Young Mens Sexual
AND
Reproductive Health
Toward a National Strategy
FRAMEWORK AND
RECOMMENDATIONS
Freya L. Sonenstein, editor
URBAN INSTITUTE
Urban Institute
2100 M Street, NW
Washington, DC 20037
Phone: (202) 261-5709
Fax: (202) 728-0232
E-mail: paffairs@ui.urban.org
http://www.urban.org
This report is available on the
Urban Institute Web site or by calling the
Urban Institute Office of Public Affairs
at (202) 261-5709.
The views expressed in this report are those
of the author and do not necessarily reflect those
of the Urban Institute, its sponsors, or its trustees.
' Urban Institute, 2000
2 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
A C K N O W L E D G M E N T S
This report was prepared with support from the Office of Population Affairs, U.S.
Department of Health and Human Services. Many individuals contributed to its
development. In particular, the working group would like to acknowledge the
able research assistance provided by Karen Alexander and Stacey Phillips and
the meeting support provided by Sonja Drumgoole and the staff at Airlie House
in Airlie, Virginia. In addition, program administrators attending a workshop at
the Male Advocacy Network meeting in New Orleans, November 8 10, 1999,
provided many examples of how organizations could achieve the five program
objectives for promoting young mens sexual and reproductive health. Their
suggestions are reflected in the framework presented for comprehensive program approaches.
3
4 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
D E A R
R E A D E R
,
The comprehensive health promotion effort presented here is a starting
point for building a broader consensus about the value of enhancing the reproductive health of young men. It reflects the consensus of a working group of
experts representing the major professional groups with leadership roles in this
important policy area.
In this report we document the need for a broad new initiative to promote
This is a particu-
the sexual and reproductive health of young men, offer a comprehensive
larly opportune
strategy to meet that need, identify the essential components of services that
and critical time
must be delivered, and recommend specific actions that can and should be
to launch a
taken immediately by community service providers and by federal agencies,
in particular the Department of Health and Human Services (DHHS), to
comprehensive
health promotion
implement the new initiative.
The framework and recommended actions were developed by an interdisciplinary working group of experts, whose names and affiliations are listed on the
following pages. They participated in a two-day working session at Airlie House
initiative to
address the unmet
in Virginia, September 28 29, 1999. The meeting was convened by the Urban
reproductive and
Institute to address the lack of consensus about the scope, content, and delivery
sexual health needs
of reproductive health services for young men in the United States today. During
the session, a group consensus developed about the need for a broad new ini-
of young men.
tiative to promote the reproductive and sexual health needs of young men and
the key elements of such an initiative. The papers prepared for the meeting form
the foundation for the recommendations presented here. These papers were
subsequently revised into chapters in a companion volume, Young Mens
Sexual and Reproductive He a l t h Toward a National Strategy: Getting Started.
Freya Sonenstein, editor
5
Y OUNG M EN S S EXUAL AND R EPRODUCTIVE
H EALTH W ORKING G ROUP
*Bruce Armstrong, D.S.W.
Associate Clinical Professor
Heilbrunn Center for Population
and Family Health
Columbia University
Mailman School of Public Health
New York, N.Y.
David L. Bell, M.D., M.P.H.
Assistant Clinical Professor &
Medical Director of Young
Men’s Clinic
Heilbrunn Center for Population
and Family Health
New York Presbyterian Hospital
New York, N.Y.
*Claire Brindis, Dr.P.H.
Professor, Department of
Pediatrics,
Division of Adolescent Medicine,
& Director, Center for
Reproductive Health Research
and Policy
University of California–San
Francisco
San Francisco, Calif.
K.D. Burkett
Project Director
Legacy Resource Group
Carlisle, Iowa
*Obie Clayton, Ph.D.
Professor of Sociology &
Director, Morehouse Research
Institute
Morehouse College
Atlanta, Ga.
Alwyn T. Cohall, M.D.
Director, Harlem Health Promotion
Center
Associate Professor of Clinical
Public Health and Pediatrics
Columbia University
Mailman School of Public Health
Division of Sociomedical Sciences
New York, N.Y.
Barbara Cohen
Policy Analyst
Office of Population Affairs/Office
of Family Planning
Bethesda, Md.
Jonathan M. Ellen, M.D.
Assistant Professor of Pediatrics
Division of General Pediatrics and
Adolescent Medicine
Johns Hopkins University School
of Medicine
Baltimore, Md.
*Arthur Elster, M.D.
Director, Clinical and Public
Health Practice Outcomes
American Medical Association
Chicago, Ill.
Shawn Gibson, M.H.S.
Director
Adolescent Programs
Family Planning Council
Philadelphia, Pa.
6 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Irvienne Goldson
Education and Training Manager
Health Services Department
Action for Boston Community
Development
Boston, Mass.
Bill Gruchow, Ph.D.
Director
Institute for Health, Science and
Society
University of North Carolina at
Greensboro
Greensboro, N.C
Tamara Kreinin, M.A.
Director of State and Local
Affairs
National Campaign to Prevent
Teen Pregnancy
Washington, D.C.
Laura Lindberg, Ph.D.
Senior Research Associate
The Urban Institute
Washington, D.C.
*Dorothy Mann
Executive Director, Family
Planning Council
Philadelphia, Pa.
Sue Moskosky, M.S., RNC
Deputy Director (Acting)
Office of Population Affairs/
Office of Family Planning
Bethesda, Md.
Edward W. Pitt, M.S.W.
Senior Researcher & Co-Director
The Fatherhood Project
Work and Families Institute
New York, N.Y.
Director
Population Studies Center
The Urban Institute
Washington, D.C.
Laura Porter
Research Associate
The Urban Institute
Washington, D.C.
Sam Taylor
Acting Director
Office of Family Planning/Office
of Population Affairs
Bethesda, Md.
Cory L. Richards
Vice President for Public Policy
The Alan Guttmacher Institute
Washington, D.C.
*Jerry Tello, M.S.
Director, National Latino
Fatherhood and Family Institute
Los Angeles, Calif.
Felicity Skidmore, M.A.
Senior Research Editor
The Urban Institute
Washington, D.C.
Freya Sonenstein, Ph.D.
Jennifer Todd, Dr.P.H.
Research Fellow
Office of Family Planning/Office
of Population Affairs
Bethesda, Md.
Kathleen M. Woodall, B.S.N.,
ARNPC
Director of Regional Operations
U.S. DHHS/OPHS
Office of Population Affairs/
Office of Family Planning
Bethesda, Md.
* steering committee
7
C ONTENTS
I NTRODUCTION .................................................. 11
The introduction provides the context for the recommended health promotion
effort. It explains why the focus needs to be on young men, the federal context
of the proposed effort, and the source of the recommended initiative.
R ATIONALE
FOR
A CTING N OW .......................... 14
Section one provides the rationale for launching a new initiative now to promote young mens sexual and reproductive health. It describes the extent of
unmet reproductive health needs of these young men and examines the reasons for their neglect. It documents the confluence of key demographic, policy,
and service shifts that makes this a particularly opportune time to take action.
W HAT N EEDS
TO
B E D ONE .............................. 24
Section two offers the groups consensus on what needs to be done to overcome existing barriers to promoting young mens reproductive health. It
explains the importance of placing young mens reproductive and sexual
health within the broader context of adolescent development, offers a new definition of what constitutes sexual health, and develops a broad strategy to
attain that vision. It identifies five key goals that must be met by a combination
of services to effectively promote young mens reproductive health, and it
explains how key elements of the strategy relate to these goals.
8 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
R ECOMMENDED C OMMUNITY AND
F EDERAL A CTIONS ............................................ 32
The third section focuses on the implementation challenges and opportunities
facing community service organizations and the relevant federal agencies, particularly DHHS. Specific recommendations suggest how to improve the capacity of communities and federal agencies to address the reproductive and sexual health concerns of young men.
B ENEFITS
OF A
N ATIONAL E FFORT
.................. 42
The final section addresses the question of who benefits from expanding efforts to
promote the sexual and reproductive health of young men. It suggests that, because
of the universal value of this effort, the U.S. Surgeon General and DHHS take the
lead to promote the dialogue and program experimentation required to ensure that
these needs are addressed.
9
Introduction
W HY F OCUS
H
ON
Y OUNG M EN ?
uman reproduction involves a man and a woman. In spite of this
fact, efforts to improve reproductive health in the United States and
elsewhere have typically targeted women.1 But since men partici-
pate in sexual decisions and behavior associated with reproduction, the focus
here is on the sexual and reproductive health of men in the United States and
specifically on young men ages 12 to 24. While reproductive health is a concern for all men of all ages, the earliest part of the life course adolescence
and early adulthood is of utmost importance. Promoting the sexual and
reproductive health of young men is a keystone to enhancing their health
overall, to reducing some of the major health risks they face, and to establishing habits that will protect them throughout their lives. Promoting sexual and
reproductive health for young men, a population that has been largely
ignored, can lead to new inroads in promoting healthier lifestyles, preventing
disease transmission, and reducing the unplanned pregnancies and births
that are implicated in poor outcomes for children.
F EDERAL C ONTEXT OF H EALTH
P ROMOTION E FFORT
Making sexual and reproductive health an integral part of a broader health promotion effort for young men is consistent with the Surgeon General s Evolving
Health Priorities. It also will contribute to achieving the health goals established
for the nation in the Healthy People 2010 initiative.2 The initiative designates
responsible sexual behavior as one of 10 leading health indicators for the nation,
reflecting its status as a major public health concern as well as its amenability to
change. The initiative targets the behavior of both men and women. But there is
no traditional medical or public health infrastructure oriented to the sexual and
reproductive health needs of men. Addressing these needs will require the
development of new approaches and new partners for effective community
health strategies. Such an effort can serve as a catalyst and model for other
broad-based community health partnerships. Community partnerships are an
important component of the Surgeon General s strategy to build a health system
that balances treatment with disease prevention and health promotion.3
Reaching out to young men is not a new idea. The Office of Family Planning
of DHHS funded a set of demonstration projects to encourage the involvement
of men in the 1970s. The Office of Family Planning was established to administer Title X of the Public Health Services Act, to assist individuals and couples
with the number and spacing of their children. Title X s federal family planning
program, now a network of 4,600 family planning clinics, has grown and thrived
for 30 years. In sharp contrast to this success, its early demonstration program
designed to test the involvement of men in family planning clinics showed limited success and was discontinued.
The Title X program has now renewed its efforts to involve men, testing a
variety of approaches to including men in promoting reproductive health.
These approaches range from expanding family planning clinics services for
men to using community-based organizations already serving young men as
venues for delivering reproductive health services. But lack of consensus
about what reproductive health services for young men should look like and
how this undefined complement of services should be delivere d p resents an
enormous challenge.
12 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
S OURCE
OF
P ROPOSED I NITIATIVE
To help overcome this barrier, the Urban Institute convened a group of experts
representing the major professional groups that could provide leadership for the
development of reproductive health services for young men in the United States
today. This group, whose names and affiliations are listed on pages 6 7, met for
a two-day working session at Airlie House in Virginia on September 28 29, 1999,
Lack of consensus
to review a set of working papers prepared for the meeting.4 The broad strategy
about what repro-
and recommended actions presented here reflect the consensus developed by
the participants at this meeting. The suggestions are grounded in part on the
discussions held and on the information and analyses contained in the papers
prepared for the meeting.
The following pages describe why the time is right for an initiative promoting young mens sexual and reproductive health, why it is so important, how it
might be done, and how DHHS can help make it happen. The working groups
blueprint for action is presented as a starting point for building a broader con-
ductive health
services for young
men should look
like presents an
enormous
challenge.
sensus about the value of enhancing reproductive health among young men
and for shaping promising intervention strategies.
Introduction
13
Rationale for Acting Now
R
ecognition of mens crucial contribution to the healthy formation of
families has increased remarkably over the past five years. This new
awareness is apparent in the public policy realm, among service
providers across the country, and among young men. The interest and energy of
policymakers and service providers combined with the evident readiness of the
men themselves make this moment particularly favorable for a new initiative
promoting young mens sexual and reproductive health.
R ECENT P OLICY S HIFTS
More men than ever before are fathering children outside marriage and living
apart from their children.5 Recognition of these demographic shifts, and their
consequences for children who grow up without the economic or emotional support of their fathers, has led American lawmakers to require more men to take
greater responsibility for their children, even when those children are unintended or are born outside marriage. Key elements of the nations welfare reform policy set
forth in the Personal Responsibility and Work Opportunity
Reconciliation Act (PRWORA) of 1996 discourage childbearing outside marriage, encourage abstinence until marriage, and step up efforts to link unmarried
fathers with their biological children through establishment of paternity and
enforcement of child support. A clear intent of this legislation, signaled by the
name of the bill itself, is to encourage responsible behavior.
These legislative efforts parallel national campaigns and state and local programs that encourage men to get more involved with their families. Private initiatives range from faith-based campaigns to noncustodial fathers rights groups to
programs aimed at shoring up fragile families.6 On the public side, the federal government has implemented the president s 1995 memorandum to the heads of
executive departments, which directs federal agencies to support the role of
14 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
fathers in families.7 And every state now has an initiative under way to encourage
responsible fatherhood.8 At the individual level, attitudes about the father s role in
the family have shifted, with increasing emphasis on his role as caregiver and nurturer, as well as breadwinner.9
Other more recent efforts are beginning to help men avoid unintended parenthood and become more active in choosing when to become fathers.10 This is,
indeed, the first step in becoming a responsible father.11 The past few years have
brought many calls to include men in family planning strategies ranging from
Recognition of
12
conclusions of the Institute of Medicine, to the U.S. DHHS National Strategy to
Prevent Teen Pregnancy,13 to the deliberations of the 1994 International
men s crucial
Conference on Population and Development in Cairo and the 1995 Fourth
contribution to
World Conference on Women in Beijing. Thus, there is now general support for
the healthy
the goal of increasing mens participation in preventing unintended pregnancy.
formation of
However, the type of male involvement, how the objective is to be attained, and
how to pay for it are not yet clear.
There also is new interest and investment in identifying successful prevention programs, so that they can be more broadly implemented throughout the
United States. These efforts range from rigorous reviews of the evidence about
effective teenage pregnancy prevention programs conducted by the Centers for
Disease Control and Prevention and the National Campaign to Prevent Teen
families has
increased
remarkably
over the past
five years.
Pregnancy14 to efforts to identify what makes HIV prevention programs succeed,
especially community-based initiatives.15 Responding to criticism that no abstinence-only programs had undergone rigorous evaluation, Congress included
funding in its 1996 welfare reform legislation for a scientifically conducted evaluation of the new abstinence-only programs. This evaluation is under way.
While there is still more to learn, the reproductive health field is better equipped
than before to take advantage of the accumulating knowledge about what programs and program elements work.
Rationale
15
R ECENT S HIFTS
IN
E XISTING S ERVICES
Many family planning clinics around the country are finding new reasons to
serve the male partners of their customary female clientele. A key concern has
been the emergence of HIV and other sexually transmitted diseases (STDs) as
major public health problems. Some clinics are discovering, for example, that
breaking the cycle of reinfection requires them to treat the partners of the many
women who test positive for STDs. The appearance of HIV and rising rates of
STDs among their patients also have given clinics a more urgent interest in
encouraging use of condoms, a contraceptive method that had languished during the 1970s as medical methods like the pill were increasingly the method of
choice.16 Since 1979, condom use among adolescent men has more than doubled, and male condoms are now used more than half the time when teenagers
have sex for the first time.17
The health care market is also putting new pressures on family planning
clinics. Some clinics have sought to expand their clienteles. Some now offer a
broader array of care for the whole family, including job and sports physicals as
well as reproductive care STD testing and treatment, sterilization, fertility
counseling for men. Other clinics forged partnerships with youth development and criminal justice agencies to provide reproductive services to underserved populations in these nontraditional venues.
Efforts of family planning clinics to serve men have grown substantially. In a
1995 survey of publicly funded family planning agencies across the country, 39
percent reported that some of their patients were men, and more than half (52
percent) of Planned Parenthood affiliates include male partners in education and
counseling efforts.18 These efforts serve relatively few male clients overall, however. At the federal level, the Office of Family Planning is funding 30 projects to
test new approaches to involving males in family planning. Some states also are
16 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
funding family planning services for men. California has one of the most comprehensive efforts, which includes funding by the state Office of Family Planning
for 22 community-based agencies to develop and implement male involvement
programs. A 1999 report issued by the Family Planning Councils of America,
highlighting efforts in 10 states,19 calls meeting the reproductive health needs of
men in our communities one of the best-kept secrets of Title X.20
The past five years also have brought rapid growth in programs promoting
mens involvement in families. The National Fatherhood Initiative reports more
than 2,000 fatherhood programs across the country. Programs that include
reproductive health promotion are more scarce. In 1995, about 100 such programs aimed at teenage and young adult men were identified across the coun-
There is
now general
support for
the goal of
try, and many were less than three years old.21
The field of male sexual and reproductive health is emergent. Much pioneering activity and enthusiasm are evident, not only among more traditional providers
increasing men s
participation in
but also among the community-based agencies that often hold the trust of young
men, particularly those disconnected from the mainstream. The next steps are to
preventing
define the content of services, identify successful program models through inven-
unintended
torying program approaches, identify best practices, promote further innovation
pregnancy.
and partnerships, and invest in program evaluation for best bets.
R ECENT P OSITIVE C HANGES
AMONG
M EN
National surveys asking about mens attitudes and behaviors regarding sex,
contraception, pregnancies, and births reveal that young men and women are
still at high risk of unintended pregnancy and disease.22 The same surveys also
show, however, that in recent years teenage men have begun to behave more
cautiously in their sexual lives. Many of these men are highly motivated to use
condoms and have dramatically increased their use of condoms since 1979.
Rationale
17
In addition, they have modestly cut back their levels of sexual activity since
1988. These two, in turn, have reduced the proportions of teen males who have
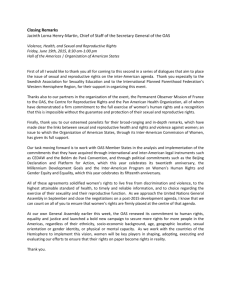
had unprotected sexual intercourse in the past year. Still, the share of young
men engaging in unprotected sexual intercourse remains high, and it is especially high among men of color. In 1995, just over one-fourth (27 percent) of all
male teenagers reported having unprotected sex in the past year, but the proportions were substantially higher among African-American (40 percent) and
Hispanic men (37 percent).23
Levels of Protection in the Last 12 Months against HIV/STDs
among Never-Married Males Ages 15 to 19, by Race/Ethnicity, 1995
100%
80%
23%
37%
39%
21%
60%
5%
40%
35%
16%
9%
7%
39%
20%
0%
Black
White
100% CONDOM USE
NO SEX IN LAST YEAR
51%
20%
SOME UNPROTECTED SEX*
Hispanic
* Does not include 100% effective female contraception.
Numbers do not sum to 100 due to rounding.
Source: Urban Institute 2000
18 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
NO SEX EVER
PARALLEL S HIFTS
IN
H EALTH O UTCOMES
As sexual risk-taking by adolescents declines, their health improves. National
population data show declines in adolescent pregnancy and childbearing.24
Disease surveillance data indicate that some STD rates among adolescents also
have declined.25 These declines, combined with the shift in health behaviors at
the same time, strongly suggest that public health efforts to educate teenagers
and the public at large about the dangers of HIV, other STDs, and unintended
pregnancy are beginning to pay off. Even so, AIDS is the seventh leading cause
26
of death among men ages 15 to 24,
and the physical, social, and economic
costs of other STDs and unintended pregnancy remain great.
But adolescent men the targets of much of the public effort and rhetori c
are not the age group with the greatest reproductive health risk. Young men in
their early 20s actually face greater risks. They have sexual intercourse more often
and use condoms less often (see chart on next page). One-third of unmarried
Reducing
sexual risk-taking
among young adult
men...is an
important strategy
for reducing high
sexually experienced men ages 22 to 26 have had three or more female sexual
rates of STDs and
partners in the past year, compared with one-fifth of unmarried, sexually experi-
childbearing
enced men ages 18 and 19.27 Not surprisingly, rates of STDs are also higher
among female
among men in their 20s. In 1998, the gonorrhea rate was 575 per 100,000 among
men ages 20 to 24, compared with a rate of 355 among men ages 15 to 19.28
teenagers.
These behavior patterns among men in their early 20s affect the health of
female adolescents, because such men father most births to teenage girls. In
1988, 51 percent of births to girls ages 15 to 19 were fathered by men ages 20 to
24, for example; another 11 percent were fathered by men ages 25 to 29.29 More
generally, sexual relationships between teenage girls and older partners tend to
be riskier than those between teen girls and their male peers, because use of contraception is lower with older male partners (Miller, Clark, and Moore 1997).30
Among females, some STD rates peak among 15- to 19-year-olds, while among
Rationale
19
Sexual Risk Behaviors among Young Men, by Age
%
Condom
Use
100%
100
80%
80
60%
60
40%
40
20%
20
0%
Number of Times
Had Sex in Last
Year
0
15–17
18–20
21–23
24–26
Source: Urban Institute 2000
males they peak among 20- to 24-year-olds. Thus, reducing sexual risk-taking
among young adult men, as well as their sexual involvement with teen women
generally, is an important strategy for reducing high rates of STDs and childbearing among female teenagers.
E XTENT OF U NMET R EPRODUCTIVE
H EALTH N EEDS OF M EN
Young men need more reproductive health information and services than they
are getting. First, though in recent years young men have reduced their sexual
risk-taking, more change is needed to protect them and their partners from
AIDS, other STDs, and unintended or too early pregnancies and births.
Second, young men report that they want more information about reproductive health issues than they receive. Parents often do not provide teens with
20 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
the help they need. Only half of teen men, for example, say they have spoken
to their parents about a reproductive health topic.31 In addition, many opportunities for educating young men through school, family, the media, and
health care professionals are missed. Third, many young men do not have
access to preventive care or treatment. Together, these problems leave young
men in need of much greater access to information and services that could
enhance their reproductive health.
Most male teenagers (71 percent) had a physical exam in the past year. Yet
relatively few report getting information about reproductive issues from their
health care providers. Less than one-third (31.5 percent) of the group who had a
physical reported discussing even a single reproductive health topic with their
doctor or nurse (Porter and Ku 2000). A smaller proportion of men in their 20s
(56 percent) had a physical exam in the past year, although a similar proportion
(31 percent) of those who had been examined discussed reproductive health
issues with a doctor or nurse. Their lower overall contact with health providers
reduces the overall proportion of men in their 20s who receive reproductive
health information from this source.32 Many of those providers miss prime
opportunities for addressing reproductive health risks, like STDs, among this
generally healthy population. And many men lack access to care altogether.
R EASONS FOR I NADEQUATE A CCESS
C ARE AND I NFORMATION
TO
H EALTH
The absence of health insurance is a major stumbling block to access to care. The
same survey that found that almost three-quarters of males ages 15 to 19 received
a physical exam in the past year found that fewer than half of the 11 percent of
males without health insurance received a physical exam.33 Among men ages 22
to 26, regardless of insurance status, only 56 percent received a physical exam in
Rationale
21
the past year.34 Access to health care providers must be expanded, and the sexual and reproductive health content of these services must be improved.
Aggravating the situation for most young men is the absence of any special
setting where they can go to seek gender- and age-appropriate reproductive and
sexual health services. The nature of routine care generally differs for men and
women. Reproductive health and family planning care are much more common
for young women. No comparable system ensures that young men receive
reproductive and HIV/STD-related preventive health services. Some family
planning clinics are not able to meet the reproductive and sexual health needs
of young men and are generally perceived as not very welcoming to men.
Further, education and training materials on mens reproductive and sexual
health are limited.35 In 1998, out of the 4.4 million family planning users served
by Title X clinics, approximately 3 percent were men (116,584). This number
does not include STD and HIV tests (144,608) funded by Title X for male clients.
If these tests were added, the number of men served might double but it would
still represent a small share of the clientele.36 While Medicaid and Title X pay for
the overwhelming majority of sexual and reproductive health care for lowincome women, no such recognized funding source is routinely available to
low-income men.
The medical specialties most pertinent to mens sexual and reproductive
health needs are urology and infectious diseases. However, few young men see,
or need to see, these specialists. Primary care physicians such as pediatricians
(including adolescent medicine), family practitioners, and internists provide the
bulk of care to young men. As previously noted, many of these providers fail to
respond to young mens sexual and reproductive health needs even though the
American Medical Association,37 the Society for Adolescent Medicine,38 and a
special commission sponsored by the Health Resources and Services
Administration and the Health Care Financing Administration39 recommend
22 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
that specific reproductive health services, counseling, and education be incorporated into routine care for adolescents. No medical or public health specialty
responds comprehensively to sexual and reproductive health needs of young
men, especially those beyond adolescence.
The lack of access of adolescents and young men to preventive health care
in general, and to sexual and reproductive health care in particular, causes problems that can deepen over their lifetime. A recent survey commissioned by the
Commonwealth Fund found that among adult men, one in four had not seen a
The lack of access
of adolescents and
physician in the past year, fewer than one in five said they would seek immedi-
young men to
ate medical care if they were sick or in pain, and one in five said they were not
preventive health
comfortable discussing their feelings with a doctor. Among men ages 50 and
care causes
older, 41 percent had not been tested for prostate cancer.40 Thus, few adult men
develop health-seeking behavior in their youth that will protect their health,
including their sexual and reproductive health, in their later adult years.
problems that can
deepen over their
lifetime.
Rationale
23
What Needs to Be Done
M
ost young men move from adolescence into adulthood with inadequate information about sex, little guidance about their sexual
responsibilities and relationships, and little access to appropriate
health care. Filling these gaps is a challenge that cannot be met with a single model.
P LACE R EPRODUCTIVE N EEDS
L IFE C YCLE C ONTEXT
IN
To understand how young mens reproductive health needs vary, those needs
must be placed within the broader context of adolescent male development.
Adolescence is generally divided into three phases early, middle, and late.
Although the phases have distinct and recognizable characteristics, young men
pass from childhood into adulthood at different speeds, and their place along
this path influences their needs and their abilities to address their reproductive
health at different ages.
Early adolescence which is typically ages 12 to 14 but can be earlier or
later is marked by the onset of puberty. Middle adolescence around ages 15
to 16 manifests a strong orientation to peers. Late adolescence beginning
typically at age 17 ends with the transition to adulthood, marked by some
combination of taking on adult work roles, marriage, or fatherhood.
The age at which the transition from late adolescence to adulthood actually
occurs is difficult to pinpoint. In many communities, the transition may not be
complete until the mid-20s, as young men only slowly gain the maturity and selfsufficiency to assume their role as an adult. Lack of economic opportunity may further slow this transition, because financial self-sufficiency is often considered one
of the marks of a man. At the other extreme, absent fathers, family stress, and some
peer relationships may cause younger teens to take on adult roles before they are
ready. Adolescent fatherhood may force even younger adolescents into adult roles.
24 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Because adolescence is a period of substantial developmental change, it is
both unrealistic and inappropriate to have a single set of health goals for all
young men.41 This has grown even more true as the time most young men spend
between puberty and marriage has increased, creating wider variation in their
sexual experience. For younger adolescents, reproductive health goals might
focus on delaying the onset of sexual activity. For older adolescents, it may be
necessary to focus more on protection from the potentially negative consequences of sexual activity.
Differences in the types of relationships with partners also must be taken into
account. Some young men have long-term monogamous relationships, some
engage in serial monogamous relationships, some have many partners, and
some have sex only once in a while. Each pattern requires different approaches
to promoting healthy behavior and protecting young men and their partners.
This range of experience points to the importance of a client-centered approach
to the delivery of services.
U NDERSTAND M ULTIPLE
R ISK -TAKING OF Y OUNG M EN
One final point about context: Efforts to reduce sexual risk-taking must recognize that adolescent men who experiment with sexual risk-taking are likely to
be taking other risks as well. Many studies have noted a disturbing clustering
of risk behaviors, such as sexual behavior, substance use, and violence, among
adolescents.42
According to one recent study, more than four out of five male 7th- to
12th-grade students engaging in unprotected intercourse also participate
regularly in one or more additional health risk behaviors. These include regular tobacco use, regular alcohol use, regular binge drinking, marijuana use,
What Needs to Be Done
25
other drug use, weapon carrying, physical fighting, and suicidal thoughts or
attempts.43 Particularly troubling in the context of sexual risk is the tendency
to combine sexual activity and substance use. One in five young men report
having been drunk or on a drug high the last time they had intercourse.44
More generally, a growing body of research is finding an association between
substance use and a variety of sexual risk behaviors nonuse of condoms,45
multiple partners,46 earlier initiation of sexual activity,47 casual sex,48 trading
sex for money or drugs,49 as well as increased sexually transmitted diseases
rates.50 Clearly, adolescent males sexual risk-taking cannot be addressed in
isolation from experimentation or regular participation in other health-risk
behaviors.
E STABLISH A N EW V ISION
OF M EN S S EXUAL H EALTH
Any effort to enhance young mens sexual and reproductive health needs a clear
definition of sexual and reproductive health for young men. Because such a
definition has remained elusive ever since the unsuccessful effort in the 1970s to
include men in Title X s programmatic initiatives, the working group developed
a set of consensus goals for a comprehensive sexual and reproductive health
promotion strategy for young men.
The fundamental belief guiding this effort to define sexual and reproductive health services for men is the group s vision of what constitutes sexual
health for men.
26 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
According to this vision,
All males will grow and develop with a secure sense of their
sexual identity, an understanding about the physical and emotional
aspects of sexual intimacy, and attitudes that lead to responsible
behavior. Achieving these developmental goals will result in men
postponing sexual intercourse until they are emotionally mature
enough to manage the physical and psychological aspects of sexual
intimacy. When they have sexual intercourse it will occur with as
little risk as possible to either themselves or their partner.
To achieve these results, all young men living in communities throughout
the country need access to a range of educational, counseling, clinical, and
social support services that, in combination, fulfill five goals:
➤ Promote sexual health and development.
➤ Promote healthy intimate relationships.
➤ Prevent and control STDs, including HIV.
➤ Prevent unintended pregnancy.
➤Promote responsible fatherhood.
To attain each of these goals, the working group suggests that a comprehensive reproductive health strategy for young men must do the following:
➤ Convey necessary information.
➤ Foster skills development.
➤ Promote positive self-concept.
➤ Identify and develop positive values and motivation to act on those values.
➤ Provide access to clinical care, as appropriate.
What Needs to Be Done
27
A CCOMPLISH F IVE K EY G OALS
Below is a short summary of the types of information, skills, self-images, values and motivation, and clinical services that could plausibly accomplish each
of the five goals the working group has set for sexual and reproductive health
services for young men. The list is not meant to be all-inclusive, but rather to
serve as a starting point for discussion. The group hopes that such discussion
and other efforts will lead to modifications and extensions as consensus grows
about what the core content of such services should be. To facilitate comparative review, the summary is also reproduced in table form (see page 31).
1
PROMOTE SEXUAL HEALTH AND DEVELOPMENT. Necessary information under this goal includes normal male and female pubertal develop-
ment, social and emotional development, hygiene, and components of a
healthy lifestyle. Skills development includes working on communication and
decisionmaking skills. Promoting a positive self-concept includes coverage of
masculinity and male role identity, sexual identity, self-respect, and personal
potential. (The content of this element remains fairly constant across the five
goals.) Positive values can include respect for others, cultural appreciation,
and the importance of physical health. Access to clinical care includes regular
visits to a health provider, screening and treatment for anomalies, and referrals for other services.
2
PROMOTE HEALTHY INTIMATE RELATIONSHIPS. Information under this
goal includes stages in romantic relationships, forms of sexual expression,
and sexual coercion and violence. Skills development includes how to make
decisions about initiating sex, how to refuse unwanted sexual overtures, how to
avoid unhealthy relationships, and how to develop clear lines of communication with partners. Positive values can include the desirability of give and take in
28 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
relationships, and mutual fidelity. Clinical care includes counseling, screening
and treatment of sexual dysfunction, and identifying potential physical, emotional, or sexual abuse.
3
PREVENT AND CONTROL THE TRANSMISSION OF STDs, INCLUDING HIV.
Information to be conveyed includes knowledge of the various types of STDs,
how they are transmitted and prevented, and how they can be detected and treated. Skills development includes how to obtain and use condoms correctly and how
to negotiate with partners about safe sex, including saying no to sex and obtaining
information about the partner s HIV/STD risk status. In addition to the common
elements promoting a positive self-concept, it is also important to convey recognition of personal vulnerability to disease. Positive values can include concern for
ones own health and the health of ones partner. Access to clinical care includes
screening, counseling, and treatment provided for all STDs. It also includes facilitating access to condoms through distribution programs or other approaches.
4
PREVENT UNINTENDED PREGNANCY. Information to be conveyed
includes the biological mechanisms underlying reproduction and the
merits and side effects of various types of contraceptive methods. Men need
information about female contraceptive methods. Skills development, again,
includes how to negotiate safe sex. Because the most effective methods for
pregnancy prevention are abstinence or methods used by female partners like
hormonal contraceptives, intrauterine devices (IUDs), or sterilization, good
communication with and expressions of support to these partners are also
essential. An additional element of positive self-concept is conveying a sense of
control over one s destiny. Positive values include life goals and how childbearing fits in. Clinical services include contraceptive counseling and services,
counseling about pregnancies, and referrals for other health care.
What Needs to Be Done
29
5
PROMOTE RESPONSIBLE FATHERHOOD. Information to be conveyed
includes the specifics about the responsibilities of parents, prenatal health
and childbirth, child development, and well-child care. Skills development
includes parenting and communication skills, which contribute to stronger parent-child and father-mother relationships. It also includes other life skills needed for the fulfillment of parental roles such as doing well in school, getting and
keeping jobs, and managing finances. Promoting a positive self-concept includes
recognizing the role of nurturance. Positive values include responsible fathering
and manhood. Access to clinical services includes fertility services to have children when they are desired and the screening and treatment of infertility.
D ELIVER S ERVICES E FFECTIVELY
To be effective, the mechanisms through which this content is delivered need to be
varied and extremely flexible. Four major channels provide the most effective ways
to reach young men: education, counseling, clinical services, and various support
services. The rationales for the first three are relatively obvious. The rationale for the
fourth, support services, may need to be spelled out. The environment in which a
young man is raised, the people with whom he has contact, and the opportunities
and challenges of life presented to him will influence the health risks he faces and
his sexual and reproductive decisionmaking. For this reason, enhancing the reproductive health of young men potentially necessitates not only clinical services,
health education, and counseling but also a range of support activities such as recreation, employment and training, and spiritual guidance, which promote healthy
social development, a positive self-image, meaningful interpersonal relationships,
educational attainment, and meaningful employment. In addition, a comprehensive strategy must include efforts to change the environments of young men by also
targeting policies and community norms and values for transformation.
30 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Suggested Core Content
Sexual and Reproductive Health Services for Young Men
Information
Goal 1
Goal 2
Goal 3
Goal 4
Goal 5
PROMOTE SEXUAL HEALTH AND
DEVELOPMENT
PROMOTE HEALTHY INTIMATE
RELATIONSHIPS
PREVENT AND CONTROL
STD/HIV
PREVENT UNINTENDED
PREGNANCY
PROMOTE RESPONSIBLE
FATHERHOOD
normal anatomy and pubertal
development
social and emotional
development
hygiene
STDs/HIV
where and how to
access services
nutrition
physical activity
stages in romantic relationships
readiness for sexual involvement
forms of sexual expression
sexual coercion and violence
STD symptoms and transmission
diagnosing and treating STDs
prevention strategies (including
effectiveness of condom use)
prevalence of diseases
short- and long-term consequences
of STDs (for men and
women)
where to get condoms
contraception and its effectiveness (incl. 100% effectiveness
of
abstinence)
reproductive biology and how
pregnancy occurs
where to obtain contraceptives
consequences/costs (of pregnancy/contraception)
forms of sexual expression
responsibilities of parents
prenatal health and childbirth
child development
child health and well-child care
paternity establishment, child
support, and visitation
resisting peer pressure
communication
decisionmaking
self-advocacy
risk assessment and avoidance
setting and achieving goals
communication and listening
partner selection and avoiding
unhealthy relationships
negotiating safe sex
recognizing difference between
consent and coercion
violence prevention
negotiating sexual activity and
setting limits
negotiating condom use
how to use condoms properly
communication (with partner
about sex)
how to recognize STD symptoms
how to access services
how to ask for more information
negotiating sexual activity and
setting limits
communication (with partners,
providers)
decisionmaking
how to access services/resources
resisting peer pressure
how to be intimate with partners
how to use contraceptives
how to use condoms properly
parenting skills
life skills (e.g., job, housing,
medical care, etc.)
training and opportunities for
financial self-sufficiency
communication
(child and child’s mother)
Positive
Self-Concept
self-esteem
self-respect
sexual identity/orientation
gender roles
personal potential
self-esteem
self-respect
sexual identity/orientation
gender roles
self-esteem
self-respect
awareness of vulnerability
self-efficacy
sexual identity/orientation
self-esteem
self-respect
confidence in the future
sense of control over one’s life
and decisions
self-esteem
self-respect
nurturance
sense of control over
one’s life and decisions
Values and Motivation
respect for others
spirituality
family expectations
healthy lifestyles
value of education
social responsibility
and contribution
cultural appreciation
value of healthy sexuality
healthy relationships
role expectations
mutual fidelity
health as a priority
concern for partner’s health
women’s/men’s role
in contraception
women’s/men’s role
in pregnancy
setting and achieving life goals
parenting as a life goal
values regarding parenthood/
fatherhood
values regarding “being a man”
physical exam
screening for development
abnormality
primary health care services
preventive health services
mental health assessment
access to services including
counselors (adult and peer),
mentors, health educators
physical exam
screening and treatment for
sexual dysfunction
screening and treatment for
sexual abuse
counseling (individual, relationship)
physical exam
STD testing, treatment, partner
referral
HIV testing and counseling
HIV follow-up care
counseling (safe sex)
access to condoms
physical exam
counseling (contraception,
pregnancy options)
contraceptive services
(with partner)
referral for health services
physical exam
fertility assessment
child health and well-child care
support groups for young
fathers
referral for health, mental
health,
and other services
Skills
Clinical Services
31
Recommended Community and Federal Actions
T
ypically, agencies in communities specialize in some but not all of the
types of services described in the preceding section. It is not realistic to
expect organizations to provide every service young men potentially
need. Community agencies have different capacities and will prioritize issues differently based on their community resources, their history, their mission, and how
prepared they are to engage in reproductive health services for young men. For
example, a health clinic may concentrate on integrating various areas of reproductive health, such as STD prevention and control, HIV prevention, and family planning services, but look to other organizations to gain access to (and the trust of) the
young men they need to reach. Community-based youth-serving organizations
that regularly see at-risk males may facilitate access to another organizations clinical reproductive health services for their clients. These examples demonstrate that
the initiating agency can be a clinic, a neighborhood-based youth development
organization, or some other type of community agency. The important point is that
few agencies will be able to deliver comprehensive sexual and reproductive health
services to young men alone. Partnerships across agencies are essential.
I MPORTANCE OF C OLLABORATION
C OMMUNITY O RGANIZATIONS
AMONG
Thus, to provide access to a full range of reproductive health resources for young
men, most organizations will need to reach out into their communities and create partnerships with other agencies that specialize in complementary areas of
reproductive health or service delivery modalities. Ideally, organizations can
work together to create a network of services that benefits young mens sexual
and reproductive health, maximizes reliance on community strengths and
resources, and is easily accessible by youth.
32 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
The broader the range of desired activities, the greater the need for
interaction with other organizations. Collaborative efforts will require the commitment of a wide variety of stakeholders, including young men themselves,
their partners, their families, and their communities; many different types of
nongovernmental health and social service organizations; and various sectors of
local, state, and federal government. These groups bring different types of skills,
expertise, and sensitivities to the promotion of mens reproductive health.
The desire to reach underserved populations further propels the need to
collaborate across agencies. Because health providers have traditionally found it
hard to reach young men, forming partnerships with other community organizations that have longstanding experience working with young men is a prom-
The desire to
reach underserved
populations further
ising strategy for them. Alliances with organizations offering activities that are
propels the need
especially attractive to young men, such as sports or job preparation, can be a
to collaborate
good approach to recruiting young men into health promotion and care servic-
across agencies.
es. Collaborating with agencies that have captive populations of particularly
high-risk young men with special needs, such as shelters for runaway and
homeless youth, the foster care system, or the juvenile justice system, is yet
another promising way to broaden the base of populations served. Beyond the
young men themselves, agencies may want to reach the broader environments
that shape these youth their families; schools; communities; health, welfare,
and social service agencies; government; and the business sector.
VALUE
OF
S TARTING S MALL
Where existing resources are scarce, small-scale efforts (such as educational initiatives or pilot programs) may be the only realistic starting place. These efforts
are worthwhile if they are planned thoughtfully and conducted well. However,
making a commitment to address the reproductive health needs of young
Recommended Actions
33
m e n e ven if the effort is quite focused, like a health fair or a media spot
almost inevitably leads to additional opportunities to do more. For example, a
The working
simple media spot encouraging young men to be screened for STDs requires
capacity in the community to conduct the tests, provide treatment, convey
group s overarching
information, teach partner communication skills, follow up with partners, and
recommendation is
provide other services that might keep young men from needing the screening
that the U.S.
and treatment again. Once young men are engaged and motivated to improve
their reproductive health, organizations need to be able to either provide the
Surgeon General
needed services or create partnerships with the clinical and other resources that
spearhead a broad
meet young men s reproductive and other health needs. Many communities do
Young Men s Health
not currently have anything approaching a full range of clinical and sexual
reproductive health services for young men.
Initiative to address
these problems.
F EDERAL C HALLENGES
AND
O PPORTUNITIES
Promoting the sexual and reproductive health of young men is an extremely
important and neglected policy concern one of many aspects of young men s
health that needs more attention and resources from the federal agency with
the key responsibility for meeting these health needs, the U.S. Department of
Health and Human Services (DHHS). The health of many young men in the
country is compromised by participation in health-risk behaviors and lack of
access to adequate health care and support services that affect their ability to
make successful transitions into adulthood and lead to unacceptably high
rates of mortality and morbidity. Consequently, the working group s overarching recommendation is that the U.S. Surgeon General spearhead a broad
Young Men s Health Initiative to address these problems.
34 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Young Men s Health Initiative
KEY ACTIONS NEEDED BY SURGEON GENERAL
To implement a broad Young Mens Health Initiative, the working group
recommends that the Surgeon General immediately take the following actions
and rigorously evaluate these efforts three years after implementation:
Determine Extent of Existing Federal Efforts. Solicit statements from the
relevant operating agencies within DHHS Centers for Disease Control and
Prevention, Substance Abuse and Mental Health Services Administration, Office
of Population Affairs, National Institutes of Health, Health Resources and
Services Administration, Bureau of Primary Care, Bureau of HIV/AIDS
Prevention, Administration for Children and Families, and others to describe
their goals, plans, and financial resources they have that will address the pressing health needs of young men in the United States.
Assess Adequacy of Insurance Coverage. Review Medicaid and the State
Childrens Health Insurance Program (SCHIP) for the extent to which they provide coverage for the male health clinical package of services including sexual
and reproductive health services, as well as for their outreach and enrollment
strategies targeting young men. Particular attention should be paid to issues of
confidentiality.
Expand Current Federal Efforts. Request additional funding from the
Secretary of DHHS to support new program initiatives and to conduct research
and evaluation to identify best practices.
Document Gaps between Needs and Federal Services. Develop a report on
young mens health in the United States, to document the health condition of
young men and to examine the evidence about DHHS s ability to address their
health needs.
Recommended Actions
35
Toward a National Strategy
Integrate Young Men s Health Needs across Federal Efforts and Agencies.
Actions here would include integrating young mens health into the U.S.
Department of Health and Human Services Interagency Fatherhood Initiative;
including a broader array of young mens health objectives and indicators
among the Healthy People 2010 priorities; and reaching out to other federal
agencies such as the Departments of Education, Justice, Labor, and Defense to
develop coordinated efforts addressing young mens health needs.
The working
group also urges
the Surgeon
General to make
sexual and
reproductive health
concerns a major
priority within
this effort.
Expand Training of Health Professionals. Provide leadership in the expansion of training for health professionals and others regarding young mens health.
Reorient Focus of Managed Care Providers. Spur medical directors of
major managed health care programs to address young men s health.
Collaborate with Media to Convey Positive Images. Partner with the media
to highlight how current images of men may convey messages that are harmful
to their health and to spotlight the health needs of young men.
The working group also urges the Surgeon General to make sexual and
reproductive health concerns a major priority within this effort. To this end, the
group offers more specific recommendations about how to improve the capacity of the communities and federal agencies to address these concerns.
Monitor the Five Goals. First, the overall goals set by the working group are
consistent with the Healthy People 2010 goals for the nation, such as the prevention of STDs and unintended pregnancy. However, a system for monitoring
and measuring the receipt of services by men and the outcomes is still underdeveloped for the Healthy People Campaign. The group recommends explicitly monitoring the attainment of its goals for young men s sexual and reproductive health.
36 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Young Men s Health Initiative
The goals are repeated here for emphasis:
➤
Promote young mens sexual health and development.
➤
Promote healthy intimate relationships.
➤
Prevent and control STDs, including HIV.
➤
Prevent unintended pregnancy.
➤
Promote responsible fatherhood.
Target Most Vulnerable Groups. Second, while all men face a current
health care system that is mostly unresponsive to their sexual and
reproductive health, the working group identified seven high-priority target
populations because of their higher levels of participation in risky sexual
behaviors, their greater levels of negative reproductive heath outcomes, and
their greater barriers to service. These populations are (1) young men of color,
(2) men living in poverty or impoverished neighborhoods, (3) out-of-school
men, (4) men involved in the criminal justice system, (5) men in foster care,
(6) gay/bisexual men, and (7) men in their early 20s. Substantial numbers of
young men fall into at least one of these at-risk groups. Many belong to more
than one of these groups and face multiple and related sources of
disadvantage.
Emphasize Collaboration across Agencies and Organizations. Third, any
action to promote sexual and reproductive health is encouraged. But the
working group particularly recommends that community agencies and
organizations collaborate to leverage existing resources and to develop new
resources that will provide accessible and effective educational, counseling,
clinical, and other supportive services for young men.
Recommended Actions
37
Toward a National Strategy
These collaborative efforts should:
➤ Promote a comprehensive, client-centered approach to sexual and reproductive health.
➤ Provide a minimum standard of clinical sexual and reproductive health
services for young men.
➤ Ensure meaningful community involvement through the participation of
organizations that are rooted in the community, that hold community trust, and
that have a longstanding relationship with young men in the community. These
types of organizations can be lead agencies or partners.
Building partnerships across agencies and organizations is challenging but
can be highly rewarding when the result is a comprehensive range of services
that meets young mens sexual and reproductive health care needs.
Strengthen Federal Facilitator Role. DHHS should take steps to facilitate the
development of collaborative partnerships. One obstacle to establishing and
maintaining sexual and reproductive health programs for men is the scarcity
of designated sources of funding for such programs. No federal program has a
mandate or mission to serve the sexual and reproductive health needs of men.
At the same time, several relevant federal programs that do exist are underutilized for delivery of these services to male populations.
Federal health insurance programs such as Medicaid and the State Childrens
Health Insurance Program (SCHIP) could be more important in reimbursing the
clinical component of mens reproductive health services. It must be noted,
though, that reproductive health services represent a minuscule fraction of these
programs multibillion-dollar budgets. And mens health projects will need to
maneuver within the rules, requirements, and managed care aspects of these vast
insurance programs if they are to be successful in tapping their funds. In
particular, DHHS should examine whether certain dimensions of Medicaid and
38 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Young Men s Health Initiative
SCHIP implementation, including the issue of confidentiality, unintentionally act
as barriers to reimbursing reproductive health services delivered to young men.
Existing federal grant programs also can be tapped to broaden access to sexual
and reproductive health care for young men. The relevant programs are the Title X
Family Planning Program, the Title XX Adolescent Family Life Program, the Centers
for Disease Control Reproductive Health and HIV and STD Prevention Programs,
the Title V Maternal and Child Health Block Grant Program, the Community Health
Center Program, the Ryan White Care Act, the Title XX/Social Services Block Grant
DHHS should
Program, and Temporary Assistance for Needy Families. In addition to these are
take steps to ease
other categorical grant progra m s f rom agencies such as the Substance Abuse and
access to funds and
Mental Health Services Administration and the Health Resources and Services
Administration that could support some of the services recommended.
build the capacity
of community
Ease Access to Federal Funding. To deliver the full range of services, community agencies will almost certainly need multiple sources of funding. While
agencies to use
doing this is cumbersome for program administrators because of the need for
them for sexual
multiple grant applications and the fragility of some sources of funding such as
and reproductive
demonstration programs, it does reflect the current fiscal reality faced by health
and human service agencies throughout the country, including family planning
agencies. DHHS should take the following steps to ease access to funds and
health services for
young men.
build the capacity of agencies to use them for sexual and reproductive health
services for young men:
➤Request additional funding from the Secretary for a program that supports community agencies in gaining access to existing resources to deliver
sexual and reproductive health services to men. Without some programmatic
funds devoted to building infrastructure and supporting key administrative
functions, the working group strongly believes that community agencies will be
unable to access existing resources and maintain continuity of services.
Recommended Actions
39
Toward a National Strategy
➤Solicit plans from the relevant operating agencies within DHHS that show
how those agencies will contribute resources to meet the sexual and reproductive health needs of men.
➤ Support technical assistance and training for agencies to build their
capacity to access existing sources of financial support, including nonfederal
funding sources.
Enhance Information and Technical Assistance. DHHS can encourage
community agencies to develop services for young men in addition to providing
program financing. A key function is supporting activities that will promote the
dissemination of knowledge about effective service approaches, community
mobilization strategies, innovative ideas, and administrative practices. DHHS
should also encourage and fund communication among programs, so that existing knowledge and experience can be readily shared and integrated quickly into
practice. Making this knowledge and experience accessible to planners of new
programs is essential to the effective mobilization and use of people resources
in communities. The working group recommends that DHHS provide support
for the following:
➤ A clearinghouse to inventory and collate information about existing program approaches and to make them readily accessible to programs and program planners.
➤ Training and technical assistance to community agencies and program
planners.
➤ Forums in which innovative ideas and practices can be shared.
➤Dissemination of information and program promotion.
40 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Young Men s Health Initiative
Build a Stronger Research and Evaluation Base. DHHS should support
basic and program evaluation research to build an information base capable of
monitoring shifts in the sexual and reproductive health of young men in the
United States, gaining an understanding of the factors contributing to outcomes
for various population groups, and identifying effective program practices. A
continual investment in research and development will build the base of knowledge and contribute to innovation. Strategies include the following:
➤Supporting and encouraging routine national surveys that include
A continual
measures of men s sexual and reproductive health. For example, the National
investment in
Survey of Family Growth in 2002 is planning to include men in the sample for
research and
the first time.
➤Supporting analysis of data from surveys and other sources to build an
understanding of the factors contributing to better sexual and reproductive
health outcomes.
➤Supporting innovative demonstration programs in which new programmatic approaches can be tested and studied.
➤Supporting rigorous outcome evaluation of programs to identify pro-
development will
build the base of
knowledge and
contribute to
innovation.
grams that are very promising models of service delivery.
Support More Effective Professional Training. DHHS should support the
development of training curricula for health professionals and other community agency personnel to provide them with the information and skills needed to
deliver sexual and reproductive health services to young men. In addition, curricula are needed for medical schools and other institutions providing training
to health professionals and for continuing education for personnel in the field.
The development of such curricula will also build consensus about the core
content and practice of promoting young mens sexual and reproductive health.
Recommended Actions
41
Benefits of a National Effort
Y OUNG M EN T HEMSELVES
E
xpanding efforts to promote the sexual and reproductive health of
young men in the United States will improve health outcomes among
the young men themselves, their partners, their children, and society
as a whole. A broad strategy to facilitate the development of young men into
physically and emotionally healthy adults must focus on the whole array of
their health needs, with sexual and reproductive health an important part.
Meeting the sexual and reproductive health needs of young men, as the working group has stated, will increase men s knowledge and understanding of
their own health including their sexual health and give them better skills to
reduce disease and to adopt healthy lifetime practices. Men will also benefit
from increased understanding and better skills to negotiate and sustain successful relationships with partners. And they may avoid premature fatherhood
and unintended pregnancies and births. Offering both men and women the
means and opportunity to plan their families may lead to greater nurturing
and parental support for the children they have.
F EMALE PARTNERS
Providing men with the knowledge and skills that many of them lack will complement and leverage existing investments in womens reproductive health services. These mens sexual partners will reap similar benefits in the form of reductions in disease and unintended pregnancies and births. Partners will also
experience more support from these men for their own preventive health
efforts. And improved communication and negotiation between partners will
improve the chances of healthy relationships that sustain themselves over time,
to the benefit of both partners and their children.51
42 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
S OCIETY
Society as a whole also will benefit from investing in promoting sexual and reproductive health for men. The public sector now pays a substantial amount to cover
health costs associated with STDs. It also covers the birth and delivery costs of
people not covered by private health insurance. Additional public funds are
expended to establish paternity for nonmarital children and to collect child support for children who do not live with their biological fathers. To the extent that
efforts to promote male sexual and reproductive health lead to reductions in STDs
or unintended pregnancies and births, these investments will pay for themselves.
Promoting the sexual and reproductive health of young men in the United
States could produce direct health benefits for the men themselves and additional benefits for their partners, their children, taxpayers, and the social fabric
of our society. As this report shows, developing strategies to deliver the array of
services needed to accomplish this objective will require commitment, ingenuity, a break with tradition, and collaboration across diverse community agencies. Each of these requirements will create both psychic and financial demands
beyond the actual dollars that are required for programs and services. While the
working group acknowledges the scope and difficulty of the task, it believes that
the benefits resulting from integrating mens sexual and reproductive health
needs into public health promotion efforts will be well worth the investment.
The group urges the U.S. Surgeon General and DHHS to provide leadership in
promoting the dialogue and program experimentation now required to ensure
that the sexual and reproductive health needs of both young men and young
women in the United States are addressed.
Benefits
43
E N D N O T E S
1. Ndong, I., R. M. Becker, J. M. Haws, and M. N. Wagner. 1999. Mens Reproductive Health:
Defining, Designing, and Delivering Services. International Family Planning Perspectives 25 (supplement): S53 S55.
2. Satcher, D. 1999. Evolving Health Priorities. Washington, D.C.: Office of Public Health and
Science.
3. U.S. Department of Health and Human Services. 2000b. Healthy People 2010: Understanding and
Improving Health, conference edition. Washington, D.C.: author.
4. A monograph containing the revised working papers is also available.
5. Bachrach, C., and F. Sonenstein. 1998. Report of the Working Group on Male Fertility and
Family Formation. In Nurturing Fatherhood: Improving Data and Research on Male Fertility, Family
Formation, and Fatherhood (45 98). Washington, D.C.: Federal Interagency Forum on Child and Family
Statistics.
6. Mincy, R. 1995. Reforming Income Maintenance and Family Support Systems to Strengthen
Fragile Families. Statement presented before the U.S. Commission on Child and Family Welfare.
7. Bachrach, C., and F. Sonenstein. 1998. Report of the Working Group on Male Fertility and
Family Formation. In Nurturing Fatherhood: Improving Data and Research on Male Fertility, Family
Formation, and Fatherhood (45 98). Washington, D.C.: Federal Interagency Forum on Child and Family
Statistics.
8. Bernard, S. N., and J. K. Knitzer. 1999. Map and Track State Initiatives to Encourage Responsible
Fatherhood. New York: National Center for Children in Poverty.
9. Federal Interagency Forum on Child and Family Statistics. 1998. Nurturing Fatherhood:
Improving Data and Research on Male Fertility, Family Formation, and Fatherhood. Washington, D.C.:
Federal Interagency Forum on Child and Family Statistics.
10. Bachrach, C., and F. Sonenstein. 1998. Report of the Working Group on Male Fertility and
Family Formation. In Nurturing Fatherhood: Improving Data and Research on Male Fertility, Family
Formation, and Fatherhood (45 98). Washington, D.C.: Federal Interagency Forum on Child and Family
Statistics.
11. Levine, J. A., and E. W. Pitt. 1995. New Expectations: Community Strategies for Responsible
Fatherhood. New York: Families and Work Institute.
12. Brown, S. S., and L. E. Eisenberg. 1995. The Best Intentions: Unintended Pregnancy and the WellBeing of Children and Families. Washington, D.C.: National Academy Press.
13. U.S. Department of Health and Human Services. 1997. A National Strategy to Prevent Teen
Pregnancy. Washington, D.C.: author.
14. Kirby, D. 1997. No Easy Answers: Research Findings on Programs to Reduce Teen Pregnancy.
Washington, D.C.: The National Campaign to Prevent Teen Pregnancy.
15. Centers for Disease Control and Prevention. 2000. http://www.cdc.gov/hiv/prevresearch.htm.
16. Schulte, M., and F. Sonenstein. 1995. Men at Family Planning Clinics: The New Patients?
Family Planning Perspectives 27 (5): 212 216, 225.
17. Sonenstein, F., L. Ku, L. Lindberg, C. Turner, and J. Pleck. 1998. Changes in Sexual Behavior
and Condom Use among Teenaged Males: 1988 to 1995. American Journal of Public Health 88 (2):
956 959.
18. Frost, J. J., and M. Bolzan. 1997. The Provision of Public Sector Services by Family Planning
Agencies in 1995. Family Planning Perspectives 29 (1): 6 14.
19. Arizona, California, Iowa, Massachusetts, Missouri, New Jersey, New York, Pennsylvania, Texas,
and Wyoming.
20. Family Planning Councils of America. 1999. The Best Kept Secret of Title X: Meeting the
44 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
Reproductive Health Needs of Men in Our Communities. Pittsburgh: Family Planning Councils of
America.
21. Sonenstein, F. L., K. Stewart, L. D. Lindberg, M. Pernas, and S. Williams. 1997. Involving Males in
Preventing Teen Pregnancy: A Guide for Program Planners. Washington, D.C.: The Urban Institute.
22. Bearman, P. S., J. Jones, and J. R. Udry. 1997. The National Longitudinal Study of Adolescent
Health. In The National Longitudinal Study of Adolescent Health: Research Design.
http://www.cpc.unc.edu/projects/addhealth/design.html; Centers for Disease Control. 1998b. The
Youth Risk Behavior Survey: Trends in Sexual Risk Behaviors among High School Students United
States, 1991 1997. Morbidity and Mortality Weekly Report 47 (36): 749 752; Laumann, E. O., J. H.
Gagnon, R. T. Michael, and S. Michaels. 1994. The National Health and Social Life Survey. In The
Social Organization of Sexuality: Sexual Practices in the United States. Chicago: The University of
Chicago Press; Sonenstein, F. L., J. H. Pleck, and L. Ku. 1989. The National Survey of Adolescent Males
(Sexual Activity, Condom Use, and AIDS Awareness among Adolescent Males). Family Planning
Perspectives 21: 152 158; and Tanfer, K., W. R. Grady, D. H. Klepinger, and J. O. G. Billy. 1991. The
National Survey of Men: Condom Use among U.S. Men. Family Planning Perspectives 25: 61 66.
23. Sonenstein, F., L. Ku, L. Lindberg, C. Turner, and J. Pleck. 1998. Changes in Sexual Behavior and
Condom Use among Teenaged Males: 1988 to 1995. American Journal of Public Health 88 (2): 956 959.
24. Henshaw, S. 1999. Teenage Pregnancy: Overall Trends and State-by-State Information. New York:
The Alan Guttmacher Institute; and Ventura, S. J., T. J. Mathews, and S. C. Curtin. 1999. Declines in
Teenage Birth Rates, 1991 1998: Update of National and State Trends. National Vital Statistics Reports
47 (26).
25. Centers for Disease Control and Prevention. 1998a. Sexually Transmitted Disease Surveillance
1997. Atlanta: Centers for Disease Control and Prevention.
26. Hoyert, D. C., K. D. Kochanek, and S. L. Murphy. 1999. Deaths: Final Data for 1997. National
Vital Statistics Reports 47 (19).
27. Ku, L., L. St. Louis, C. Farshy, S. Aral, C. F. Turner, L. D. Lindberg, and F. Sonenstein. 2000. Risk
Behaviors, Medical Care, and Chlamydial Infection among Young Men in the United States. Under review.
28. Centers for Disease Control. 1999. Sexually Transmitted Disease Surveillance 1998. Atlanta:
Centers for Disease Control and Prevention.
29. Landry, D. J., and Forrest, J. D. 1995. How Old Are U.S. Fathers? Family Planning Perspectives
27 (4): 159 161, 165.
30. Miller, K. S., L. F. Clark, and J. S. Moore. 1997. Sexual Initiation with Older Male Partners and
Subsequent HIV Risk Behavior among Female Adolescents. Family Planning Perspectives 29 (5): 212 214.
31. Lindberg, L. D., L. Ku, and F. Sonenstein. 2000b. Adolescents Reports of Receipt of
Reproductive Health Education, 1988 1995. Family Planning Perspectives 32 (5): 220 226.
32. Bradner C., L. Ku, and L. D. Lindberg. 2000. Older, but Not Wiser: How Do Men Get AIDS/STD
Information after High School? Family Planning Perspectives 32 (1): 33 38.
33. Porter, L. E., and L. Ku. 2000. Use of Reproductive Health Services among Young Men, 1995.
Journal of Adolescent Health 27 (3): 186 194.
34. Bradner C., L. Ku, and L. D. Lindberg. 2000. Older, but Not Wiser: How Do Men Get AIDS/STD
Information after High School? Family Planning Perspectives 32 (1): 33 38.
35. Forrest, K. A., J. M. Swanson, and D. E. Beckstein. 1989. The Availability of Educational and
Training Materials on Mens Reproductive Health. Family Planning Perspectives 21 (3): 120 122.
36. Frost, J. J., and M. Bolzan. 1997. The Provision of Public Sector Services by Family Planning
Agencies in 1995. Family Planning Perspectives 29 (1): 6 14; unpublished data from the Alan
Guttmacher Institute.
45
37. Elster, A. B., and N. J. Kuznets. 1994. AMA Guidelines for Adolescent Preventive Services (GAPS).
Baltimore: Williams and Wilkins.
38. Society for Adolescent Medicine. 1991. Position Paper on Reproductive Health Care for
Adolescents. Journal of Adolescent Health 12: 649 661.
39. U.S. Department of Health and Human Services. 2000a. Bright Futures: Guidelines for Health
Supervision of Infants, Children, and Adolescents. Washington, D.C.: author.
40. Sandman, D., E. Simantov, and C. An. 2000. Out of Touch: American Men and the Health Care
System. New York: The Commonwealth Fund.
41. Millstein, S. G., A. C. Petersen, and E. O. Nightingale, eds. 1993. Promoting the Health of
Adolescents: New Directions for the Twenty-First Century. New York: Oxford University Press.
42. Donovan, J. E., and R. Jessor. 1985. Structure of Problem Behavior in Adolescence and Young
Adulthood. Journal of Counseling and Clinical Psychology 53: 890 904; Elliott, D. S., and B. J. Morse.
1989. Delinquency and Drug Use as Risk Factors in Teenage Sexual Activity. Youth and Society 21:
21 60; Lindberg, L. D., S. Boggess, L. Porter, and S. Williams. 2000. Teen Risk-Taking: A Statistical
Portrait. Washington, D.C.: The Urban Institute; and Osgood, D. W., P. M. O Malley, J. G. Bachman, and
L. D. Johnston. 1988. The Generality of Deviance in Late Adolescence and Early Adulthood. American
Sociological Review 53: 81 93.
43. Lindberg, L. D., S. Boggess, L. Porter, and S. Williams. 1999. Co-Occurrence/Clustering of Youth
Risky Behavior. Unpublished table in a report to the DHHS Office of the Assistant Secretary for
Planning and Evaluation.
44. Lindberg, L. D., L. Ku, and F. Sonenstein. 2000a. Adolescent Sexual Behavior within the Context
of Drugs and Alcohol. Journal of Sex Research (forthcoming).
45. Ford, K., and A. E. Norris. 1998. Alcohol Use, Perceptions of the Effects of Alcohol Use, and
Condom Use in Urban Minority Youth. Journal of Acquired Immune Deficiency Syndrome Human
Retrovirology 17 (3): 269 274; and Weinstock, H. S., C. Lindan, G. Bolan, S. M. Kegeles, and N. Hearst.
1993. Factors Associated with Condom Use in a High-Risk Heterosexual Population. Sexually
Transmitted Diseases 20: 14 20.
46. Graves, K. L., and B. C. Leigh. 1995. The Relationship of Substance Use to Sexual Activity among
Young Adults in the United States. Family Planning Perspectives 27; and Latkin, C., W. Mandell, M.
Oziemkowska, M. Vlahov, and D. Celentano. 1994. The Relationships between Sexual Behavior, Alcohol
Use, and Personal Network Characteristics among Injecting Drug Users in Baltimore, MD. Sexually
Transmitted Diseases 21: 161 167; and Leigh, B. C., M. T. Temple, and K. F. Trocki. 1994. The Relationship
of Alcohol Use to Sexual Activity in a U.S. National Sample. Social Science Medicine 39: 1527 1535.
47. Mott, F. L., and R. J. Haurin. 1988. Linkages between Sexual Activity and Alcohol and Drug Use
among American Adolescents. Family Planning Perspectives 20: 128 136; and Rosenbaum, E., and D.
B. Kandel. 1990. Early Onset of Adolescent Sexual Behavior and Drug Involvement. Journal of
Marriage and the Family 52: 783 798.
48. Baker, S. A., D. M. Morrison, M. R. Gillmore, and M. D. Schock. 1995. Sexual Behaviors,
Substance Use, and Condom Use in a Sexually Transmitted Disease Clinic Sample. Journal of Sex
Research 32: 37 44; and Latkin, C., W. Mandell, M. Oziemkowska, M. Vlahov, and D. Celentano. 1994.
The Relationships between Sexual Behavior, Alcohol Use, and Personal Network Characteristics
among Injecting Drug Users in Baltimore, MD. Sexually Transmitted Diseases 21: 161 167.
49. Sly, D. F., D. Quadagno, D. F. Harrison, I. Eberstein, and K. Riehman. 1997. The Association
between Substance Use, Condom Use, and Sexual Risk among Low-Income Women. Family Planning
Perspectives 29: 132 136.
50. Marx, R., S. O. Aral, R. T. Rolfe, C. E. Sterk, and J. G. Kahn. 1991. Crack, Sex, and STD. Sexually
Transmitted Diseases 18: 92 101.
51. Becker, S. 1996. Couples and Reproductive Health: A Review of Couple Studies. Studies in
Family Planning 27 (6): 291 306.
46 Young Men’s Sexual and Reproductive Health: Toward a National Strategy
For Further Information
The recommendations set forth here are based in part on papers prepared by members of the working
group for the 1999 Airlie House Conference (see pages 6 7). The edited papers are chapters of a companion publication, Young Mens Sexual and Reproductive He a l t h Toward a National Strategy: Getting Started,
November 2000, Urban Institute Press. Below is the table of contents for this companion volume:
Young Mens Sexual and Reproductive Health
Toward a National Strategy:
Getting Started
Freya L. Sonenstein, editor
TABLE OF CONTENTS:
To order either this
publication or the
companion volume,
please call the
Public Affairs office at
(202) 261-5709
Framework and Recommendations for a Young Mens Sexual and
Reproductive Health Initiative
Freya L. Sonenstein
Why Males, Why Now: The Rationale for Addressing the
Reproductive Health of Young Men
Laura Duberstein Lindberg and Freya L. Sonenstein
Young Mens Sexual and Reproductive Health: A Framework
or e-mail
Laura Porter, Freya L. Sonenstein, and Laura Duberstein Lindberg
paffairs@ui.urban.org;
Clinical Care for the Sexual and Reproductive Health of Adolescent
or call 1-888-UIPRESS
and Young Adult Men
or e-mail
pubs@ui.urban.org.
Jonathan M. Ellen
Getting Started: Practical Advice
·
·
Claire Brindis, Laura Porter, Hector
Sanchez,
and Freya L. Sonenstein
The Keys to Enhancing Young Mens Reproductive Health:
Collaborative Partnerships
Kay A. Armstrong, Shawn E. Gibson, Roberta Herceg-Baron, and Dorothy Mann
Financing Young Mens Reproductive Health Projects
Leighton Ku, Christina Pallitto and Laura Porter
Appendix: Useful Web Sites
48 Young Men’s Sexual and Reproductive Health: Toward a National Strategy