How Childhood Trauma Effects Learning

How Childhood Trauma
Effects Learning
1
Developed by:
Rhonda Best & Mitch Kremer
Northern Illinois University
Center for Child Welfare and Education
2
The Center for Child Welfare and
Education (CCWE)
A Partnership Between Northern Illinois
University and the Illinois Department of
Children and Family Services
3
“Each of us must come to care about everyone else’s children.
We must recognize that the welfare of our children and grandchildren is intimately linked to the welfare of all other people’s children.
After all, when one of our children needs lifesaving surgery, someone else’s child will perform it.
If one of our children is threatened or harmed by violence, someone else’s child will be responsible for the violent act.
The good life for your own children can be secured only if a good life is also secured for all other people’s children.”
Lillian Katz
Northern Illinois University Center for Child
Welfare & Education - 2013
Training Overview
What is childhood trauma?
What are the implications for education?
What is needed for recovery?
Educational interventions
Secondary trauma
Resources
Plan development
4
Northern Illinois University Center for Child
Welfare & Education - 2013
Outcomes
Understand the nature of childhood trauma
Recognize the impact of trauma on development
Understand the impact of trauma on learning
Gain knowledge of appropriate interventions
Understand the impact of secondary trauma
Develop a plan to address the needs of traumatized children
5
Northern Illinois University Center for Child
Welfare & Education - 2013
Lisa’s
911
Call
7
Childhood Trauma
8
Adverse Childhood Experiences (ACEs)
Growing up in a household with:
Recurrent physical, sexual or emotional abuse
Emotional or physical neglect
Domestic violence between parents
An alcohol or drug abuser
An incarcerated household member
Someone who is chronically depressed, suicidal, institutionalized or mentally ill
One or no biological parents
(2004, http://www.acestudy.org/)
Northern Illinois University Center for Child
Welfare & Education - 2013
Consequences Of Unresolved Trauma
9
Northern Illinois University Center for Child
Welfare & Education - 2013
(2004, http://www.acestudy.org/)
Importance of the Adverse Childhood
Experiences Study
ACEs are surprisingly common – 44% of 13,494 adults reported physical, psychological or sexual abuse as children.
They happen even in “the best of families”.
They can have long-term, damaging consequences for children and society.
(2004, http://www.acestudy.org/)
10
Northern Illinois University Center for Child
Welfare & Education - 2013
Discussion Questions
1.
How does this reflect what you’re seeing?
ACE’s
School violence
2.
What are the unique demographic or social factors in your community that may increase or decrease prevalence?
11
Northern Illinois University Center for Child
Welfare & Education - 2013
12
Trauma and Development
What is Stress?
Stress is the set of changes in the body and the brain that are set into motion when there are overwhelming threats to physical or psychological well-being.
Under threat, the limbic system engages and the frontal lobes disengage. When safety returns, the limbic chemical reaction stops and the frontal lobes reengage.
13
(van der Kolk, B., 2005)
Northern Illinois University Center for Child
Welfare & Education - 2013
Three Types of Stress
Stressful events can be beneficial, tolerable, or harmful:
Positive stress: moderate, short-lived stress responses.
Tolerable stress: more intense stress responses that allow enough time to recover, or occur in a relatively safe environment with the presence of supportive adults.
Toxic stress: strong, frequent or prolonged activation of the body’s stress management system, without access to supportive adults in a safe environment.
(National Scientific Council on the Developing Child, 2005)
14
Northern Illinois University Center for Child
Welfare & Education - 2013
Bimodal Response to Stress
Hyperarousal Dissociation
15
(Externalizing behaviors, more common in males)
Fight
Flight
Hypervigilant
Reactive
Alarm response
Tachycardia
(Internalizing behaviors, more common in females)
Freezing
Fainting
Somatoform dissociation
Numbing
Compliance
Derealization (depersonalization)
The response that is most adaptive for the individual becomes that individual’s automatic response to subsequent stress.
(Adapted from Perry, Child Trauma Academy, 2002)
Northern Illinois University Center for Child
Welfare & Education - 2013
The Stress Response Cycle
17
What is Trauma?
Trauma arises from an inescapable stressful event that overwhelms an individuals’ coping mechanisms
(van der Kolk & Fisler, 1995).
Childhood Trauma:
Experience or witnessing of an event that involves:
* Actual or threatened death or serious injury to self or others
Northern Illinois University Center for Child
Welfare & Education - 2013
* Threat to psychological or physical integrity of self or others
(Zero to Three, 2004)
Isolated Trauma Versus Complex Trauma
Isolated traumatic incidents tend to produce discrete conditioned behavioral and biological responses to reminders of the trauma (as in
PTSD)
18
Complex (chronic) trauma interferes with neurobiological development and the capacity to integrate sensory, emotional and cognitive information into a cohesive whole.
(van der Kolk, B., 2005)
Northern Illinois University Center for Child
Welfare & Education - 2013
19
Responses to Complex Trauma
The trauma response is bimodal: hyper-reactivity to stimuli and traumatic reexperiencing coexist with psychic numbing, avoidance and amnesia (van der Kolk, 2004)
1.
Stimulus generalization
2.
Triggered pattern of repeated dysregulation in response to trauma cues
3.
Anticipatory organization of behavior to prevent the recurrence of the trauma effects
(van der Kolk, B., 2005)
Northern Illinois University Center for Child
Welfare & Education - 2013
20
Early Brain Development
Use-dependent modification is a core principle of neurodevelopment
Brain cells (neurons) that are stimulated mature and connections
(synapses) develop between neurons.
Synapses that are used become a permanent part of the brain.
Synapses that are not used frequently are eliminated.
Northern Illinois University Center for Child
Welfare & Education - 2013
(Perry, 1998)
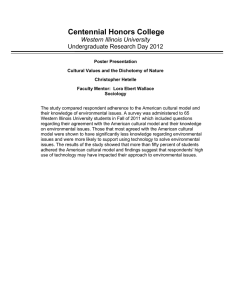
Traumatic Stress and Critical Windows of
Brain Development
21
Cortex
Limbic Brain
cognitive functioning:
12 months - 48 months emotional functioning:
6 months - 30 months
Mid Brain
motor functioning: first year
Brain Stem
Northern Illinois University Center for Child
Welfare & Education - 2013 state regulation: pre-birth - 8 months
(Adapted from: Perry, 2002)
What are the Long-Term Effects of
Traumatic Stress?
The automatic response to trauma or trauma cues, involves the production of toxic amounts of stress hormones (primarily cortisol) which affect:
brain function
all major body systems
social functioning
(Cairns, K. & Stanway, S., 2004.)
22
Northern Illinois University Center for Child
Welfare & Education - 2013
Lasting Effects of Trauma
Effects on brain development and functioning are often global
Physiological effects
Physical effects
Emotional effects
Social effects
(Cairns, K. & Stanway, S., 2004.)
23
Northern Illinois University Center for Child
Welfare & Education - 2013
Possible Long Term Effects on Brain
Functioning
These brain functions may be diminished or lost:
language, especially spoken language
expressing words for feelings sense of meaning and connection empathy impulse control
mood regulation short term memory capacity for joy
(Cairns, K. & Stanway, S., 2004.)
24
Northern Illinois University Center for Child
Welfare & Education - 2013
Physiological Effects
Perpetual extreme levels of stress arousal may lead to:
hypervigilance and loss of ability to concentrate
altered vision and hearing hyperactivity or dissociation avoidance of potential triggers to trauma altered sleep patterns
altered eating patterns compulsive self harm attempts to self medicate with substances
(Cairns, K. & Stanway, S., 2004.)
25
Northern Illinois University Center for Child
Welfare & Education - 2013
Physical Effects
Continued stress arousal may lead to:
headaches
digestive disorders respiratory disorders other psychosomatic illnesses muscle tension
aching joints clumsiness altered spatial awareness
(Cairns, K. & Stanway, S., 2004.)
26
Northern Illinois University Center for Child
Welfare & Education - 2013
Emotional Effects
Inability to process emotions through language
Diminished capacity for empathy
Hypersensitivity to trauma in others
Diminished range of emotions: terror or rage
Diminished aesthetic and spiritual experiences
Feelings of worthlessness and shame
Traumatic stress takes over core identity
(Cairns, K. & Stanway, S., 2004.)
27
Northern Illinois University Center for Child
Welfare & Education - 2013
Social Effects
May become socially isolated or member of deviant peer group due to:
Extreme reactions of terror or rage
Diminished empathy limits social connectedness
Survival mode restricts motivation to be sociable
Avoidance restricts capacity to connect to others
Diminished language restricts social accountability
Traumatic identity leads to persistent victim or aggressor behaviour
(Cairns, K. & Stanway, S., 2004.)
28
Northern Illinois University Center for Child
Welfare & Education - 2013
Discussion Questions
1.
Does the research presented on childhood trauma help you to look at children in your classrooms or schools differently?
2.
How might this information help you to better meet children’s needs?
29
Northern Illinois University Center for Child
Welfare & Education - 2013
30
Resiliency and Recovery
Shaping the Early Brain
Dr. Bruce Perry, Texas Children’s Hospital, a leading researcher in early brain development and childhood trauma:
“Children are not resilient, they are malleable.”
Resilient: “Able to recover readily from misfortune”
Malleable: “Capable of being shaped or formed”
“Childhood experiences define the adult by shaping the developing brain.”
NATURE VS. AND NURTURE
31
Northern Illinois University Center for Child
Welfare & Education - 2013
What is Resiliency?
Resilience describes an individual’s positive functioning despite experiencing adverse circumstances.
Resiliency is influenced by vulnerability factors, compensatory factors, and protective factors, operating at the individual, family and community levels.
Should NOT be considered an individual character trait
(Luthar & Cicchetti, 2000)
32
Northern Illinois University Center for Child
Welfare & Education - 2013
Factors that Influence Recovery
The child’s personality
Strong social competence – the ability to be empathetic, caring
& responsive
Creative thinking - problem solving, resourcefulness
Autonomy – strong self-esteem, ability to separate self from dysfunctional environment
Sense of purpose – optimism, persistence toward achieving goals, hopeful outlook for future
(Luthar & Cicchetti, 2000)
33
Northern Illinois University Center for Child
Welfare & Education - 2013
Factors that Influence Recovery
The type of trauma
Children who experience an isolated trauma, such as a natural disaster, will more quickly gain a sense of control because the stressful event comes to an end.
Children who experience complex trauma (violent neighborhood, abuse, domestic violence) have more difficulty with recovery because they can’t separate from the stressful environment.
(Luthar & Cicchetti, 2000)
34
Northern Illinois University Center for Child
Welfare & Education - 2013
Factors that Influence Recovery
Strong support systems - the majority of children that are provided with strong support systems overcome developmental damage and actually use the challenges from their lives to develop strength and confidence
Individualized intervention strategy, that includes
Therapeutic support
Family support
School support
Community support
(Luthar & Cicchetti, 2000)
35
Northern Illinois University Center for Child
Welfare & Education - 2013
Discussion Questions
There is a correlation between resiliency and recovery and the quality of supports surrounding a child.
What supports are already available in your
School?
Community?
What supports need to be developed?
36
Northern Illinois University Center for Child
Welfare & Education - 2013
37
Let’s Take A Break!
Back in 10?
38
Effects of Trauma on Learning
“Most of them (learners at risk) are very tough and tenacious in confronting the challenges life presents to them. Despite the difficulties they face, they continue to respond with the best they can draw out of their personal resources and experience. If their responses are less than fully competent, or even maladaptive, this is the result of faulty knowledge rather than lack of effort.”
Frank H. Wood
39
Northern Illinois University Center for Child
Welfare & Education - 2013
Opportunity for Intervention
40
Source: Thompson, UCLA Laboratory of Neuroimaging, &
Giedd, National Institutes for Mental Health, 2004
The prefrontal cortex doesn’t fully develop until about age 21, it’s functions include:
* Reasoning * Problem solving
* Integrating information from the senses
Northern Illinois University Center for Child
Welfare & Education - 2013
Why is it more difficult for schools to work with children who are traumatized?
Issues over changes of placement or mobility
Lack of adequate information or expertise
Lack of clarity about roles and responsibilities
Lack of knowledge and skill to deal with traumatized children
Difficulty of containing post traumatic behaviours in the school environment
Effects of secondary traumatic stress
(Cairns, K. & Stanway, S., 2004)
41
Northern Illinois University Center for Child
Welfare & Education - 2013
Explicit and Implicit Memory
CORTEX: higher level thought processes, planning, problem solving
HIPPOCAMPUS:
Explicit memory governs recollection of facts, events or associations
AMYGDALA:
Implicit memory – No conscious awareness
(procedural memory – e.g., riding a bike and emotional memorye.g., fear) Adrenal gland
42
Chronic stress = overstimulation of the Amygdala, resulting in the release of cortisol, possible shrinkage or atrophy of the Hippocampus and Cortex , affecting memory and cognition, and leading to anxiety or depression.
(Adapted from: Brunson, Lorang, & Baram, 2002)
Northern Illinois University Center for Child
Welfare & Education - 2013
Effects of Trauma on IQ and
Achievement
Research shows substantial decrements in both IQ and reading due to trauma.
7.5 point decrements in IQ
9.8 point decrements in reading achievement
(Delaney-Black, et.al., 2002)
43
Northern Illinois University Center for Child
Welfare & Education - 2013
44
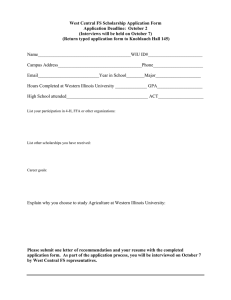
Most Frequent Difficulties Following
Chronic Trauma
75%
60%
45%
30%
15%
61.5%
59.2%
57.9%
53.1%
45.8%
0%
Af fe ct
D ys re gu la tio n
At te nt io n/
C on ce nt ra tio n
N eg at iv e
Se lf-I m ag e
Northern Illinois University Center for Child
Welfare & Education - 2013
Im pu ls e
C on tro l
Ag gre ss io n/
R is k-t ak in g
(Spinazzola.J, et.al., 2005)
How Traumatized Children are Typically
Diagnosed
45
The most common psychiatric diagnoses in order of frequency:
separation anxiety disorder
oppositional defiant disorder
phobic disorders
PTSD
ADHD
(van der Kolk, B., 2005)
Northern Illinois University Center for Child
Welfare & Education - 2013
Relationship Between Diagnoses & Eligibilities
Special Education Eligibility:
Emotional Disturbance
Inability to learn not explained by health, intellectual, or sensory disability;
Inability to build/maintain relationships;
Inappropriate behavior or feelings under normal circumstances;
Pervasive anxiety or depression;
Physical symptoms or fears.
Psychological/Neurobiological Diagnosis:
Traumatic Stress
Rarely in attentive state
Defiant, aggressive, oppositional
Hyperarousal
Internalizing disorders
Fear, somatic disorders
Special Education Eligibility:
Specific Learning Disability
Disorder in basic psychological processes involved in understanding/using language, spoken or written, may manifest in an imperfect ability to listen, think, speak, read, write, spell, or do mathematical calculations.
Rarely in attentive state;
Lack of concentration;
Misperceptions;
Avoidance;
Dissociation;
Repeated intrusive memories
(Shumow & Perry, 2006)
46
Northern Illinois University Center for Child
Welfare & Education - 2013
47
Manifestations of Trauma that Affect
School Performance
Externalizing Behaviors: Coping by acting out on external world
(physical/verbal aggression).
More visible
More likely to receive intervention in school
Internalizing Behaviors: Coping by withdrawing into the self (anxiety, depression, dissociation).
Less visible
Less likely to receive intervention in school
Somatic Disorders:
Frequent visits to school nurse
Frequent school absences
(Shumow & Perry, 2006)
Northern Illinois University Center for Child
Welfare & Education - 2013
How we Perceive Traumatized Children
Many problems of traumatized children can be understood as efforts to minimize objective threat and to regulate their emotional distress
Unless teachers understand the nature of such re-enactments, they are likely to label the child as
“oppositional,” “rebellious,” “unmotivated,” or
“antisocial”
(van der Kolk, B., 2005)
48
Northern Illinois University Center for Child
Welfare & Education - 2013
Power and Control Strategies that are NOT
Beneficial
Threats
Bribes
Control over bodily functions, like prohibiting children from using the bathroom
Random enforcement of petty rules
Humiliation or degradation
Isolation
Corporal punishment
(van der Kolk, 2006)
49
Northern Illinois University Center for Child
Welfare & Education - 2013
What Youth Say:
“I changed schools three times, so friends were hard to keep. I had a lot of conflict at school. I felt isolated and alienated.”
“School was the most consistent thing in my life. I moved around a lot and I went to nine different elementary schools. But I always knew that my teacher was going to be there when I got there every morning and I didn’t have that at home.”
50
Northern Illinois University Center for Child
Welfare & Education - 2013
Discussion Questions
1.
What problems stem from school and mental health providers not sharing common terminology, eligibilities and diagnoses?
2.
Knowing that for traumatized children some behaviors are organic rather than willful, how do we reconcile that with current discipline policies?
51
Northern Illinois University Center for Child
Welfare & Education - 2013
52
Interventions for Children with Trauma
53
Curriculum for Traumatized Children
Connecting
1 Safety
2 Engaging
3 Trusting
Processing
4 Managing the self
5 Managing feelings
6 Taking responsibility
Adapting
7 Developing social awareness
8 Developing reflectivity
9 Developing reciprocity
(Cairns, K. & Stanway, S., 2004.)
Northern Illinois University Center for Child
Welfare & Education - 2013
Step I - Safety First
Stay aware of the terror
Provide and sustain a relaxing environment
Use self appropriately to deal with a terrified flight animal: voice, gestures, expression
Use group work skills to create sense of safety
Bring relaxation into the awareness of the child and encourage practice
Discourage dependence on high stimulus activities
54
Northern Illinois University Center for Child
Welfare & Education - 2013
55
Step II - Engaging
Provide appropriate environmental stimulation for adults and children
Learning about the effects of trauma is part of the treatment
Stories and metaphors are powerful tools for teaching about overwhelming events
Encourage expression of experience and development of emotional intelligence
Bring dissociation into awareness, develop sense of protector self and observer self
Northern Illinois University Center for Child
Welfare & Education - 2013
Step III - Trusting and Feeling
Accept the level of trust the child has to offer
Encourage open discussion of issues of trust
Encourage the child to express inner states in words, even though they will find this difficult
Notice non-verbal signals of feelings and help child to recognize and name what is happening
Identify self-transcending as well as self-assertive emotions
56
Northern Illinois University Center for Child
Welfare & Education - 2013
Step IV - Managing the Self
Discuss and practice relaxation and soothing activities with the child
Avoid asking ‘why did you do that?’ Instead invite reflection linking inner state with actions
Encourage the child to be interested in their own inner state with regard to their behaviour
Comment on small indicators of self-regulation
Encourage children to build on growing capacity for selfmanagement
57
Northern Illinois University Center for Child
Welfare & Education - 2013
Step V - Managing Feelings
Expect and contain disturbed behaviour
Help child to engage with therapy
Encourage child to feel more in control - space, time, activities
Limit choices, restrict choice-making to less stressful situations and celebrate successes
Encourage child to recognize and celebrate learning from mistakes
58
Northern Illinois University Center for Child
Welfare & Education - 2013
Step VI - Taking Responsibility
Recognize the power of traumatic identity and expect resistance to changing identity
Provide choices about how they see themselves
Allow child to let go of excessive or inappropriate responsibilities
Encourage child to allow adults to be in control appropriately
Celebrate any evidence of the child taking appropriate responsibility for behaviour
59
Northern Illinois University Center for Child
Welfare & Education - 2013
VII - Developing Social Awareness
Encourage friendships and social interaction
Identify and rehearse social situations requiring self-control in the child
Encourage the child to broaden the range of their social connections and to be interested in people generally
Promote activities motivating social accountability such as sport, drama, music
60
Northern Illinois University Center for Child
Welfare & Education - 2013
VIII - Developing Reflectivity
Promote self-esteem; catch them doing something good
Provide and comment on role models of centered people who are comfortable in their own lives
Encourage the use of tools for reflection such as keeping a diary
Help children deal with feedback from a range of social situations
Be creative about ways to help the child become fearlessly reflective
61
Northern Illinois University Center for Child
Welfare & Education - 2013
IX - Developing Reciprocity
Provide and invite reflection on wide range of aesthetic experiences
Share thoughts and feelings
Apologize when we hurt the child
Encourage the child to reflect on our experience as well as their own
Invite the child to take our position - ‘What do you think I should do about this?’ in response to child’s behaviour
Accept that we are a problem for the child
62
Northern Illinois University Center for Child
Welfare & Education - 2013
63
1.
2.
3.
4.
5.
6.
7.
8.
9.
Dealing with Individual Incidents of Posttraumatic Behavior
Safety first
Engaging
Trusting and Feeling
Managing the self
Managing feelings
Taking responsibility
Developing social awareness
Developing reflectivity
Developing reciprocity
Northern Illinois University Center for Child
Welfare & Education - 2013
64
Illinois Children’s Mental Health Act and the Illinois Learning Standards
Children’s Mental Health Act of 2003
Required ISBE to incorporate social/emotional development as part of the Illinois Learning Standards.
By August, 2004 Every Illinois School District was to develop a policy for incorporating social and emotional development into the district’s educational program, which addresses:
Teaching
Assessment
Protocols for responding to social/emotional problems that impact learning
65
Northern Illinois University Center for Child
Welfare & Education - 2013
Social/Emotional Learning Standards
Goal 1: Develop self-awareness and selfmanagement skills to achieve school and life success.
A.
B.
C.
Identify and manage one’s emotions and behavior.
Recognize personal qualities and external supports.
Demonstrate skills related to achieving personal and academic goals.
66
Northern Illinois University Center for Child
Welfare & Education - 2013
Social/Emotional Learning Standards
Goal 2: Use social-awareness and interpersonal skills to establish and maintain positive relationships.
A.
B.
C.
D.
Recognize the feelings and perspectives of others.
Recognize individual and group similarities and differences.
Use communication and social skills to interact effectively with others.
Demonstrate an ability to prevent, manage, and resolve interpersonal conflicts in constructive ways.
67
Northern Illinois University Center for Child
Welfare & Education - 2013
Social/Emotional Learning Standards
Goal 3: Demonstrate decision-making skills and responsible behaviors in personal, school, and community contexts.
A.
B.
C.
Consider ethical, safety, and societal factors in making decisions.
Apply decision-making skills to deal responsibly with daily academic and social situations.
Contribute to the well-being of one’s school and community.
68
Northern Illinois University Center for Child
Welfare & Education - 2013
Discussion Question
1.
How can these recommendations for traumatized children support your implementation of the learning standards?
69
Northern Illinois University Center for Child
Welfare & Education - 2013
70
Secondary Trauma
Trauma is catching:
Secondary Traumatic Stress
Secondary traumatic stress is the stress that results from caring for or about someone who has been traumatized.
It can result in injuries similar to those produced by primary trauma.
People who are empathic, and/or have experienced trauma in their own lives, and/or have unresolved personal trauma are vulnerable.
People who care for traumatized children are particularly vulnerable to secondary traumatic stress.
(Cairns, K. & Stanway, S., 2004.)
71
Northern Illinois University Center for Child
Welfare & Education - 2013
Impact of STS on individuals
Performance
decrease in quality and quantity
increased mistakes avoidance of tasks
perfectionism obsessiveness exhaustion irresponsibility
Morale
decrease in confidence apathy dissatisfaction
negativity feel incomplete subsume own needs detachment
(Cairns, K. & Stanway, S., 2004.)
72
Northern Illinois University Center for Child
Welfare & Education - 2013
Impact on whole network
Withdrawal
Lack of appreciation
Impatience
Increase in conflict
Poor communication
Persecutor/victim/rescuer dynamic
73
Northern Illinois University Center for Child
Welfare & Education - 2013
(Cairns, K. & Stanway, S., 2004.)
Discussion Questions?
1.
In what ways do you see secondary trauma affecting your school staff?
2.
How do you currently support school staff who may be impacted by secondary trauma?
74
Northern Illinois University Center for Child
Welfare & Education - 2013
Community Resources
Family Violence Shelters:
Family Shelter Service (Bi-lingual) 630-
469-5650
Hamdard Center (South Asian & Mid-
Eastern) 630-860-9122
Sexual Assault Programs:
DuPage Cty. Children’s Sexual Abuse
Center 630-407-2750
Mutual Ground 630-897-0080
YWCA West Suburban Sexual Assault
Hotline 630-971-3927
Violence & Prevention Training :
Prevent Child Abuse IL 630-790-
6869
Family Shelter Service 630-469-
5650
75
Northern Illinois University Center for Child
Welfare & Education - 2013
Plan Development
How do you communicate the information to your staff?
Who else needs this information? Whose buy-in do you need to get?
How to incorporate with current policies MHA, how to implement, etc.
Identifying resources you have
Identifying gaps in resources
Addressing secondary trauma
Other issues unique to your school or district
Identify first steps (3?)
Follow up
76
Northern Illinois University Center for Child
Welfare & Education - 2013
Recommended Reading:
Right on Course: How trauma and maltreatment impact children in the classroom, and how you can help.
Available from: Civitas, www.civitas.org
Learn the Child: Helping looked after children to learn.
Available from: British Association for Adoption & Fostering, www.baaf.org.uk
Helping Traumatized Children Learn: Supportive school environments for children traumatized by family violence.
Available from: Massachussets Advocates for Children, www.massadvocates.org
77
Northern Illinois University Center for Child
Welfare & Education - 2013
Content for this presentation was compiled from the following sources:
The Adverse Childhood Experiences Study, The Effects of Adverse Childhood
Experiences on Adult Health and Well Being. Retrieved 12/21/04: http://www.acestudy.org/
Bedics, B. C., Rappe, P. T., and Sansone, F. A. (1998). Trauma of children in a residential wilderness treatment program. TRAUMATOLOGYe , Volume IV: 2,
Article 2. <http://www.fsu.edu/~trauma/art3v4i2.htm>
Brendtro, L. (1988). Problems as opportunities: Developing positive theories about troubled youth. Journal of Child Care, 3, 15-24.
Brunson KL, et. al. (2002): Corticotropin releasing hormone (CRH) downregulates the function of its receptor (CRF-1) and induces CRF-1 expression in hippocampal and cortical regions of the immature rat brain. Exp
Neurol 176:75 –86.
78
Northern Illinois University Center for Child
Welfare & Education - 2013
Presentation Sources, Continued.
Cairns, K. & Stanway, S., 2004. Learn the Child - Helping looked after children to learn: a good practice guide for social workers, carers and teachers
Skyline House:London.
De Kloet, E.R., et.al. (1991). Brain Corticosteriod Receptor Balance and
Homeostatic Control. Frontiers of Neuroendocrinology, 12, 95-164.
Delaney-Black, V. M.D., MPH. Violence Exposure, Trauma, and I.Q. and/or
Reading Deficits Among Urban Children. Archives of Pediatric and Adolescent
Medicine, 2002; 156:280-285.
Excessive Stress Disrupts the Architecture of the Brain. (2005). National
Scientific Council on the Developing Child, Working Paper No. 3. Retrieved 8-
17-2006, from http://www.developingchild.net/reports.shtml
.
79
Geroski, A. Addressing the Needs of Foster Children Within a School
Counseling Program. Northern Lights Special Collection Document. (Vol.3
No.3; p 152)
Northern Illinois University Center for Child
Welfare & Education - 2013
Presentation Sources, Continued.
80
Kraimer-Rickaby, L. (1998) Creating a Nurturing Environment for Foster Children in School-Age Child Care. University of Connecticut. Retrieved 3/5/05 from: http://www.canr.uconn.edu/ces/child/newsarticles/SAC744.html.
Luthar, S., Cicchetti, D., & Becker, B. The Construct of Resilience: A Critical
Evaluation and Guidelines for Future Work. Child Development, May/June
2000, v. 71, n. 3, pp. 543-562.
Palmer, L.F. (2001). Baby Matters: What your Doctor may not tell you about caring for your baby. Lancaster, OH:Lucky Press.
Perry, B. Childhood Experience and Expression of Genetic Potential: What
Childhood Tells us About Nature and Nurture. Brain and Mind, v. 3, pp. 79-100,
2002. Retrieved on 8-17-06 from: http://www.childtrauma.org/ctamaterials/MindBrain.pdf
Sapolsky, R. (2003). Taming Stress: An emerging understanding of the brain’s stress pathways.
Scientific American , September, 2003 .
Northern Illinois University Center for Child
Welfare & Education - 2013
Presentation Sources, Continued.
Schwartz, W. (Sept, 1999) School Support For Foster Families. Clearinghouse on
Urban Education. (Number 147).
Smider, M.J., et.al. (February 2002). Salivary Cortisol as a Predictor of
Socioemotional Adjustment during Kindergarten: A Prospective Study. Child
Development, Jan/Feb 2002, V 73, No. 1, 75-92.
Spinazzola, J., et. al. Survey Evaluates Complex Trauma Exposure, Outcome and Intervention Among Children and Adolescents. Psychiatric Annals, 35:5, pp. 433-439, May 2005.
van der Kolk, B. Developmental Trauma Disorder, Psychiatric Annals, pp. 401-
408, 2005.
van der Kolk, B. The Neurobiology of Childhood Trauma and Abuse. Child &
Adolescent Clinics of North America vol 12(2): 293-317. 2003.
81
Northern Illinois University Center for Child
Welfare & Education - 2013
Presentation Sources, Continued.
Walker, E., et.al. Costs of Health Care Use by Women HMO Members with a History of Abuse and Neglect. Arch Gen Psychiatry,
1999;56:609-613.
Zhang, Y., et.al. Effects of language experience: Neural commitment to language-specific auditory patterns. NeuroImage 26 (2005) 703 –720 .
Retrieved 8-30-06 from: http://ilabs.washington.edu:16080/kuhl/pdf/Zhang_Kuhl_2005.pdf
82
Northern Illinois University Center for Child
Welfare & Education - 2013