HIV/AIDS Epidemiology Update

HIV/AIDS Epidemiology
Update
February 2009
Dr Nigel Dickson
Director, AIDS Epidemiology Group
Department of Preventive and Social Medicine
University of Otago, Dunedin
Update data on HIV diagnoses through antibody testing
• 2008 figures and trends – 1999-2008
• New analyses
– Ethnicity
– “Late testers”
• Mention new project
– Follow up questionnaires
2008 figures and trends in people diagnosed with HIV through antibody testing – 1999-2008
Care with data …
• Year of diagnosis not infection
• Not all infected in New Zealand will have been diagnosed
• Some infected people (most diagnosed initially overseas) do not have an antibody test in NZ
– the data on these people captured through viral load testing
200
180
160
140
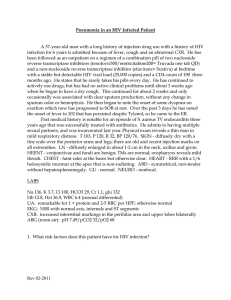
Diagnosed HIV – through antibody testing
– by year of test
Unknown
Perinatal
Other
IDU
Heterosexual contact
Homosexual contact
120
100
80
60
40
20
0
85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 00 01 02 03 04 05 06 07 08
Year of Diagnosis
50
40
30
20
10
0
80
70
60
100
Annual number of men diagnosed, infected through homosexual contact (MSM)
90
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
70
60
50
40
30
20
10
0
70
60
50
40
30
20
10
0
MSM diagnosed with HIV – 1999-2008
Place of infection
NZ
Overseas
Unk
70
Place of residence at diagnosis
60
50
40
30
20
10
0
Auckland
Other NZ
Overseas/unk
Age at diagnosis Ethnicity
15-19
20-29
30-39
40-49
50+
70
60
50
40
30
20
10
0
Europ
Maori
PI
Asian
African
Other
Men and women diagnosed infected through heterosexual contact
50
45
40
35
30
25
20
15
10
5
0
Men
Women
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
80
70
60
50
40
30
20
10
0
Heterosexually infected men and women diagnosed with HIV – 1999-2008
Place of infection
NZ
Overseas
Unk
35
30
25
20
15
10
5
0
50
45
40
Place of residence at diagnosis
Auckland
Other NZ
Overseas/unk
35
30
25
20
15
10
5
0
50
45
40
Age at diagnosis
<15
15-19
20-29
30-39
40-49
50+
60
50
40
30
20
10
0
Ethnicity
Europ
Maori
PI
Asian
African
Other
International comparison of MSM diagnosis rates – 2000-6
• Data recently published from 27/30 european
(EU/EFTA ) countries
• Canadian, Australian and US data from national surveillance reports
Care with data…
• Different patterns of HIV testing may exist
• Rates of diagnosis derived from number of all men not MSM
160,0
140,0
120,0
100,0
80,0
60,0
40,0
20,0
0,0
HIV diagnosis rate among MSM in major Western European countries + Australia, Canada, US and New Zealand
Per million men aged
15-64yr
2000 2001 2002 2003 2004 2005 2006
Australia
Austria
Belgium
Canada
France
Germany
Greece
Ireland
Italy
Netherlands
Norway
Portugal
Spain
Sweden
Switzerland
United Kingdom
United States
New Zealand
Ethnicity among people diagnosed with HIV through antibody testing
• Information collected from clinician
• Recent decade - 1999-2008
Care with data…
• How ethnicity is determined
• Rates of testing
• Relatively small numbers
Numbers of people diagnosed with
HIV by year and ethnicity
70
60
50
40
90
80
30
20
10
0
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008
Europ
Maori
PI
Asian
African
Other
Unk
Comparing disease between ethnic groups 1999-2008
Derive and compare rates
– Numerator from clinician, denominator from census
We have looked at… a) …overall comparison of diagnosis rates as an indication of newly recognised burden in these populations b) …comparison of age adjusted rate of diagnosis as a surrogate of infection risk
Comparison of rates of newly diagnosed HIV among children and adults by means of infection
0-14yr
Number
Relative
Rate and
95% CI
European
4
1.0
(Reference)
MSM (all men
15-59yr men)
Number
Relative
Rate and
95% CI
631
1.0
(Reference)
Heterosexual males (all men
15-59yr men)
Number
Relative
Rate and
95% CI
77
1.0
(Reference)
Heterosexual females (all women 15-59yr men)
Number
Relative
Rate and
95% CI
57
1.0
(Reference)
Maori
6
4.5
(1.3-16.0)
92
0.80
(0.64-1.0)
10
0.71
(0.37-1.4)
13
1.2
(0.66-2.2)
Pacific
3
4.6
(1.0-20.7)
26
0.49
(0.33-0.72)
9
1.4
(0.69-2.8)
15
3.1
(1.8-5.5)
Asian
4
8.9
(2.2-35.8)
59
0.76
(0.58-1.0)
52
5.5
(3.9-7.8)
54
7.2
(4.9-10.4)
Other
30
527
(185-1500)
39
4.8
(3.5-6.7)
149
150
(114-197)
171
273
(202-368)
Comparison of risks to predict future disease pattern in New Zealand
• Use diagnosis rates as surrogates for infection rates
• Need to take into account different age structures of population
– Comparing age standardised rates and report as standardised incidence ratios + confidence intervals
• Does the rate of infection in New Zealand give a better indication of likely future trends for infections here?
– Overall SIRs and 95% CI
– ‘”Infected in New Zealand” SIRs and 95% CI
Standardised incidence ratio + 95% CI
All infections
All
MSM
Hetero -
Males
Hetero -
Females
European Maori Pacific Asian Other
1.0
(Reference)
0.82
(0.67-97)
1.0
(Reference)
0.80
(0.64-0.97)
1.0
(Reference)
0.75
(0.36-1.14)
1.0
(Reference)
1.2
(0.62-2.0)
0.83
(0.63-1.07)
0.48
(0.31-0.71)
1.5
(0.67-2.8)
2.7
(1.5-4.5)
2.O
(1.7-2.2)
0.77
(0.59-0.98)
5.9
(4.4-7.7)
6.4
(4.8-10.2)
42
(38-46)
4.7
(3.4-6.5)
154
(130-180)
245
(210-284)
Standardised incidence ratio + 95% CI
People infected in New Zealand
All
MSM
Hetero -
Males
Hetero -
Females
European Maori Pacific Asian Other
1.0
(Reference)
1.0
(Reference)
1.0
(Reference)
1.0
(Reference)
1.3
(1.0-1.6)
1.2
(0.88-1.5)
1.5
(0.48-3.5)
2.8
(1.4-5.0)
0.81
(0.52-1.6)
0.53
(0.28-0.91)
1.3
(0.16-4.7)
3.3
(1.2-7.3)
0.96
(0.70-1.29)
0.75
(0.49-1.1)
1.3
(0.27-3.8)
3.6
1.7-6.7)
5.2
(3.2-7.8)
2.6
(1.2-4.8)
8.1
(1.0-29.3))
27
(9.8-58)
Beware of CIs as small number in reference population
Late diagnoses of HIV infection among adults in New Zealand
“Early” diagnosis of HIV infection allows…
• optimal decision regarding individual’s therapy
• helps in control of spread
– Behaviour change
– Reduction in viral load
“Late” diagnosis doesn’t!
We defined “Late tester” either …
• Diagnosis of AIDS around time of HIV diagnosis
– Within 3/12 of each other
• Initial CD4+ count ‹200 cells per µlitre
Two things influence “late testers” as a proportion of all diagnoses
• Testing practices
• Dynamics of underlying HIV epidemic
A higher proportion of “Late testers” found if:
(a) Less testing of asymptomatic people
(b) In the late-stage of a declining epidemic
(c) Both
682 HIV diagnoses among adults through antibody testing 2005-8
( initial CD4 counts first collected here in 2005)
• Initial CD4 count reported for 71% (490/682)
• Of these 30.6% (150/490) “late testers”
Are there different proportions of “late testers” among people diagnosed by demographic and other characteristics?
“Late testers” by means of infection - 2005-8
MSM
Heterosexual
Other
Unknown
Total
New diagnoses
245
217
6
22
490
‘Late testers’ OR CI (95%)
24.5%
36.9%
33.3%
36.4%
1.0
1.8
Ref.
1.2-1.7
Adj.
OR* CI (95%)
1.0
Ref.
2.0
1.34-3.1
1.6
0.41-11.1
1.2
0.21-7.1
30.6%
* Adjusted for age
Late testers among MSM 2005-8
Year
Age at Diagnosis
Ethnicity
Place of infection
Reason for testing
2005/6
2007/8
<30
30-39
40+
European
Maori
Pacific
Other
New Zealand
Overseas
Symptoms
Other
New diagnoses
127
118
44
85
116
171
32
7
33
185
55
87
154
‘Late testers’
24.4%
24.6%
6.8%
22.4%
32.8%
21.1%
40.6%
28.6%
27.3%
24.9%
23.6%
46.0%
13.0%
OR
CI
(95%)
Adj.
OR* CI (95%)
1.0
Ref.
0.93
0.51-1.7
1.0
Ref.
4.0
1.1-14.5
6.8
2.0-23.4
1.0
4.5
Ref.
1.9-11.0
2.7
0.47-15.1
1.9
0.79-4.8
1.0
Ref.
0.94
0.46-1.95
5.0
1.0
2.6-9.5
Ref.
* Adjusted for age
Late testers among heterosexual men and women -
2005-8 – work in progress
Year
Gender
Age at Diagnosis
Ethnicity
Place of Infection
Reasons for testing
Total
2005/6
2007/8
Men
Women
<30
30-39
40+
European
Maori
Pacific Island
Other
New Zealand
Overseas
Unknown
Symptoms
Immigration medical
Other
Unknown
New diagnoses
125
92
110
107
47
90
80
40
11
8
158
40
169
8
62
69
81
5
217
“Late testers”
32.8%
42.4%
45.5%
28.0%
27.7%
34.4%
45.0%
42.5%
54.5%
50.0%
33.5%
37.5%
37.3%
25.0%
66.1%
26.1%
19.8%
100.0%
36.9%
Some international comparisons
Country
NZ†
France†
Source
National surveillance
6 tertiary centers
UK and
Ireland*
Info. from providers
(76% RR)
Australia† National surveillance
Year
CD4<200 (+/- clinical late)
Overall MSM Hetero
2005-8 30.6% 24.5% M 46%
F 28%
2004 –5 31.5% Hetero>MSM
2006
2000-6
33%
Est 25%
20%
19.5%
M 43%
F 36%
Est. 39%
† CD4<200+clinical late *CD4<200
New initiative
• Follow up questionnaire with clinician 3/12 post diagnosis
– Up date information
– Check for AIDS diagnosis
– Ask about partner notification
• Clinicians asked to give questionnaire to patient for him/her to return directly to us
– Circumstances of HIV acquisition (if known)
– Includes the census ethnicity question
Conclusions
• Worrying continuing increased level of new diagnoses
– Safest to assume a reflection of new infections
• Rise in diagnosis rate in New Zealand also seen in most
Western European countries, US, Canada and Australia between 2000-2006
• Burden of new diagnoses not borne equally but all ethnic groups
• If diagnosis rate of infections within New Zealand a surrogate for infection rates no major differences between ethnic groups among men, but among women relative to European women, women of “other” ethnic groups, Pacific and Maori women at greater risk
• Late diagnosis rates slightly higher than Australia and similar to
UK and France
– Among MSM late diagnosis higher among Maori
My recommendations
• Review current of national strategy and action for HIV prevention + surveillance
• Consider when prevention needs to be specific for HIV and when it should be part of general STI prevention
• Improve surveillance of other STIs to identify risks among MSM
Acknowledgements
• Organisers and funders of this meeting
• Funding of AEG Ministry of Health
• Clinicians who provide data
• Other members of AEG
– Sue McAllister (Research Officer)
– Charlotte Paul (Epidemiologist)
– Katrina Sharples (Statistician)
– Patricia Priest (Epidemiologist) www.aidsepigroup.otago.ac.nz/