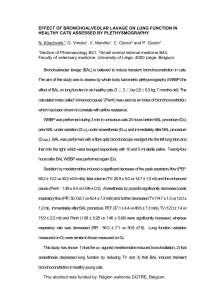
Online data supplement Acute respiratory distress syndrome mimickers lacking common risk factors of the Berlin definition METHODS Identification of patients The medical records of patients hospitalized in the two participating centers between January 2003 and December 2012 for ARDS were reviewed. The following keywords were searched on the hospital record databases: “Acute Respiratory Distress Syndrome”, “ARDS”, “Acute Interstitial Pneumonia”, “Diffuse Alveolar Hemorrhage”, “Drug-induced Acute Lung Injury”. “Common” risk factors from the Berlin definition These include the following factors (Table 1):[1] pneumonia, gastric aspiration, pulmonary contusion, drowning, inhalation of gases, extra-pulmonary sepsis, polytrauma, pancreatitis, burns, non-cardiogenic shock, drug intoxication, and polytransfusion. Patients with “vasculitides” were deemed to have ARDS with no CRF because vasculitides are not pathologically characterized by diffuse alveolar damage. Patients with no “common” risk factors ARDS patients with no common risk factors (ARDSCRF-) were separated into four etiological groups: immune ARDS, drug-induced ARDS, malignant ARDS, and idiopathic ARDS. The immune ARDS group included vasculitides, as defined by the American College of Rheumatology criteria, [2] and connective tissue diseases according to ACR and ARA criteria, with systemic lupus erythematosus,[3] rheumatoid arthritis,[4] mixed connective tissue,[5] inflammatory myopathy[6] and scleroderma. Undifferentiated connective tissue diseases were classified separately, in case of clinical and serological evidence of autoimmunity within the criteria of a conventional connective disease.[7, 8] Thresholds used for positivity were as follows: > 15 IU/mL for rheumatoid factor; > 5 IU/mL for anti-CCP antibodies; titer > 1/160 for antinuclear antibodies, and > 20 IU/mL for anti-neutrophil cytoplasmic antibodies (ANCA). Assessment of lung lesions reversibility The presence of lung lesions potentially responding to therapy with corticosteroids was assessed by three experts blinded to the final diagnosis and to outcome (AP, BM, MF), based on BAL fluid cytology and chest CT scan patterns, and patients were considered as “potential responders” when an agreement of all three experts was met. From this, threshold values for BAL cell counts associated with potential responsiveness to therapy with corticosteroids were obtained with Receiver Operator (ROC) curves (Figures E1 and E2). The composite variable obtained was finally entered into a multivariable logistic regression model aimed at determining factors associated with in-ICU mortality among ARDSCRF- patients.[9]-[10] Data presentation and statistical analysis Categorical variables are expressed as number and percentages (95% confidence interval), and compared with the chi2 test or the Fischer Exact test, as appropriate. Continuous variables are reported as median [interquartile range IQR 25-75] or mean (± standard deviation SD), and compared using the Student t-test or the Mann-Whitney test, as appropriate. The distribution of variables was tested using the Shapiro-Wilk normality test. Comparisons of more than two groups were performed using ANOVA and the Bonferroni post-hoc test, when overall p value was less than 0.05, or using the Kruskal-Wallis test, as appropriate. Two distinct sets of statistical analyses were performed. First, a comparison of ARDSCRF+ and ARDSCRF- patients was performed. Second, ARDSCRF- patients were studied. Factors associated with intensive care unit mortality were determined by univariate and multivariable analyses, both within the whole cohort of patients, and within the ARDSCRF- subgroup. Interaction between variables were tested using the Mantel-Haenzel test, and interaction terms introduced in the multivariable analysis when appropriate. Odds ratios (OR) and their 95% confidence intervals (95% CI) were computed. Independent variables with p<0.10 in univariate analysis were included in the multivariable analysis, with backward elimination of variables displaying a p value >0.05. Analyses were carried out using the SPSS Base 21.0 statistical software package (SPSS Inc., Chicago, IL). RESULTS Based on the experts’ consensus, the variable most significantly associated with the presence of potentially reversible lung lesions was BAL lymphocyte counts, which yielded an area under the ROC curve of 0.88 (Figure 1D). A proportion of lymphocytes >20% in the BAL fluid was associated with the best discrimination between potential responders and nonresponders to steroids, as defined by the experts’ consensus (Figure 1C). BAL neutrophils yielded an area under the curve of 0.79 (Figure 1F), and the threshold value associated with the best discrimination was a proportion of neutrophils <22% in the BAL fluid (Figure 1E). The composite variable “presence of potentially reversible lung lesions” also tended to be associated with the lack of signs consistent with pulmonary fibrosis (honeycombing and traction bronchiectasis, Figure 2) on chest CT scan. References 1. ARDS Definition Task Force, Ranieri VM, Rubenfeld GD, et al. (2012) Acute respiratory distress syndrome: the Berlin Definition. JAMA J Am Med Assoc 307:2526– 2533. doi: 10.1001/jama.2012.5669 2. Jennette JC, Falk RJ, Andrassy K, et al. (1994) Nomenclature of systemic vasculitides. Proposal of an international consensus conference. Arthritis Rheum 37:187–192. 3. Hochberg MC (1997) Updating the American College of Rheumatology revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum 40:1725. doi: 10.1002/1529-0131(199709)40:9&lt;1725::AID-ART29&gt;3.0.CO;2-Y 4. Lee DM, Weinblatt ME (2001) Rheumatoid arthritis. Lancet 358:903–911. doi: 10.1016/S0140-6736(01)06075-5 5. Sharp GC, Irvin WS, Tan EM, et al. (1972) Mixed connective tissue disease--an apparently distinct rheumatic disease syndrome associated with a specific antibody to an extractable nuclear antigen (ENA). Am J Med 52:148–159. 6. Dalakas MC, Hohlfeld R (2003) Polymyositis and dermatomyositis. Lancet 362:971– 982. doi: 10.1016/S0140-6736(03)14368-1 7. Kinder BW, Collard HR, Koth L, et al. (2007) Idiopathic nonspecific interstitial pneumonia: lung manifestation of undifferentiated connective tissue disease? Am J Respir Crit Care Med 176:691–697. doi: 10.1164/rccm.200702-220OC 8. Doria A, Mosca M, Gambari PF, Bombardieri S (2005) Defining unclassifiable connective tissue diseases: incomplete, undifferentiated, or both? J Rheumatol 32:213– 215. 9. Gay SE, Kazerooni EA, Toews GB, et al. (1998) Idiopathic pulmonary fibrosis: predicting response to therapy and survival. Am J Respir Crit Care Med 157:1063–1072. doi: 10.1164/ajrccm.157.4.9703022 10. Terriff BA, Kwan SY, Chan-Yeung MM, Müller NL (1992) Fibrosing alveolitis: chest radiography and CT as predictors of clinical and functional impairment at follow-up in 26 patients. Radiology 184:445–449. doi: 10.1148/radiology.184.2.1620845 Table 1. Common risk factors of the Berlin definition (adapted from [1]). ARDS Risk factor Pneumonia Non-pulmonary sepsis Aspiration of gastric contents Major trauma Pulmonary contusion Pancreatitis Inhalational injury Severe burns Non-cardiogenic shock Drug overdose Multiple transfusions or transfusion-associated acute lung injury (TRALI) Pulmonary vasculitis a Drowning a Pulmonary vasculitis was not considered as a “common risk factor” in the current study, as it is not associated with the presence of diffuse alveolar damage. Table 2. Factors recorded on admission and within 48h of mechanical ventilation and associated with ICU mortality (n=665) n Death n (%) - Univariate analysis OR (95% CI) P 1.03 [1.02-1.04] <0.0001 1.14 [1.10-1.18] <0.0001 Multivariable analysis OR (95% CI) P 1.03 [1.02-1.04] <0.0001 1.09 [1.04-1.06] <0.0001 SAPS II a 665 b LODS 665 Shock Yes 516 299 (58) 1.99 [1.37-2.88] <0.0001 No 149 61 (41) 1 Absence of common risk factors for ARDS Yes 50 33 (66) 1.69 [0.92-3.09] 0.091 2.06 [1.02-4.18] 0.044 No 615 327 (53) 1 Berlin classification with shock c mild 58 31 (53) 1 moderate 280 126 (45) 1.66 [0.49-5.56] 0.41 severe 327 203 (62) 4.65 [1.36-15.94] 0.014 2.04 [1.41-2.95] <0.001 Age d 665 1.02 [1.01-1.03] <0.001 1.02 [1.01-1.03] 0.004 e NIV duration 665 1.17 [1.04-1.32] 0.009 1.46 [1.24-1.71] <0.001 No bacterial infection Yes 306 189 (62) 1.78 [1.30-2.42] <0.001 1.47 [1.03-2.11] 0.033 No 359 171 (48) 1 a per unit of simplified acute physiology score (SAPS II); b per unit of logistic organ dysfunction score (LODS); c interaction variable created from the severity of ARDS and shock; d per year; e per day of non-invasive ventilation (NIV). The Hosmer-Lemeshow goodness of fit test showed good calibration of the model (p=0.37). The area under the ROC curve of the model was 0.76 (sensitivity=74%, specificity=63%). Table 3. Histopathological and cytological diagnoses of ARDS patients with no common risk factors. Cases Lung tissue specimen Cytological/Histopathological patterns Idiopathic ARDS (n=4/13) case 1 OLB DAD, fibroproliferative stage case 2 TB DAD case 3 TB Organizing pneumonia case 4 TB Organizing pneumonia Immune ARDS (n=2/24) case 1 OLB Organizing pneumonia, fibrosis case 2 Autopsy Hemophagocytosis, TL infiltration Drug-induced ARDS (n=2/20) case 1 Autopsy DAD, fibroproliferative stage case 2 Autopsy DAD, fibroproliferative stage Malignant ARDS (n=10/12) cases 1-4 BAL Bronchiolo-alveolar carcinoma cases 5-6 BAL Monoclonal lymphocytes cases 7-10 BB Carcinoma cells OLB, open Lung Biopsy; TB, transbronchial biopsy; BAL, broncho-alveolar lavage; BB, bronchial biopsy; DAD, diffuse alveolar damage; TL, T lymphocytes Figure legends Figure 1. Broncho-alveolar lavage (BAL) fluid cytology for patients with ARDS and no risk factors from the Berlin definition categorized as responders or non-responders to steroids by three experts blinded to management and outcome. BAL cellularity (A), macrophage (B) and eosinophil (G) counts, and the proportion of patients with diffuse alveolar hemorrhage (H) were not different between both groups. In contrast, BAL lymphocytes (C) were higher and neutrophils (E) lower in responders than in non-responders to steroids. Dashed lines show the best threshold values for BAL lymphocytes (alveolar lymphocytes > 20% (C); area under the ROC curve (AUC) = 0.88 (D)) and neutrophils (alveolar neutrophils<22% (E); area under the ROC curve = 0.79 (F)) for discriminating responders from non-responders to steroids. Figure 2. Chest CT scan patterns for patients with ARDS and no risk factors from the Berlin definition categorized as responders or non-responders to steroids by three experts blinded to management and outcome. There was no difference in the proportion of patients with ground glass opacities (A) and septal thickening (D). In contrast, there was a trend towards less frequent honeycombing (B) and traction bronchiectasis (C) in responders than in nonresponders to steroids. Figure 1 A BAL cellularity P=0.52 1.0×106 5.0×105 0.0 C Responders 40 20 0 40 20 Responders Responders D Non-responders BAL lymphocytes 100 Sensitivity (%) BAL lymphocytes (%) 60 0 60 P<0.0001 80 P=0.092 80 Non-responders BAL lymphocytes 100 100 BAL macrophages (%) BAL cells / mL 1.5×106 BAL macrophages B 50 AUC=0.88 0 Non-responders 0 50 100 100 - Specificity (%) F E BAL neutrophils BAL neutrophils P=0.002 Sensitivity (%) BAL neutrophils (%) 100 100 80 60 40 50 AUC=0.79 20 0 Responders 0 Non-responders 0 50 100 100 - Specificity (%) H G Diffuse alveolar hemorrhage BAL eosinophils 25 P=0.34 20 30 Patients (n) BAL eosinophils (%) 40 20 10 0 15 P=0.71 Non-responders Responders 10 5 Responders Non-responders 0 Present Absent Figure 2 A Ground glass opacities 25 B 20 P=0.63 Non-responders Responders 15 10 Patients (n) Patients (n) 20 5 0 Present 15 10 5 0 Absent D C Patients (n) Patients (n) 15 P=0.096 10 5 0 Present Present Absent Absent Septal thickening Traction bronchectasies 15 Honeycombing P=0.065 P=0.34 10 5 0 Present Absent