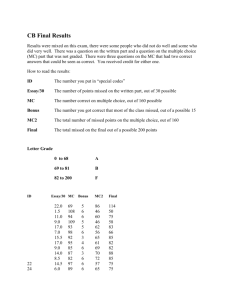
Year 1 Medical Adherence Chart
advertisement

SUNDAY MONDAY TUESDAY WEDNESDAY THURSDAY FRIDAY SATURDAY Late Late Late Late Late Late Late Missed Late Missed Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Late Missed T1 T2 T3 T4 T5 T6 Late Late Missed Missed Late Late Missed Late Missed Late Missed Late Missed Late Missed Missed Missed T1 T2 T3 T4 T5 T6 Late Missed Missed Late Missed Missed Missed Late Missed T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 Late Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 Missed T1 T2 T3 T4 T5 T6 Late Missed Late Missed Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 Missed T1 T2 T3 T4 T5 T6 Late Missed Late Missed Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Late T1 T2 T3 T4 T5 T6 Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Late Late Missed Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Missed T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 T1 T2 T3 T4 T5 T6 Missed Missed each ofAssociation these times? Timeofofbed # of 1 = get in/out 4 = work Changed? Meds 2 = meal day 5 = other (specify) T13 = regular interval T2 Time of Association? # T3 day T4 T1 T5 T2 T6 T3 T7 T4 T8 T5 Total T6 Total 4. 3. Late T1 T2 T3 T4 T5 T6 Patient ID: ____________________ Date: ___________________________ 1. How many times a day do you take 1. In the past 30medications, days, has there been a prescription including change in the number of prescription pills, inhalers, drops, liquids on a medications regular basis?or doses of a particular medication that you have been taking? No meds 1 NO (0) YES (1) 2 2. How3many times a day do you take prescription medications, including 4 pills,5inhalers, drops, patches, injections or liquids on a regular basis? 6 7 0 1 2 3 4 5 6 8 3. How many medications do you take at thesemedications times? 2. each How of many do you take at Missed 5. Are sidecause effects from any of or your Did there anything you problems medications that cause you to either difficulties in taking your medications? miss a dose or take it late? No No Yes, Yes, _________________________ _________________________ _____________________________ Do you use anything or anyone to help you take your medications? 0 = nothing 1 = pill box 2 = alarm / beeper 3 = checklist / log 4 = household member 5 = DOT (professional) 6 = other _______________________