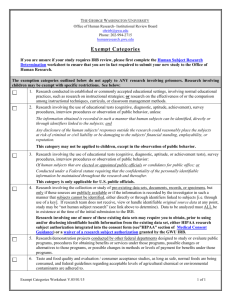
Administrative Pre-Review Checklist for CIRB Protocols

CIRB ADMINISTRATIVE PRE-REVIEW CHECKLIST
PI Name:_ ____________________ IRB-HSR # _____________
Training Current? Yes No If no, who? _ _________________________________________________________
Funded by Grant? No Yes GIRB # Sponsor? List as Sponsor in database
Funded by Contract? No Yes Sponsor? List as Sponsor in database
Is the PI an attending at UVa? Yes No
IRB of Record: Name Institutional Affiliation (if applicable)
Is an IRB Reliance Agreement with this CIRB on file? Yes No If yes, IRB-HSR #
If no, refer to AG 2-36.
Does a UVa researcher have a conflict of interest in this protocol? Yes No
If yes- is there a COI Management plan from the COI Committee? Yes No
If yes, the IRB-HSR will send this plan to the IRB of Record. Completed
Enter date and person who sent the plan
ADDITIONAL APPROVALS/REVIEWS NONE
If any of the items below are applicable- they should be checked below and on regulatory page of IRB Online.
Forward approvals and any additional requirements from these groups to CIRB
Cancer Center Protocol Review Committee (PRC)
Institutional Biosafety Committee (IBC)
New Medical Device Form
Radiation Safety/ HIRE/ RDRC
Information Security, Policy & Records Office (ISPRO)
NA Pending Approval On file
NA Pending Approval On file
NA
NA
Pending Application
Pending Approval
On File
On file
Pharmacy Approval
NA Pending Approval On file
NA Pending Approval On file
If the CIRB approved the use of a Legally Authorized Representative have you reminded the study team that the UVa language for the surrogate consent signature section is required in the consent? NA Yes
Review comments:
Page 1 of 7
Version: 06/08/16
New Protocol Event Process:
1.
Download protocol into IRB online.
2.
Designate applicable CIRB of Record
3.
Enter Type as applicable per CIRB review type.
4.
Change status to “Open to Enrollment”
5.
Enter approval and expiration dates if approved by CIRB. These must be the same dates as the CIRB approval/expiration date. (If not yet approved, the study team is instructed to submit these dates to the
IRB-HSR within 5 days of receipt.)
Original approval date- CIRB
Last approval date- CIRB
Expiration date- CIRB
6.
Remove Next 5 Year Review date.
7.
Do not enter Last Meeting Date.
8.
DO enter Next Meeting Date
9.
Determine any HIPAA waivers to be granted and document on Regulatory page.
10.
If CIRB approval is included: enter event “Receipt of New Protocol Approval- Central IRB”, under
“Type” enter review type used by CIRB
11.
If CIRB approval is NOT included enter a “Receipt” event and include in comment section that the study team will submit CIRB approval within 5 days of receipt.
12.
Include the following language in the comment field of event:
Protocol Open to Enrollment at UVa.
IRB Authorization Agreement UVa Tracking # INSERT# on file.
If applicable: COI Management Plan sent to CIRB.
13.
Include any additional language as required in comment field of event- see “Additional Comments”
14.
Click on Regulatory button and insert any applicable comments for HIPAA Waivers.
15.
Leave AGENDA TYPE as NONE
16.
No IRB-HSR Assurance is utilized as the IRB-HSR is NOT the IRB of record.
17.
Verify all approvals from UVa applicable committees have been received and note them on the regulatory page.
18.
NeuroNEXT Protocols ONLY: Confirm approval of HIPAA and Injury language in consent and sign the NeuroNEXT form approving the language.
19.
Verify current training completion and create the Training Certificate
20.
Save all submitted documents and the Administrative Review Checklist on the U drive under Current
IRB Protocols & Consents/ ( applicable CIRB) ( applicable protocol)
21.
Upload the following documents as a PDF file into IRB Online. Insert a description of the documents uploaded with the event in the comment field.
On Versions page upload under IRB Application: o CIRB Application
Under Event “Receipt of New Protocol Approval- Central IRB” upload: o CIRB Approval
Under Event “Receipt” o Protocol Cover Sheet o Training Certification Form o Ancillary Committee approvals ( if applicable) o HIPAA Waiver documentation or HIPAA Authorization (English/ Spanish) (if applicable- and if protocol reviewed by CITN CIRB, NCI CIRB, Western CIRB) o Emails/ correspondence (if applicable) o Other
Page 2 of 7
Version: 06/08/16
ADDITIONAL COMMENTS
Does the protocol require the approval of any other UVa committee/office?
If yes, add : Other Approvals
Is this protocol funded by an external grant?
If yes, add Other Approvals
Will the IRB-HSR serve as the HIPAA Privacy Board?
If yes, add HIPAA
Does the study include sharing data/ specimens outside of the UVa HIPAA covered entity
without the written consent of the subject ? Nutrition services employees are part of UVA HIPAA covered entity .
If sending names to Center for Survey Research for health related research- answer YES
If yes, see Sending or Receiving Data and/ or Specimens to determine required steps & documentation
Does this study include Waiver of HIPAA Authorization for the main study and involve
Unaffiliated Investigators, other than Nutrition Services employees, or who has not obtained
approval from the SOM via the SOM Volunteer Form who will receive identifiable health information?
If yes, see Unaffiliated Investigator, Access to PHI, Waiver of Consent/HIPAA Authorization
Does the study involve Gene Transfer?
If yes, document in event comment field that all other required approvals are on file
Administrative Staff Completing Form at Pre-review: Date
Yes No
Yes No
Yes No
Yes No
Yes No
Yes No
Page 3 of 7
Version: 06/08/16
HIPAA
HIPAA- De-identified and / or no health information,(no consent)
HIPAA- Identifiable-External Disclosure-Tracking Required ( no consent)
Tracking instructions found at U/ IRB/IRBHSR/Administrative FAQ’s /HIPAA/ HIPAA TRACKING INSTRUCTIONS
HIPAA- Limited Data Set (no consent)
HIPAA-Identifiable-External Disclosure-Tracking Required-screening log only ( no consent for screening log disclosure)
Tracking instructions found at U/ IRB/IRBHSR/Administrative FAQ’s /HIPAA/ HIPAA TRACKING INSTRUCTIONS
HIPAA-Identifiable-Internal Use-No Tracking Required( no consent)
NOTE: change wording that is automatically populated as the IRB-HSR is not the IRB of record granting Waiver of Consent.
CONTACTING
2. Contacting: Not Health Care Provider-Waiver of HIPAA Authorization
Recruitment 2 a or b is checked. If the study involves more than one group of subjects (controls vs. non- controls, patients vs. health care providers) make it clear in the wording below- which group you are referring to if not applicable for all subjects.
This protocol has been granted [DELETE a Waiver of Consent via 45CFR46.116 (Add additional regulations as
applicable-e.g. DoD, FDA- see below) and ] a Waiver of HIPAA Authorization via 45CFR 164.512(i)(2) to contact subjects by direct contact by a person who is not their health care provider. Direct contact may include phone, letter, direct email or approaching potential subjects while at UVa. Phone, letter or emails will be approved by the IRB-HSR prior to use. The following HIPPA identifiers may be collected: Name, medical record number, date of birth and contact information appropriate to the recruitment plan. The minimum necessary PHI to be collected includes only those items related to the inclusion/ exclusion criteria.
If subjects over the age of 89 will be enrolled add For subjects over the age of 89, their date of birth and age will not be recorded. All will be recorded as >89 years of age.
[DO NOT INSERT ANY ITEMS BELOW]
1) Funded by DoD? , If yes, add and 32CFR219.117(c)
2) Involve testing of an in-vitro device? add and"FDA Guidance on Informed Consent for In Vitro Diagnostic Device
Studies Using leftover Human Specimens that are Not Individually Identifiable. "
3) and 21CFR50.23: (Tip: Includes drugs or devices- emergency use )
4) and 21CFR50.24: (Tip Includes drugs or devices ( very rare- consult with IRB Director )
Reviewer Comments:
5. Waiver of HIPAA Authorization- Main Study
Excludes a waiver for identifying /contacting.
If the study involves more than one group of subjects ( controls vs non- controls, patients vs health care providers) make it clear in the wording below- which group you are referring to if not applicable for all subjects.
If de-identified health information and if subjects over the age of 89 will be enrolled add: For subjects over the age of 89, their date of birth and age will not be recorded. All will be recorded as >89 years of age.
If PHI and LDS add : Health information meets the criteria of a limited data set. DUA sent to PI.
If PHI and Identifiable : This protocol has been granted a waiver of HIPAA authorization under 45CFR 164.512(i)(2) for the main study. The following HIPAA identifiers will be collected: INSERT.
The minimum necessary PHI to be collected includes INSERT
Subjects may not be contacted by any method (email, phone, in person etc.) to obtain more information for this study without additional IRB-HSR approval.
No identifiable health information will be taken or shared outside of the UVa HIPAA covered entity.
Page 4 of 7
Version: 06/08/16
8.
Waiver of HIPAA Authorization-Questionnaires
PICK ONE: Identifiable health information will not be collected in this study . OR if includes identifiable health information add
This protocol has been granted an alteration of HIPAA Authorization under 45CFR164.512(i)(2) to obtain oral HIPAA authorization for questionnaires. The IRB determined that obtaining written HIPAA authorization would be impracticable because : insert
9.
Waiver of Documentation of HIPAA Authorization-Main Study
, PICK ONE: Identifiable health information will not be collected in this study . OR if includes identifiable health information add
This protocol has been granted a alteration of HIPAA Authorization under 45CFR164.512(i)(2) to obtain oral HIPAA authorization for the main study. The IRB determined that obtaining written HIPAA authorization would be impracticable because : insert .
Page 5 of 7
Version: 06/08/16
OTHER APPROVALS
RSC If required- add the following to the approval comment field
Radiation Safety Committee approval on file.
HIRE If required- add the following to the approval comment field
HIRE Committee approval on file.
If required- add the following to the approval comment field
SOM CTO approval on file for PI held PICK ONE IND /IDE.
SOM-CTO
PI held IND or
IDE
SOM-CTO
PI of Multisite Trial
SOM-CTO
Review regarding
SR/NSR status
SOM-CTO
Review regarding need for IND
SOM-CTO
Review regarding
IND/IDE held by outside PI
SOM CTO-
Outside academic investigator serving as Sponsor
PRC
If required- add the following to the approval comment field
SOM CTO approval on file for PI of multisite trial.
If required- add the following to the approval comment field
SOM CTO review on file regarding SR/NSR status. Their opinion is (INSERT). Full IRB to determine if device is
SR or NSR. If SR, an IDE will be required.
IRB may consult with SOMCTO regarding IDE exempt status, but this is not required.
If required- add the following to the approval comment field
SOM CTO determined an IND is PICK ONE required/ not required.
If required- add the following to the approval comment field
For studies involving investigational device enter:
SOM CTO review on file regarding need for an IDE. Their opinion is (INSERT). Full IRB to determine if device is SR or NSR. If SR, an IDE will be required.
For studies involving an investigational drug enter:
SOM CTO determined an IND is PICK ONE required/ not required.
If required- add the following to the approval comment field
SOM CTO review of sponsors’ protocol on file as outside academic investigator is serving as sponsor.
IBC#
If PRC exemption provided enter:
PRC exemption on file.
If PRC approval is required- add the following to the approval comment field
PRC approval on file.
If there is a PRC approval, the version date listed on the PRC approval for the IRB protocol may not match the final version date. If the version date changes following the pre-review, add the following statement to the approval: Note: the version date of the protocol approved by the PRC is X. Additional changes resulted from the
IRB’s administrative review. The final version date of the protocol is X.
Check PRC approval form to verify if the PRC will review modifications. If yes, document on regulatory page.
If an IBC# is required- add the following to the approval comment field
IBC# (INSERT NUMBER) on file.
IBC Approval IBC approval for use of hazardous/toxic material in this protocol
ISPRO
Departmental
Scientific
Review
Committee
Gene Transfer
Study
Pharmacy
Approval
If PRC approval is required- add the following to the approval comment field
ISPRO approval on file.
If required- add the following to the approval comment field
Departmental Scientific Review Committee approval on file.
Add the following to the approval comment field
Approval from SOM CTO, IBC and RAC committee on file. IBC# (insert #) on file.
Protocol may be opened to enrollment once RAC committee approval is obtained.
Add the following to the approval comment field
Approval from Pharmacy on file.
Page 6 of 7
Version: 06/08/16
Grant
For grant held by UVa faculty member: add the language below into the assurance form
The grant(s) funding this protocol [GIRB#(s) INSERT NUMBER ] has/have been reviewed by the IRB-HSR.
The IRB-HSR and the PI attest that the research in this protocol is consistent with the grant application(s)/proposal(s) funding this research.
For grant held by UVa faculty member: Add the following statement to the comment field on the main page.
UVa funding for study coming via sub-contract from (INSERT NAME OF INSTITUTION) which holds the grant with (INSERT
NAME OF SOURCE OF FUNDING)
Unaffiliated Investigator, Access to PHI, Waiver of HIPAA Authorization
If yes, complete section below and add language to assurance form
Does the work being done by the unaffiliated investigator meet the criteria for Waiver of HIPAA authorization?
Yes No
(A) The use or disclosure of protected health information involves no more than minimal risk to the privacy of individuals, based in, at least, the presence of the following elements:
(1) An adequate plan to protect the identifiers from improper use and disclosure;
(2) An adequate plan to destroy the identifiers at the earliest opportunity consistent with conduct of the research, unless there is a health or research justification for retaining the identifiers or such retention is otherwise required by law; and
(3) Adequate written assurances that the protected health information will not be reused or disclosed to any other person or entity, except as required by law, for authorized oversight of the research study, or for other research for which the use or disclosure of protected health information would be permitted by this subpart.
(B) The research could not practicably be conducted without the waiver or alteration and
(C) The research could not practicably be conducted without access to and use of the protected health information
IF NO, do not complete any additional info on this page. Go to section entitled: Waiver of Documentation of
Consent/alteration of HIPAA Authorization.
IF YES, insert ALL of the following statements into the Comment Field of the Event .
This protocol has been granted a waiver of HIPAA authorization under 45CFR 164.512(i)(2) for the work being done by the unaffiliated investigator.
The following HIPAA identifiers will be shared with the unaffiliated investigator:
The PHI, deemed to be the minimum necessary to share with the unaffiliated investigator includes
Study team must track disclosures to the Unaffiliated Investigator in EPIC.
On Regulatory Page mark the following:
HIPAA- Identifiable-External Disclosure- Tracking Required (no consent)
Page 7 of 7
Version: 06/08/16