Expert Article
Review Articles
Healthcare Perspectives
Feature Articles
WWW.UCDSMJ.COM
su pp or te d by Bank of Ireland, Montrose
Original Research
2015
EDITION 02
Table of Contents
Editorial Team
Acknowledgements
Foreword
Original Research
All published articles are decided by a panel of editors drawn from the
of the UCDsmj or of the UCD School of Medicine and Medical Science.
Expert Article
The authors, editors and publishers do not accept any responsibility for
patients and the interpretation of published material lies with the medical
practitioner. The statements and opinions expressed are those of the au-
06
Emergency Medical Services and Emergency
Medical Science - Where Now?
18
Gestational Weight Gain and Gestational Diabetes
Mellitus: Popular Beliefs and Emerging Evidence
26
Prof. Gerard Bury
any loss or damage arising from actions or decisions based on information
contained in this publication; ultimate responsibility for the treatment of
Attitudes to Clinical Research within the
Epidermolysis Bullosa (EB) Community Maeve Jones-O’Connor, Dr. Amanda McCann, Avril Kennan
student body of University College Dublin. The opinions expressed within
the journal are the authors’ own and do not necessarily reflect the opinions
02
03
04
Review Articles
thors and the inclusion in this publication of material relating to a particular
Lisa A O'Higgins, Dr. Amy C O'Higgins, Sophie Gray,
product, method or technique does not amount to an endorsement of its
Thomas McCartan, Dr. Ann Rowan, Dr. Anne Fennessey,
value or quality, or of the claims made by its manufacturer.
Prof. Michael J Turner
All permissions were obtained.
Copyright © 2015 UCD Student Medical Journal
Considering the Policy of Indefinite Deferral
Imposed on MSM Blood Donors in Ireland
All Rights Reserved. No part of this publication may be reproduced, stored
Dr. John Lambert
Kevin O’Malley, Reviewed by Dr. Sinead McDermott,
in a retrieval system or transmitted in any form or by any means electronic,
mechanical, photocopying, recording, scanning or otherwise except as
described below, without the permission in writing of the publisher.
to the extent permitted by national copyright law. All correspondence
including orders for advertising space should be addressed to:
Marketing Manager,
UCD Student Medical Journal,
Healthcare
Perspectives
Alternatively, an email can be sent to ucdsmj@gmail.com
This current volume can be accessed at http://ucdsmj.com
HR Holfeld,
Merville Road,
Stillorgan,
Co Dublin
ISSN (Print): 2009-4795
ISSN (Online): 2009-4809
The Use of Aspirin for Primary Prevention
of Cardiovascular Disease:
Review of Literature and Sample Evidence
of Common Practice in Ireland 52
A Day in the Life of an Intern in Ireland
62
Interview with Dr. Rhona Mahony
66
Top 10 Apps for Health Care Students
72
Maeve Montague ft. Dr. Ken Fitzpatrick
Neasa Conneally, Sarah Murphy
Published by Night Printers,
Unit 6,
42
John Travers, Edited by Dr. Helen Gallagher
School of Medicine and Medical Science,
Dublin 4
Food Poverty and Policy in Ireland:
A Review of the Literature Diarmuid D Sugrue, Edited by Prof. Ivan Perry Copying of articles is not permitted except for personal and internal use,
UCD Belfield,
34
Feature Articles
Sarah Murphy, Nora Tadros
Student Summer Research - Experience
76
Bewilderment: A Symptom of,
& Solution for Empathotoxicity
82
Cathal Ahern, Peter Fryc, Caroline Moran
Matthew Shipsey
UCD Student Medical Journal
03
Edition 2
Committee 2014/15
Neasa
Conneally
Secretary
Róisín K
O'Sullivan
Editor
Maeve
Jones-O'Connor
Finance & Marketing Manager
Bebhinn
Shine
Editor
Deirdre
Ryan
Kordan
Harvey
Maeve
Healy
Ciara
Kehoe
UCD Medical Society
Liaison
Editorial Team
Editorial Team
Editorial Team
Amin
Manssouri
Roisin
McGinley
Maeve
Montague
Sarah
Murphy
Editorial Team
Editorial Team
Editorial Team
Editorial Team
Emily
Pender
Ben
Shanahan
Nora
Tadros
Cathal
Ahern
Editorial Team
Editorial Team
Editorial Team
Design Team
Matthew
Bechbache
Nina
Esfa
Jack
Evans
Rajiv
Lakhani
Design Team
Design Team
Design Team
Eleanor
O'Neill
Krishna
Vinnakota
Darren
O'Gorman
Design Team
Design Team
Marketing Team
Design Team
← Committee 2014/15
→ Acknowledgement
Acknowledgements
To all those who made this edition of the UCDsmj possible, thank-you. We particularly want to extend
our gratitude to the members of the UCD staff who guided and supported us throughout this journey.
02
Co-Founders of the UCDsmj and
Co-Editors of the First Edition
Aileen Conway
Denise Connolly
Founding Team
Norella Broderick
Kyle Halligan
Siobhán McKeown
Adrian Rutledge
Keith Siew
Website Design & Maintenance
Cathal Ahern
based on a previous website by
Caroline Fenlon
Sam Kehoe
Poster Design by
Matthew Bechbache
School of Medicine and
Medical Science Reviewers
Dr. Helen Gallagher
Dr. Amanda McCann
Dr. Jennifer Thompson
School of Medicine and
Medical Science Advisors
Dr. Suzanne Donnelly
Paul Harkin
Dr. Peter Holloway
Prof. Jason Last
The following UCD staff held writing
and research workshops on behalf
of the UCDsmj
Dr. Peter Holloway
Dr. Amanda McCann
Dr. Cliona McGovern
UCD Medical Society
Aoife McEvoy, Auditor
Alex Owens, Treasurer
UCD Medical Society Liaisons
Alex Owens
Deirdre Ryan
Journal Design and Photography
Fay Teo
cargocollective.com/sufuiteo
Printer
Night Printers
www.nightprinters.com
The committee would like to thank
the following individuals for their
contributions to the UCDsmj
Dr. Mary Codd
Jamie Condren
Aoife Cox
Rory Crean
Mairead Egan
Hannah Featherstone
Dr. Susan Fitzgerald
Dr. Ken Fitzpatrick
Mary Headon
Suzanne Hayden
Prof. Carel le Roux
Dr. Rhona Mahony
Dr. Paddy Mallon
Dr. Ambrose McLoughlin
Eibhlin Mulroe
Sean O'Rourke
Prof. Donal O'Shea
Cian O'Sheehan
Adam Tattersall
Zoe Thompson
Helen Tobin
04
UCD Student Medical Journal
Edition 2
05
Foreword
Foreword
Associate Dean for Programmes &
Educational Innovation
UCD School of Medicine & Medical Science
There is a theme that permeates this edition of the SMJ that I would
like to highlight. Since 2008, the School has partnered with patients
through our PACE programme (Patient and Advocate Centred
Education and Research). This programme invites patients and patient
advocacy organisations to become involved in teaching our students
within medical, biomedical and diagnostic imaging programmes.
Sometimes, this involves a patient giving a lecture or a seminar. It
can also involve groups of patients entering our patient educator
programme which ultimately leads to their participation as educators
in many of our clinical skills and professionalism learning initiatives.
More recently, students have partnered with voluntary organisations
in conducting research in domains associated with their cause. I am
delighted therefore to note that patients and society feature strongly
Prof. Jason Last
within this edition, with the role of students and faculty as patient
advocates core to many of the articles. The first article highlights the
importance of the patient voice in epidermolysis bullosa research.
We then meet evidence-based opinion highlighting the need for
measures of quality to include patient outcomes in emergency care
provision and then articles debating the impact of blood donation
policy on society and the continuing food poverty struggle in Ireland.
I can’t help thinking that this theme has arisen, in part, because of
the School’s unique approach to patient partnership which aims to
propogate and harness the innate patient and society centricity of
our all our students and staff.
Prof. Jason Last
This is a fascinating edition of the UCD Student
Medical Journal (UCDsmj) and should be read from cover to
cover. It is the product of several years of effort which started
with the production of the first edition of the UCDsmj and might
have finished there only for the determination of the Journal’s
leadership and their supporters. As Director of Educational
Development in the School, one of the five goals that I have laid
out to be achieved over the next five years is that each student
in each programme will have been supported in reaching their
individual potential. This edition of the UCDsmj demonstrates
the importance of student-led initiatives in achieving that goal.
The student contributors have demonstrated that, given the
opportunity, they are more than capable of writing articles of
great interest to a wide audience and that frequently challenge
our knowledge, traditions and values. This form of personal
endeavour is of enormous merit and should be multiplied and
more systematically incorporated into the student experience at
UCD.
Foreword by
The professional approach of the UCDsmj committee, and their
desire to make this Journal sustainable gives great confidence that
this is the second of many editions. I note in particular the stellar
efforts of Neasa Conneally, Roisin O’Sullivan, Maeve Jones-O’Connor
and Bebhinn Shine and their editorial, design and marketing team
members. Equally, staff associated with the School have assisted,
collaborated, supervised projects and submitted to interviews making
this student-led initiative a shining example of what can be achieved
through staff-student collaboration. Given the admixture of science,
the patient’s voice and the humanities distributed through the edition,
it seems fitting to segue to the words of Dr. Anne Merriman.
Dr. Merriman, MBE, is a distinguished alumnus of UCD School
of Medicine who pionneered the hospice movement in Africa, a
continent to which she has devoted the majority of her working life.
In an inspiring address to the 2014 Medical Gala Dinner, Dr. Merriman
explained to the gathered graduands, that
“patients want to know what’s in your mind
and what’s in your heart.”
It appears that we are enabling a generation of medical students who
have the capability of rising to Dr. Merriman’s humbling challenge.
Attitudes to
Clinical
Research
within the
Epidermolysis
Bullosa (EB)
Community
Written by
Maeve Jones-O'Connor1,
Dr. Amanda McCann1,
Avril Kennan2
UCD School of Medicine and Medical Science,
University College Dublin, Belfield, Dublin 4, Ireland
1
DEBRA Ireland, Clanwilliam Terrace, Grand Canal Quay,
Dublin 2, Ireland
2
Clinical research; Clinical Trials; Epidermolysis Bullosa; Patient
Advocacy; Patient Engagement
07
UCD Student Medical Journal
Keywords
06
Original Research
Attitudes to Clinical Research within the Epidermolysis Bullosa
(EB) Community
08
UCD Student Medical Journal
Written by
Maeve Jones-O'Connor
Dr. Amanda McCann
Avril Kennan
A BSTRACT
BACKG RO U ND
There has been much investigation of attitudes towards clinical
research (CR) in the general population.1-11 This research mainly concerns
attitudes towards clinical trials in a general sense, i.e. in a non-disease specific
way. In the context of rare diseases, the general research is of limited relevance.
O B J E CT I V E
The aim of this study was to examine attitudes towards CR and
factors involved in clinical trial (CT) participation in epidermolysis bullosa (EB)
researchers and patients.
M E T H O DS
This was a two phase, mixed methods study. Semi-structured
interviews were used to gather the views of EB clinical researchers (n=11). The
results were thematically analysed and inductive analysis was performed. An
online survey of patients and carers (n=43) gathered the patient perspective,
in relation to factors influencing the decision on whether to partipate in clinical
trials and perceptions of clinical research.
RE S U LT S
The main themes that emerged from the interviews with
researchers were: 1) many and varied challenges face EB clinical research
2) there is a degree of polarisation of opinion and experience and 3) community
development and collaboration are necessary for progress. There is much
variation in attitudes, with some reporting negative experiences of research
and low levels of motivation and others, the opposite. Findings of the patient
survey highlighted patients’ and families’ motivation to find a cure and relief
of local symptoms, but also that there are barriers to participation in the form
of fear of risks to health, additional pain and travel issues. Both branches of the
study confirmed the importance of a trusting, cooperative relationship between
members of the community.
CO N CLU S I O NS
There are many, varied attitudes towards clinical research in the EB
community which are both positive and negative. The cohort of researchers
interviewed have high levels of motivation, despite many challenges and
frequently, negative experiences. Reports of patients’ attitudes as perceived
by researchers were mixed and polarised. Data from the patient cohort is
suggestive of motivated but risk-averse attitudes. Coordinated efforts by the
EB community as a whole are necessary for the progression of research. More
investigation is needed to explore the nuances of this topic in relation to subsets
of EB and its community.
09
Original Research
Attitudes to Clinical Research within the Epidermolysis Bullosa
(EB) Community
I NTRODUCTION
In an era of rapidly evolving technologies,
medical advances are not keeping pace. This is due
to a variety of factors, including increased regulation
and decreased funding. Another pervasive factor also
requires attention – lack of patient engagement with,
and participation in, clinical trials. Low rates of patient
participation are a well-recognised barrier to clinical
trials and, thus, to the advancement of medical
research.3 , 1 0 , 1 2 , 1 3
Much research has investigated this consistently poor
engagement in research and the attitudes that lead to
it in the general population. A range of non-disease
specific attitudes and barriers to engagement have
been unearthed by others. Typical examples of these
include: a lack of trust of medicine; poor awareness
of clinical research, and lack of motivation.1 , 3 , 1 0 ,
1 2 - 1 4 Most of these attitudes may be generally
attributed to a weak relationship, and poor quality of
communication, between those involved in medical
science and the general population.3 - 7
In a disease-specific context, information from
the general population provides only some of the
answers for poor levels of participation. In rare
diseases, in particular, attitudes towards research
in their communities have not been thoroughly
analysed.
Epidermolysis bullosa (EB) is an example of one
such rare disease. Inherited EB is a group of rare
genetic skin diseases, characterised by extreme skin
and tissue fragility and recurrent blistering.1 5 There
are over 30 different genotypes and phenotypes
of the condition. The major subtypes of EB are
simplex (EBS), junctional (JEB) and dystrophic (DEB);
these are differentiated on the basis of the mutated
proteins and the level at which cleavage takes place
in the skin.1 6 EB has a reported incidence in the USA
of 19 per million live births,1 5 with EBS being the
most common type, followed by DEB and JEB.
There is no cure for EB. Medical treatment primarily
involves meticulous wound care and dressing,
nutritional support and symptomatic relief of pain
and itch. Clinical research (CR) into EB is currently
active in a variety of potential treatment domains,
including protein, cell, gene and drug therapies.
It is well known that EB patients and families want
more and better treatments. Despite this, CR and
clinical trials (CTs) are not always well enrolled
or successfully completed. The reasoning for
this poor engagement is anecdotal and not well
established. This study aimed to begin analysing
this phenomenon, by undertaking preliminary
investigations into attitudes and perceptions towards
CR, within the global EB community.
ME THOD S
This research was conducted during the
period of May-August, 2014, under the auspices of
DEBRA Ireland, on behalf of DEBRA International.
DEBRA is a patient organisation that focuses on
patient care and research. There are numerous
national DEBRA organisations around the world and
they come together under the umbrella of DEBRA
International.
The aim of the study was to gather information from
both clinical researchers involved in EB and people
living with EB about their experiences of clinical
research and their attitudes towards clinical trials.
As well as this, factors involved in patients’ and their
families’ decisions to take part in clinical trials were
to be investigated. DEBRA has a central position as a
trusted advocate in this community, which facilitated
the engagement of participants in the study.
An explanatory mixed-methods approach was
adopted. As a first step, the views of researchers were
explored through interviews. The themes emerging
from this qualitative phase were then used to guide
the design of a survey to explore the views of patients
in a quantitative manner.
I NTERV IE W S
Twenty-four senior investigators with
experience in EB clinical research were contacted
in May and June of 2014. These investigators were
either known to be involved in past or active clinical
trials and/or were listed as investigators on the main
clinical trial registries. Thirteen responded and eleven
of these were interviewed. The interviews took place
over the phone or via Skype®. Ten open-ended
questions were used to guide each conversation in a
semi-structured manner. These questions were made
available to each participant beforehand.
Confidentiality was assured at the beginning of each
interview. Consent to record the interview and for
opinions to be published on an anonymous basis
was requested. Each person was encouraged to
raise any additional topics or points of information
during the course of the conversation. Interviewees
were asked questions on a range of topics, including
their experiences of recruiting patients, the particular
issues for EB patients participating in CR and the
role DEBRA might play in supporting recruitment.
Interviewees were asked to consider the topics from
their perspective as both a researcher and a patient
10
UCD Student Medical Journal
Written by
advocate. An opportunity was given at the end of
each interview for any additional comments the
interviewee may have had.
Notes were hand written during the interview, with
key words and phrases being highlighted. During
this process, care was taken to reflect the views
of the participants accurately. These notes were
de-identified and served as the main material for
analysis. They were then reviewed on the principles
of thematic analysis.18 Patterns in the interviews
were highlighted, and emergent themes were crosschecked between interviews. A single investigator
completed the review, coding and description of
overarching themes; this approach was necessitated
due to time and resource constraints. Thus,
methodical rigor via triangulation was not available,
though there was much discussion between authors,
after the analytical framework was drafted.
The themes that emerged were used to define a
focus of questioning for the second, quantitative
phase of the study.
S U RV E Y
The survey was designed on the basis
of the outcomes of the interviews, the experiential
knowledge of DEBRA representatives and the
literature relating to general populations. It was
targeted towards patients themselves and their
parents/carers. It was an online survey, disseminated
internationally through digital media. The survey was
made available in English, so a good proficiency in
this language was required. Requests were made
to some DEBRA representatives internationally for
assistance in spreading awareness of the survey.
It was noted that the fact that they survey was
disseminated through DEBRA channels, and that
the partipants were self-selecting, might introduce
selection bias. That is, those participating were
likely to have a prior interest in the topic and to be
positively disposed towards DEBRA.
The preamble to the survey contained information
about the purpose of the study, what the results
would be used for and assured participants of
confidentiality. Moving from the introduction to the
body of questions implied consent for results to be
used in analysis.
Maeve Jones-O'Connor
Dr. Amanda McCann
Avril Kennan
The survey was hosted on SurveyMonkey Inc. (www.
surveymonkey.com). It was publically available
from June to August. Respondents were asked
nine questions in total; three of these provided the
background of the respondent; one asked about
their previous experience with clinical trials; two
asked about where they would source information;
two asked to rank the relative weight of factors
in their decision-making process. Questions took
a variety of formats, including open questions
and fixed response questions, some of which
incorporated 5-point Likert scales. There was a total
of 43 respondents to the survey. The full text of the
survey is presented in Table 1.
At close of the project, data was downloaded from
the hosting website and responses were analysed.
The results of the survey were then considered on
their own merit and in consideration of the themes
emerging from the researcher interviews.
11
→
Original Research
Attitudes to Clinical Research within the Epidermolysis Bullosa
(EB) Community
Question
Answer format
Possible answers/options
Completion
rate
1. Which option best
describes you?
Multiple choice
• I have EB
• I am a parent of child with EB
• Other
43/43 (100%)
• Mild
• Moderate
• Severe
43/43 (100%)
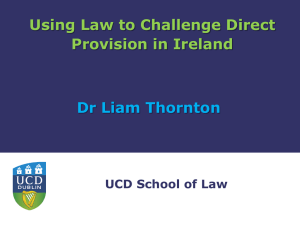
Table 1
Detail of survey
questions and
answers
2. Which of the following
Multiple choice
best describes the
severity of your EB? If
you are a parent, please
answer this and all
following questions on
behalf of your child.
3. In which continent do
you live?
Free Text
4. Which of the following
best describes you, in
relation to EB clinical
trials?
Multiple choice
43/43 (100%)
• I have taken part in one or more EB clinical trials
43/43 (100%)
• I would be very eager to take part in an EB clinical trial
• I would consider taking part in an EB clinical trial but with
reservations
• I would never take part in an EB clinical trial
• I am unsure whether I would take part in an EB clinical
trial
5. If you wanted to find out Free text
more about EB clinical
trials, where would you
go for information?
Please be as specific
as possible and you
can list more than one
source.
43/43 (100%)
6. To what extent
would the following
POSITIVELY influence
your decision to take
part in an EB clinical
trial?
Matrix of choices
(Likert scale):
Very strong
Strong
Moderate
Weak
No influence
• The possibility of a cure
• The possibility of relief from symptoms
• The potential to contribute to the advancement of EB
medical knowledge
• Having the costs of participation covered
• The likelihood of receiving expert medical care for the
duration of the trial
• Access to the treatment/intervention, following
completion
• The knowledge that it was difficult to recruit enough
patients to ensure the trial’s successful completion
37/43 (86%)
7. To what extent
would the following
NEGATIVELY influence
your decision to take
part in an EB clinical
trial?
Matrix of choices
(Likert scale):
Very strong
Strong
Moderate
Weak
No influence
•
•
•
•
•
•
•
•
•
•
The possibility of a minor risk to health
The possibility of a major risk to health
The possibility of receiving a placebo
The need for painful procedures during the trial
The treatment being limited or localised
The need to attend clinicians other than your usual ones
The need to travel a long distance to the trial centre
The need to revisit the trial centre at 2-weekly intervals
The need to revisit the trial centre at monthly intervals
The need to revisit the trial centre at 3-monthly intervals
37/43 (86%)
8. To what extent would
you trust information
from the following
people/groups, in
considering whether
to participate in an EB
clinical trial?
Matric of choices
(Likert scale):
Would definitely
trust
Would likely trust
Would cautiously
trust
Would likely not
trust
Would definitely
not trust
•
•
•
•
•
Your primary doctor
Your family
Other families who live with EB
Social networks with a focus on EB
DEBRA
37/43 (86%)
9. Finally, if there is
anything else you would
like to add, we would
really like to hear it.
Free text
8/43 (18.6%)
12
UCD Student Medical Journal
Written by
RE S U LT S
I NT E RV I E W S
Three major themes emerged from analysis
of the content of the interviews with EB clinical
researchers. These represent attitudes and ideas that
are held across the spectrum of those interviewed.
However, in a small community such as EB, the
outliers that may not be represented by broad
themes are proportionally very important. As such,
this analysis does not purport to be exhaustive.
Th e m e 1 : E B c l i ni c a l re s ea rc h i s m o re
c h a l l e ng i ng th a n ex pe c te d b y tho s e
i nvo l v e d
Many positive enabling factors exist for EB clinical
research. These include:
»»
»»
»»
good, communicative relationship between
A
EB patients and their clinicians;
A patient and family cohort who are quite
medically literate and willing to engage;
A motivated network of researchers.
However, on balance, the experience of CR is seen to
be more challenging than straightforward. Pervasive
negative factors and challenges exist, such as:
»»
»»
»»
»»
»»
»»
Many subtypes of EB, which complicates study
design;
Limited current evidence on the natural history
of EB;
Patients are small in number and geographically
scattered;
High burden of disease on the patient;
Lack of up-to-date and quality registries;
Issues with coordination between different
clinics, in some cases.
In addition to these challenges, there was some
mention of particular challenges with regulatory
bodies and other groups, such as insurance
companies. These references were noted, but not
explored in detail.
Th e m e 2 : H e te ro g e ne i ty o f o pi n i o n
o f pati e nts to w a rd s re s earc h
The researchers reported a diversity in the attitudes
to clinical research among patients. One one hand,
most reported engaging with patients who were
consistently interested and keen to be involved. On
the other hand, many had also encountered patients
who would not - or often, could not - take on the extra
burden of being engaged in research.
Maeve Jones-O'Connor
Dr. Amanda McCann
Avril Kennan
All researchers acknowledged that face-to-face
communication, such as taking extra time with
patients in clinic to explain more about research or
a particular trial opportunity, might help to postively
change attitudes to CR. Other opportunities to
spread information about research, such as speaking
at conferences, were also viewed as having a
positive effect, although most also expressed an
opinion that this was not frequently feasible. This
type of sentiment was suggestive of a sense of
frustration within the EB research community as
well. Researchers appear to be aware that flexible,
creative methods may help overcome some
challenges, but these are seen as unrealistic due to
resource constraints. Overall, clinicians were aware
that they would have to adapt and be flexible when
undertaking EB clinical research.
The m e 3: The c e n tra l ro le o f
c o m m un i ty a n d c o lla b o rati o n
The idea of there being an EB "community",
"world" or "network" was a strong theme across the
interviews. It is generally considered to consist of
patients and their families at the centre, with DEBRA,
clinicians and researchers beside them.
It appears to be agreed opinion that patients and
their advocates must be involved in clinical research
efforts on an equal standing to the researchers, if
clinical research is to be successful. Researchers’
efforts tended to be more fruitful when they
collaborated with DEBRA, for example. However,
there is a wide variation in how much the community
aspect of EB is utilised in this regard. Whether this
is due to not knowing how to collaborate, or some
members of the community being unwilling to do so,
is unclear.
Most people directly mentioned community in
their final comments. This was most frequently
expressed in the context of a desire for more unity
and collaboration, particularly within the medical
community, and between the medical community
and patient. The next most frequently mentioned
sentiment was in praise of ongoing community
building efforts.
13
Original Research
Attitudes to Clinical Research within the Epidermolysis Bullosa
(EB) Community
S URVE Y
Of the total number of survey respondents
(43), 39.53% were people with EB and 48.8% were
parents of children with EB (it was not specified
how many of their children were affected). Mild and
moderate EB were the most common severities
of EB cited (44.2% and 41.9%, respectively). The
geographical locations of respondents spanned five
continents.
Only 9.3% of respondents reported having taken
part in a clinical trial. The majority of people (76.7%)
expressed a willingness to participate in a clinical
trial; 34.88% of these reported to be "very eager" to
take part and 41.86% reported they would "consider
taking part with reservations". Only 1 respondent
(2.32%) chose the explicitly negative option of "I
would never take part in an EB clinical trial"; however,
with a small sample as this, such responses should
not be deemed insignificant.
In responding to Question 5, on where respondents
would go for information on EB clinical trials,
DEBRA was the most commonly quoted source
of information for EB clinical trials (26 mentions of
63 total), followed by search engines (“internet”
or “Google”; 16 of 63). Medical personnel
(dermatologists, nurses or clinics) were mentioned as
a source 9 times in total. Other responses included
"social media" (5), other organisations (2) and don’t
know/not sure (5).
In total, 37 of the 43 respondents completed
Questions 6 to 8. Responses to the following three
questions: “To what extent would the following
factors POSITIVELY/NEGATIVELY influence your
decision to take part in an EB clinical trial?” and “To
what extent would you trust information from the
following people/groups, in considering whether to
participate in an EB clinical trial?” are presented in
Tables 2,3 and 4.
Question 6 asked about factors that would positively influence a decision to participate in a
CT. The vast majority (75%; n=193) of scale points
chosen across all options were either “very strong”
or “strong” influence. 94.5% listed symptom relief as
either a “very strong” or “strong” influence, compared
with 89.1% for the possibility of finding a cure. Access
to the trial intervention after completion of the study
was the next most influential factor, with 78.3% of
responses showing it was either “very strong” or
“strong” influence.
Question 7 asked about factors that may negatively
influence the decision to participate in EB clinical
trials. The single most utilised scale point in this set
of answers was “moderate influence”, with 26.7%
of all responses. When the number of responses to
“very strong” and “strong” influence are combined,
the leading negative influences from this series were:
the possibility of a major risk to health (89.19% of
responses either “very strong” or “strong”) and the
need for painful procedures during the trial (64.86%).
It is interesting to note that most people ranked
travel concerns as a “moderate" influence. Overall,
the distribution of points chosen was more balanced
across the scale as compared to Question 6.
Question 8 asked about the trustworthiness of
sources within the EB community. Responses to
this question also showed a tendency towards the
positive scale points, i.e. "would definitely/likely
trust". These results are reported in Table 4. The
results also show that social media networks are more
likely to be considered trustworthy than not.
Responses to Question 9 were given in a free text
manner. 18.6% of survey respondents wrote an
answer. Two answers expressed an opinion as to
the direction research should be moving, asking for
a focus on oral and gastrointestinal issues. Three
respondents expressed surprise at the fact that it may
be hard to enroll trials adequately; they and another
expressed a desire for more information. Another
suggested having a new method of registering
interest for trials. The final respondent expressed a
desire to find a cure for EB.
14
UCD Student Medical Journal
→
Table 2
Responses to Q.6,
“To what extent
would the following
factors POSITIVELY
influence your
decision to take
part in an EB
clinical trial?”
Responses to Q.7,
“To what extent
would the following
factors NEGATIVELY
influence your
decision to take
part in an EB
clinical trial?”
15
Maeve Jones-O'Connor
Dr. Amanda McCann
Avril Kennan
Very strong
influence
Strong
influence
Moderate
influence
Weak
influence
No influence
Total
The possibility of a cure
78.38% (29)
10.81% (4)
5.41% (2)
2.7% (1)
2.7% (1)
(37)
The possibility of relief from
symptoms
75.68% (28)
18.92% (7)
2.7% (1)
0% (0)
2.7% (1)
(37)
The potential to contribute
to the advancement of EB
medical knowledge
40.54% (15)
29.73% (11)
16.22% (6)
10.81% (4)
2.7% (1)
(37)
Having the costs of
participation covered, e.g.
travel expenses
29.73% (11)
The likelihood of receiving
expert medical care for the
duration of the trial
41.67% (15)
27.78% (10)
19.44% (7)
8.33% (3)
2.78% (1)
(36)
Access to the treatment/
intervention, following
completion of the trial
45.95% (17)
32.43% (12)
16.22% (12)
0% (0)
5.41% (2)
(37)
The knowledge that it was
difficult to recruit enough
patients, to ensure the trial’s
successful completion
36.11% (13)
33.33% (12)
19.44% (7)
5.56% (2)
5.56% (2)
(36)
Very strong
influence
Strong
influence
Moderate
influence
Weak
influence
No influence
Total
The possibility of a minor risk
to health
29.73% (11)
21.62% (8)
29.73% (11)
13.51% (5)
5.41% (2)
(37)
The possibility of a major risk
to health
64.86% (24)
24.32% (9)
8.11% (3)
2.7% (1)
0% (0)
(37)
The possibility of being given
a placebo (a substance with
no therapeutic effect)
27.03% (10)
24.32% (9)
29.73% (11)
5.41% (2)
13.51% (5)
(37)
The need for painful
procedures during the trial,
e.g. injections, biopsies
29.73% (11)
35.14% (13)
18.92% (7)
8.11% (3)
8.11% (3)
(37)
The treatment being limited
or localised, e.g. treating only
1 or 2 wounds
10.81% (4)
16.22% (6)
32.43% (12)
18.92% (7)
21.62% (8)
(36)
The need to attend clinicians
other than your usual ones
10.81% (4)
13.51% (5)
27.03% (10)
24.32% (9)
24.32% (9)
(36)
The need to travel a long
distance to the trial centre
21.62% (8)
13.51% (5)
29.73% (11)
16.22% (6)
18.92% (7)
(37)
The need to revisit the trial
centre at 2-weekly intervals
10.81% (4)
24.32% (9)
32.43% (12)
10.82% (4)
21.62% (8)
(37)
The need to revisit the trial
centre at monthly intervals
2.7% (1)
21.62% (8)
27.03% (10)
27.03% (10)
21.62% (8)
(37)
The need to revisit the trial
centre at 3-monthly intervals
2.7% (1)
8.11% (3)
32.43% (12)
27.03% (10)
29.73% (11)
(37)
→
Table 3
Written by
29.73% (11)
16.22% (6)
18.92% (7)
5.41% (2)
(37)
Original Research
→
Would
definitely
trust
Would
likely
trust
Would
cautiously
trust
Would
likely
not trust
Would
definitely
not trust
Total
Your primary doctor
40.54% (15)
21.62% (8)
24.32% (9)
10.81% (4)
2.7% (1)
(37)
Your family
37.84% (14)
21.62% (8)
24.32% (9)
13.51% (5)
2.7% (1)
(37)
Other families with EB
25% (9)
38.89% (14)
30.56% (11)
2.78% (1)
2.78% (1)
(36)
Social networks with a focus
on EB
5.41% (2)
48.65% (18)
32.43% (12)
5.41% (2)
8.11% (3)
(37)
DEBRA
55.56% (20)
38.89% (14)
5.56% (2)
0% (0)
0% (0)
(36)
Table 4
Responses to Q.8,
“To what extent
would you trust
information from
the following
people/groups, in
considering whether
to participate
in an EB clinical
trial?”
Attitudes to Clinical Research within the Epidermolysis Bullosa
(EB) Community
DI S CUS S I ON
Prior to this study, the evidence relating
to the attitudes and opinions of researchers and
patients towards CR in EB was primarily anecdotal.
Being a small community with a strong network, such
evidence should not be discounted. However, this
study aimed to add to understanding of the attitudes
to EB clinical research by objective investigation.
The anecdotal evidence indicated that patient
engagement and participation in EB clinical research
is a particular issue; as such, it was chosen as a central
theme for this research. The qualitative portion of this
research acted as an exploratory phase, from which
additional themes emerged. The semi-structured
approach taken allowed these new themes to
emerge, as well as allowing specific questions to
be answered. Much information and insight into
attitudes to CR was garnered in this way.
It would be inappropriate to try and label
researchers’ attitudes to CR as wholly “positive” or
“negative” in the context of EB. The general attitude
is both broadly positive and negative – positive in
the sense that there is a great sense of motivation
amongst researchers, and negative in the sense that
they experience it to be a very challenging area of
research - indeed, of medicine in general.
The three themes that emerged on analysis of the
interviews with researchers are reflective of the more
common attitudes to research within the medical
community as a whole. However, one theme itself
must be remembered in any attempt to categorise
the attitudes towards EB CR - the prevalence of
heterogeneity, in terms of experience and of opinion.
Some researchers reported excellent and relatively
straightforward experiences; others, the opposite.
This must be kept in mind for actions taken in future.
Despite this, it would be legitimate to suggest
that the vast majority of researchers believe in
the importance of community and collaboration
between researchers, patients and their advocates,
in this area of medical research. During the course
of the interviews, this idea was either shared
explicitly or seen as an implicit part of any efforts.
However, the context in which these people were
being interviewed must be taken into account – this
research was done under the auspices of DEBRA, a
leading coordinator of the EB community, so this may
have created a kind of selection bias in the people
who chose to cooperate with this study.
The quantitative portion of the study investigated
patients’ and their families’ attitudes towards CR,
with a particular focus on the factors that influence
their participation. As such, the results of the survey
provide good data on what factors are involved
in a decision to participate. Motivation levels and
perceptions are also probed in this question set, but
in an indirect way.
The overwhelmingly positive tendency in responses
to Question 6, on factors that positively influence
participating in clinical trials (Table 2), was interesting
to note. This consistent trend to list factors as “Very
strong” or “Strong” influences suggests that patients
are open to the idea of many types of research,
from curative to localised symptom management
This is indicative of a general open-minded, positive
attitude towards CR. As well, the advancement of
medical knowledge into EB was consistently rated as
a very positively influencing factor. This demonstrates
a strong altruistic motivation to participate.
Understandably however, factors with the potential
to postively influence the patient’s own health are of
foremost consideration.
As mentioned previously, Question 7 asked about
negative factors involved in decision making. Here,
answers lacked the trend towards positive scale
points seen for Question 6, with more of a central
16
UCD Student Medical Journal
Written by
tendency. Thus, on a relative scale, the degree of
influence exerted by positive factors outweighs the
influence of negative factors (Tables 3,4). This
suggests that positive factors play a more decisive,
stronger role in decision making than negative
factors. The one strong exception to this was the
possibility of a major risk to health which was rated
as having a strongly negative influence on the
decision to participate in a clinical trial. In this case,
only 3 respondents suggested that it would not be
a "very strong" or "strong" negative influence. This
risk aversion is not surprising - the decision making
process can be seen to be akin to a risk/benefit
analysis. The higher the possible risk, the higher the
possible gain must be to overcome that barrier.
The survey data on perceived trustworthiness
of different information sources provided some
interesting, but not entirely surprising, insights.
Primary doctors were considered only slightly more
trustworthy than family members as an information
source on clinical trials. This is perhaps indicative of
the fact that primary care specialists are rarely expert
in a complex condition like EB. DEBRA was viewed as
a highly trustworthy source of information; this should
be viewed cautiously, in consideration of the fact that
all respondants were recruited through engagement
with the charity. One of the most interesting findings
here is the general positive attitude towards
information received from social media networks,
with almost half the respondents reporting that they
would likely trust EB social networks. The role of
social media in clinical trials is a new and growing
phenomenon that needs further attention. It holds
the possibility of being of massively beneficial or
hugely detrimental to CR; vested interests need
to be actively aware of what is happenening on
social media, in order to reduce the likelihood of
the latter occurring. Other social networks, such as
other families with EB, also play an important role in
the dissemination of information. Again, this is not
surprising in a small and close community. However,
such dissemination can be troublesome if the
information itself is not accurate.
One conclusion that can be drawn from the
combined results of the interviews and survey is
that patient attitudes are very variable. Reports from
interviews suggest that there are two main cohorts
of patients. One is highly motivated and positively
predisposed; they will consistently find and engage
with research, be that by general support or active
participation. The other cohort consistently do not
want to paticipate and cannot be convinced, in large
part, due to the daily burden of the disease. The
survey results do not contradict this. It is positive
Maeve Jones-O'Connor
Dr. Amanda McCann
Avril Kennan
to note that there is a well engaged and informed
cohort; similarly, it is disappointing to note that there
is a well-populated cohort that seem to be struggling
with the daily pressures of living with EB. Here is
where advocacy groups can play a very important
role. Those who are struggling need critical support
in their day to day lives; those who want to engage
with research need to be supported in their own way
as well.
It is likely that most who participated in the survey are
interested in CR; as such, the other segment of the
patient population, mentioned above, are unlikely to
be well represented in these results. It is important
that this cohort is engaged with in exploring these
topics, to get a complete picture of what opinions to
CR are and what drives participation.
L IMITAT IO NS
It should be made clear that this study does
not aim to be comprehensive. The findings are to
be used by DEBRA and others as a basis for further
research, and as a starting point from which solutions
to problems can be found. Themes which were not
possible to exlore in-depth in this study, such as the
researchers' experiences of engaging with regulators
and the implications of cross-border collaboration,
are areas in need of further investigation.
There are limitations to this piece of research, the vast
majority of which were anticipated before the project
commenced. Chief among these was the limited
timeframe available for data collection and the small
sample sizes.
CO NCLUSIO NS
Clinical research into epidermolysis
bullosa is a known to be a challenging endeavour.
We aimed to investigate the attitudes towards
clinical research within the community, by engaging
medical researchers, and patients and families.
Attitudes within the community are not homogenous,
but among those who are positively predisposed,
motivation levels are high and consistent. Patient
participation poses a particular challenge for the
progress of clinical trials. The barriers to this are well
recognised by all, but they are not insurmountable.
Engagement with clinical research is seen in the
light of perceived risks and benefits. Efforts should
be made to educate people as to what the actual
risks and benefits are, as well as minimising risk and
maximising benefits for patients and families, where
possible.
17
Original Research
Acknowledgements
DEBRA Ireland provided funding for
this project. The authors would
also like to express their sincere
gratitude to all patients, families,
advocates and medical personnel who
supported this project.
References
01 Institute of Medicine. Public
Engagement and Clinical Trials: New
Models and Disruptive Technologies:
Workshop Summary. Washington DC, USA:
Institute of Medicine; 2011. Available
from: http://www.nap.edu/download.
php?record_id=13237
02 Tweet, Marysia S. et al. Spontaneous
Coronary Artery Dissection: A
Disease-Specific, Social Networking
Community-Initiated Study; Mayo Clinic
Proceedings, 86:9 pp. 845 - 850
http://www.mayoclinicproceedings.org/
article/S0025-6196(11)65214-2/abstract
03 N.S. Sung et al. Central Challenges
Facing the National Clinical Research
Enterprise. JAMA. 2003; 289(10):
1278–1287.
04 Centre for Information and Study on
Clinical Research Participation. Study
Participant Experiences. Boston, MA,
USA: CISCRP; 2013. Available from:
https://www.ciscrp.org/wp-content/
uploads/2014/01/2013-CISCRP-StudyStudy-Participant-Experiences.pdf
05 Centre for Information and Study on
Clinical Research Participation.
Report on Research Participant
Concerns. Boston, MA, USA: CISCRP;
2009 Available from: https://www.
ciscrp.org/wp-content/uploads/2014/03/
ciscrp_research_participant_concerns.
pdf
06 Food and Drug Administration. Patient
Advocate’s Perspective on Clinical
Trials. Washington DC, USA: FDA; 2011.
Available from: http://www.fda.gov/
downloads/Training/Clinical
InvestigatorTrainingCourse/UCM340021.
pdf
Attitudes to Clinical Research within the Epidermolysis Bullosa
(EB) Community
07 Redmond JL. Tackling Patient
Recruitment Challenges in Clinical
Trials. OncLive.com. [Internet] 2014
March 26 [date cited 2014 May 28]
http://www.onclive.com/publications/
oncology-live/2014/march-2014/
tackling-patient-recruitmentchallenges-in-clinical-trials
08 American Society of Clinical
Oncologists. Social Media in Clinical
Trials – Educational Book [Internet]
Alexandra, VA, USA: ASCO; 2014.
[Date cited 2014 June 12] Available
from: http://meetinglibrary.asco.org/
content/11400101-144
09 Kairalla JA, Coffey CS, Thomann
MA, Muller KE. Adaptive trial
designs: a review of barriers and
opportunities. Trials [Internet] 2012
August 23; 13:145. [Date cited 2014
June 19] Available from: http://www.
trialsjournal.com/content/13/1/145
10 Food and Drug Administration. Guidance
for Industry: Adaptive Trial Design
for Drugs and Biologics. Washington
DC, USA: FDA; 2010. Available from:
http://www.fda.gov/downloads/
Drugs/.../Guidances/ucm201790.pdf
11 Lewis RJ. An Overview of Bayesian
Adaptive Clinical Trial Designs.
[Presentation] 2012 September;
London, UK: Berry Consultants Ltd.;
2012. Available from: http://www.
berryconsultants.com/wp-content/
uploads/2012/09/An-Overview-ofBayesian-Adaptive-Clinical-TrialDesign.pdf
12 National Institutes of Health.
ClinicalTrials.gov – Trends, Charts
and Maps. [Internet] Bethseda, MD,
USA: National Institutes of Health;
2012 Aug. [Updated 2014 June 17;
date cited 2014 June 18] Available
from: http://clinicaltrials.gov/ct2/
resources/trends
13 European Medicines Agency. EudraCT
– Secure Cumulative Statistics until
February 28, 2013. London, UK: EMA;
2013. Available from: https://eudract.
ema.europa.eu/docs/statistics/EudraCT_
Statistics_February.pdf
14 European Commission. Q&A: New rules
for clinical trials conducted in the
EU. [Internet] Brussels, Belgium:
Europa.eu; 2014 April [Updated 2014
April 2; date cited 2014 May 26]
Available from: http://europa.eu/
rapid/press-release_MEMO-14-254_en.htm
15 Inherited epidermolysis bullosa. Fine,
JD. Orphanet J Rare Dis. 2010 May
28;5:12
16 Inherited epidermolysis bullosa:
Updated recommendations on diagnosis
and classification. Fine, JD et al.
Journal of the American Academy of
Dermatology. 2014 June; 70(6): 11031126.
17 Inherited epidermolysis bullosa:
recent basic and clinical advances.
Fine JD. Curr Opin Pediatr. 2010 Aug;
22(4):453-8.
18 Joffe H, Yardley L. Content and
Thematic Analysis. In: Marks DF,
Yardley L, editors. Research Methods
for Clinical and Health Psychology.
London, UK: Sage; 2004. pp. 56-69.
18
UCD Student Medical Journal
Emergency
Medical
Services &
Emergency
Medical
Science Where Now?
Written by
Prof. Gerard Bury, MD, FRCPI, MRCGP, MICGP
Professor of General Practice
Director of the UCD Centre for
Emergency Medical Science (CEMS)
19
Expert Article
Emergency Medical Services & Emergency Medical Science Where Now?
20
UCD Student Medical Journal
Written by
A CA S E ST U DY
A small town in Ireland – in Sligo or Kerry,
Wicklow or Donegal… Mr. Kelly, a man in his 70s
complains of central chest pain and becomes very
unwell. His distressed wife has called their daughter
Emma to come and help; while they are talking, Mr.
Kelly slumps to the floor, becomes unresponsive and
appears to stop breathing.
What care will he receive? Situations like this arise
every day and are managed by a well functioning
emergency care system with volunteers and
professionals working closely together.
Emma phones 999 and is connected to the National
Ambulance Service (NAS) Control Centre, recently
centralised to a high-tech site in Tallaght, County
Dublin. A call-taker takes brief details before
recognising that the situation she describes may
well be a cardiac arrest, coded as ‘9Echo1’ (the
highest priority) on the internationally standardised
Advanced Medical Priority Dispatch System (AMPDS)
used to manage all calls. As soon as the code
appears on the computer system, a dispatcher at a
nearby desk begins to allocate resources while the
call-taker continues to talk to Emma.
The Computer Aided Dispatch system indicates
available ambulances and Rapid Response Vehicles
in the area and also automatically identifies and
alerts volunteer Cardiac First Responders or nearby
participating GPs who may be in a position to reach
Mr. Kelly before an NAS crew. While the dispatcher
juggles these assets, the call-taker asks Emma to
re-check her father and then gives simple instructions
on how to do compression-only CPR.
A local GP is making a housecall nearby when she
receives the alert and goes to Mr. Kelly’s house
immediately – Emma is doing CPR reasonably well
and continues while the GP opens her Advisory
External Defibrillator (AED) and attaches the adhesive
pads to his chest. He is in Ventricular Fibrillation
(VF) - she delivers the initial shock and immediately
resumes CPR. At that point, a volunteer Cardiac First
Responder from the local group arrives and they
begin two-person CPR, using an airway adjunct. As
they deliver a second shock, an ambulance arrives
with an Advanced Paramedic crew member; the
second shock produces a return of spontaneous
circulation and soon afterwards, Mr. Kelly’s blood
pressure is measured at 95/70, his heart rate is 68/
min and regular and his SpO2 is 95%. A 12 lead ECG
shows an anterior ST elevation myocardial infarction
(STEMI).
Prof. Gerard Bury
21
Expert Article
Emergency Medical Services & Emergency Medical Science Where Now?
There is excellent evidence that early Percutaneous
Coronary Intervention (PCI), carried out within two
hours of onset of a STEMI, is the best treatment in
terms of survival and long term benefit. Since 2012,
Ireland has had six hospitals providing round-theclock PCI facilities in their interventional cardiology
departments; the key challenge is to reach that centre
within two hours of the first ECG to show STEMI
changes. In many parts of Ireland, that time-critical
deadline is met by the joint NAS / Irish Air Corps
Emergency Aeromedical Service, introduced in 2012.
If a land ambulance is unlikely to get Mr. Kelly to the
nearest centre within those two hours, the Air Corps
AW139 will be tasked to do so. With a crew that
includes an NAS Advanced Paramedic, Mr. Kelly will
receive ongoing monitoring and analgesia during his
trip to hospital; the GAA pitches of most towns and
villages around Ireland have been mapped and act
as informal landing sites for the helicopter, which has
successfully completed hundreds of such missions
during its trial period in this role.
P ER FO R MA NCE A ND
CH A NG E
Mr. Kelly’s case study is a realistic narrative
of high quality care delivered to many patients in
recent years. However, it’s not the full story. As our
country and health service struggle with painful
financial restrictions and major structural changes,
the NAS and the broader EMS community have
faced many challenges. In recent months, the
Health Information and Quality Authority (HIQA) has
published two reports on aspects of our pre-hospital
emergency care systems; key weaknesses were
identified and recommendations for improvement
set out.1, 2 Two further reports due early in 2015 will
explore the capacity and capabilities of the NAS and
its longterm relationship with Dublin Fire Brigade,
which provides emergency ambulance services to
most of Dublin City.
Our ambulance services comprise a key part of the
emergency medical system but other components
are also vital. Our hospital systems and particularly
their Emergency Departments have experienced
major changes in funding, organisation and
roles which have significant implications for the
communities they serve. Community services,
including general practice and lay volunteers have
also had clear recognition of their roles and potential.
KEY PERFORMANCE I NDICATORS
So what has HIQA said in its analysis?
Overall, HIQA says it has concerns about NAS
performance. In all parts of our healthcare system,
performance measurement should be an integral
part of how we work and learn – it must be a tool
to help us improve, not a stick with which to beat
individuals.
Much therefore depends on how we measure
performance.
HIQA highlights an Emergency Medical Services
(EMS) system which relies on ‘legacy’ structures
and procedures and which has much work to do to
become a uniformly high quality provider of care
to all of its patients, all of the time. HIQA expresses
concern about the poor record of the NAS in meeting
the time targets for emergency responses to 999
calls, reporting that in a 15 month period, only 58%
of the most critical calls – Echo calls, – received a
response within eight minutes and only 34% of the
next most serious category – Delta calls, received a
response in the same time period.
However, is HIQA itself part of the problem? During
much of 2010 and 2011, the NAS, HIQA and the PreHospital Emergency Care Council (PHECC) worked
together on the development of Key Performance
Indicators (KPIs) for EMS. There is general acceptance
that KPIs have much to offer all health care services
and the communities we serve – however, they should
be valid (measure what it important) and reliable
(offer consistent results). In 2011, HIQA formally
required the NAS to introduce time-based targets,
as the only measure of its clinical performance –
essentially, to ensure that 75% of Echo calls received
a response within eight minutes. A timely response is
obviously critically important in cardiac or respiratory
arrest but it is not the sole determinant of the
quality of care provided. Paradoxically, a cardiac
arrest patient who receives an EMS response at nine
minutes and is resuscitated from VF (perhaps Mr.
Kelly?) is counted as an inadequate performance
issue by HIQA, whereas a similar patient who
receives a response in seven or eight minutes but
is not resuscitated, is a success story. Both NAS and
PHECC strongly advised HIQA at the time that timebased targeting by itself is a poor measure of the
performance of such a complex clinical service and
that clinical KPIs should be introduced in parallel.3
HIQA chose to rely solely on time targets – its recent
report is influenced heavily by performance against
those targets but also accepts that clinical KPIs have a
role in the future.
Many such clinical KPIs can be identified and are
likely to be introduced by individual EMS services in
Ireland and elsewhere in coming years (aspirin and
ticagrelor for STEMI, control of seizures on scene,
treated hypoglycaemia, adequate pain relief etc).
However, if the public (and the statutory regulator of
health service quality) continue to rely on surrogate
measures of performance which have limited validity,
then confidence in the EMS system may continue to
fall.
22
UCD Student Medical Journal
Written by
Prof. Gerard Bury
23
Expert Article
Emergency Medical Services & Emergency Medical Science Where Now?
Change to improve meaningful performance
(clinical care) must be our goal. Much has changed
in Irish EMS in the last decade and our systems are
unrecognisable from those of two decades ago.
But as the cliché says, much remains to be done.
Appropriate change in systems and clinical practice
will hopefully gather pace in the short term – some
examples may illustrate the changes on the way:
1 . S COPE OF PRACTICE
Paramedics and Advanced Paramedics
now deliver care that, until a few years ago, was
the exclusive domain of registered medical
practitioners and which required equipment and
skills only available in specialist hospital units.
Defibrillation, cardioversion and STEMI thrombolysis
are among those skills; potent pain relief, reversal
of hypoglycaemia and seizure control are among
the pharmacological interventions available.
Understandably, the rapid evolution of education,
skills and Clinical Practice Guidelines has focused on
‘high acuity’ problems which threaten life or limb.
E M E RG I NG CH A L L E NG E S FO R EMS
Emergency medical science and emergency medical services in Ireland face complex challenges in the coming
decade. The more obvious include:
»»
Scientific and technological change in healthcare
»»
Demographic change
»»
Funding and organisational constraints
»»
Expectations and awareness of the public
»»
Integration with the broader healthcare system
»»
Command, control and dispatch systems
»»
Clinical KPIs and standards
»»
Scope of practice, education and Continuous Professional Development (CPD)
»»
Governance and leadership: responsive or pro-active?
The next major shift in scope of practice may involve
a re-focusing on those clinical problems dealt with
by EMS which are ‘low acuity’ but very common.
Some overseas ambulance services deal with up to
40% of their callers without sending an emergency
ambulance - callers may receive advice, be referred
to an alternative service (such as their GP or an outof-hours service) with an appointment or be dealt
with on a non-emergency basis.
‘Treat and Refer’ or ‘Treat and Discharge’ procedures
carried out by Paramedics can safely and effectively
deal with many problems. Those problems might
include treated hypoglycaemia or seizures among
patients where these are well established problems
or certain types of minor injury or illness. Of
course, most experienced clinicians will say that
a problem is ‘minor’ only with hindsight and that
every presentation has the capacity to be the start
of a more serious illness. The skillsets needed are
therefore complex and new for Paramedics and
in many ways, are reminiscent of those required
by any good doctor – taking a careful history,
establishing rapport, constructing differential and
working diagnoses and formulating and negotiating
a plan. The clinician also needs to be comfortable
with taking responsibility for those decisions
and needs to cope with the uncertainty (there’s
always uncertainty…) of each clinical situation. The
education of Paramedics is therefore likely to change
considerably.
2 . PARA ME D IC E D UCATION
Traditionally (certainly for the last 50 years),
Paramedics in the UK and Ireland have been trained
after they join the workforce, by the services which
employ them. The inadequacies of this strategy have
been well recognised, so that in the UK, by 2019,
every Paramedic joining the workforce will be the
graduate of a university programme (of three or four
years' duration) which is closely aligned with the
education of doctors, nurses and other healthcare
professionals.
The introduction of third level education for future
Paramedics in Ireland is less clear. UCD Centre for
Emergency Medical Science (CEMS) has proposed
the introduction of such pathways to government
and UCD has accredited a four year Honours BSc
Emergency Medical Science programme – however,
its adoption as an option for those entering university
is subject to government decisions on funding and
how the NAS should adapt to such change. When
introduced, these programmes will incorporate the
care of high and low acuity illness and injury, the use
of complex interventions and a closer integration
of Paramedics into the education and Continuous
Professional Development frameworks used by other
healthcare professions.
24
UCD Student Medical Journal
Written by
3 . CO M M U N I TY I N T EG R AT IO N
Since 2006, UCD CEMS has run the
Medical Emergency Responders: Integration &
Training (MERIT) Project which has equipped and
trained more than 500 general practices around
Ireland to deal with cardiac arrest in the community.
The investment of more than €3 million by HSE,
Department of Health and PHECC in this project
represents one of the biggest research investments
in general practice in Ireland in the last decade –
and has paid off handsomely. We recently reported
almost 300 Cardiac Arrests with Resuscitation
Attempts (CARAs) by GPs in the first five years of
the project.4 Overall, 35% of practices reported a
CARA in the study period and almost 19% of all these
events resulted in a well patient being discharged
from hospital. Most general practices in Ireland now
have an AED and the most recent MERIT project is
linking volunteer GPs all over the country to the NAS
Control Centre, to be alerted in case of cardiac arrest
in their locality.
Lay volunteers who join CFR groups around the
country have made a great contribution to achieving
rapid responses to cardiac arrests. CFR Ireland is the
umbrella group for those local groups – their annual
conference (Respond 2015) is becoming a highlight
(www.cfr.ie).
The rapid development of a network of local
volunteer responders is a key recommendation from
HIQA, both in relation to the work of the NAS and in
its Heath Technology Assessment of AED deployment
in the community.
Prof. Gerard Bury
4. H O SP ITA L G R O UP S
In 2013, the government announced a
major re-structuring of the country’s hospital system,
by creating six networks each essentially centred on
one of Ireland’s six medical schools.5 The intention
is to ultimately have a number of trusts which have
a good deal of scope to address the needs of the
populations they serve as efficiently as possible.
It also implies that each trust may develop its own
methods to address those needs, including the care
of emergencies. It may therefore offer opportunities
for emergency medical science to research new ways
to offer such care.
‘Transport medicine’ has already been identified as
a key innovation. With the reduction in the number
of Emergency Departments which take emergency
ambulances from more than 40 to around 20,
patients with complex problems are being cared
for for longer periods. Patients who are very unwell
are also being transferred from smaller hospital to a
small number of specialist national units. The science,
logistics and training needed to deliver these diverse
forms of emergency care are being brought together,
under the auspices of the PHECC and will provide a
novel expertise within the EMS family.
IN CO NCLUSIO N
Both emergency medical science and
emergency medical services are vibrant and central
components of our health services. The challenges
and opportunities they present make them
increasingly central to academic medicine. Mr. Kelly’s
case is an example of the high quality care we can
deliver – we now need to make sure we deliver that
standard of care to whoever needs it, whenever or
wherever they are.
Much more to do…
25
Expert Article
Emergency Medical Services & Emergency Medical Science Where Now?
UCD Centre for
Emergency Medical Science
UCD CEMS was established in 2001 (under
a different name) as a teaching, research and
innovation centre. CEMS is a unit within Academic
General Practice at School of Medicine & Medical
Science (SMMS) and grew from our beginnings as
the only unit in Ireland delivering Immediate Care
training to Irish GPs – we continue to deliver about
400 training places for courses in cardiac, trauma and
paediatric care each year. MERIT (Medical Emergency
Responders: Integration & Training) a has greatly
strengthened our Immediate Care teaching by linking
teaching to the delivery of care in cardiac arrest and
the collection of high quality research data. This is
one key part of our research activities.
CEMS is the only unit in Ireland accredited to
provide both Paramedic (DipEMS) and Advanced
Paramedic (GradDipEMS) training, in association with
our partners, the HSE National Ambulance Services
College. More than 1,500 Paramedics and Advanced
Paramedics have graduated from our programmes.
The establishment of two MScEMS programmes (one
for APs and one for Doctors, Nurses and Paramedics)
has broadened our range of teaching opportunities.
CEMS also takes responsibility for components of the
undergraduate medicine programme by accrediting
all students in BLS and delivering an intense course in
emergency care skills in the Professional Completion
Module of final semester.
We work closely with partners in the HSE NAS, Dublin
Fire Brigade, Defence Forces and many others; we
look forward to working with colleagues and students
throughout UCD to bring Emergency Medical
Science to a wider audience.
References
01 Review of pre-hospital emergency care
services. HIQA, 2014.
02 Health technology assessment of Public
Access Defibrillation. HIQA, 2014.
03 Price L. Treating the clock and
not the patient: ambulance response
times and risk. Qual Saf Health Care
2006;15(2):127-130.
04 Bury G, Headon M, Egan M, Dowling J.
Cardiac arrest management in general
practice in Ireland: a 5-year cross
sectional study. BMJ Open 2013;3(5):
05 The Establishment of Hospital Groups
as a Transition to Independent Trusts.
Department of Health, 2013.
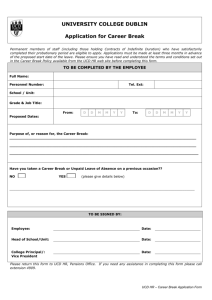
** All photos were provided by UCD CEMS
and portray Emergency First Responders
in training
Gestational
Weight Gain
and
Gestational
Diabetes
Mellitus:
Popular Beliefs
and Emerging
Evidence
Written by
Lisa A O'Higgins, Dr. Amy C O'Higgins, Sophie Gray,
Thomas McCartan, Dr. Ann Rowan, Dr. Anne Fennessey,
Prof. Michael J Turner
UCD Centre for Human Reproduction,
Coombe Women and Infants University Hospital,
Dublin 8, Ireland
27
Gestational Weight Gain, Gestational Diabetes Mellitus, Foetal
Growth, Maternal Obesity
UCD Student Medical Journal
Keywords
26
Review Article
# 1
Gestational Weight Gain and Gestational Diabetes Mellitus:
Popular Beliefs and Emerging Evidence
28
UCD Student Medical Journal
Written by
Lisa A O'Higgins, Dr. Amy C O'Higgins,
Sophie Gray, Thomas McCartan,
Dr. Ann Rowan, Dr. Anne Fennessey,
Prof. Michael J Turner
A BSTRACT
The aim of this article is to review the evidence on gestational
weight gain (GWG), and its relationship between abnormal foetal growth and
the development of gestational diabetes mellitus (GDM). Maternal obesity is a
major concern of modern obstetrics and is associated with increased maternal
and foetal complications. It is becoming increasingly common and GWG has
attracted an upsurge of interest.
In 2009, recommendations from the Institute of Medicine in
the United States revised downwards the weight gain recommendations in
pregnancy for obese mothers. There is no international consensus or guidelines
on GWG. There are concerns with evidence on GWG and many publications have
methodological shortcomings.
No causal relationship has been shown between GWG and excessive
foetal growth, however emerging evidence demonstrates a relationship
between birth weight and maternal fat-free mass. Interventions in pregnancy
aimed at targeting GWG have not shown a decrease in excessive foetal growth
and inappropriate intervention may lead to foetal malnutrition with adverse
clinical consequences. While an association between pre-pregnancy maternal
obesity and GDM has been shown, evidence of the relationship between weight
gain during pregnancy and GDM is conflicting.
A recent study has shown that fat mass gain to 28 weeks gestation
does not influence the development of GDM. Careful consideration should
be paid to the advice that pregnant women are given about GWG and their
lifestyle before, during, and after pregnancy and we believe that it may be more
appropriate to shift the focus of attention from monitoring maternal weight to
increasing physical activity levels and improving nutritional intakes.
29
Review Article
# 1
Gestational Weight Gain and Gestational Diabetes Mellitus:
Popular Beliefs and Emerging Evidence
I NTRODUCTION
Maternal obesity is a major concern in
modern obstetrics. It is increasingly common, is
associated with additional risks for both mother
and baby and gives rise to added costs to the
health services. The subject of gestational weight
gain (GWG) has attracted an upsurge of interest
in recent years, particularly as the prevalence of
maternal obesity is increasing. It is in this context
that this article aims to review the evidence on the
relationship between GWG, abnormal foetal growth
and the development of gestational diabetes mellitus
(GDM).
In 2009, the Institute of Medicine (IOM) in the United
States published a review of all existing evidence
on GWG1 . It revised GWG guidelines based on
pre-pregnancy body mass index (BMI) independent
of age, parity, smoking history, race, and ethnic
background. The focus of previous guidelines had
been on the attainment of adequate weight gain
in pregnancy so as to minimise foetal and neonatal
complications2 . The newer publication attempted
to provide guidance on the balance between
weight gain in pregnancy and outcomes for both
mother and baby. This shift of emphasis, taking into
account the possible negative outcomes associated
with excessive as well as inadequate weight gain,
resulted in recommended weight gain for obese
women during pregnancy being revised downwards.
These guidelines were based on the US population
only. There has been no international consensus on
recommendations for GWG.3
CONCERNS WITH THE
CURRE NT EVIDE NCE
Many publications on GWG have
methodological shortcomings.4 Studies on GWG
to date have been fraught with difficulties and high
quality scientific evidence is lacking.1 4 The IOM
report acknowledged that, “Unfortunately, most
of the data available to the Committee was not
collected with a high level of rigor and most studies
relied on recall weight values” (chapter 2, IOM 2009).
The accuracy of self-reported weight was reviewed
in 32 studies involving 57,172 women, and in each
study, women underestimated their weight.5 Selfreported weight leads to faulty categorisation of
BMI in 22% of cases and has led to the diagnosis of
obesity being missed in 5% of cases.6 Studies based
on self-reporting of maternal weight both underdiagnose obesity and exaggerate the risk of obesity
because women with mild obesity report themselves
in the overweight category.
There is the additional problem of timing in the
calculation of maternal BMI. In the reported studies
there is wide variance in the times when BMI is
calculated. Some studies utilised the last measured
weight before pregnancy while others utilised the
first recorded weight in pregnancy. Pre-pregnancy
weight has not been defined and in women who
are anovulatory a change in weight may stimulate
ovulation. For example, ovulation is promoted by
weight gain in underweight women and by weight
loss in those with polycystic ovarian syndrome.
During pregnancy weight is dependent on
gestational age and assessment of weight therefore
requires knowledge of gestational age. A study of
1,000 women in early pregnancy showed no change
in mean weight or body composition during the first
trimester.7 Measuring weight gain obviously requires
the measurement of weight at two different time
points. A problem arises with the timing of the repeat
measurement in pregnancy. Some studies have used
the last measured weight in pregnancy, without
account being taken of the importance of gestational
age.
In previous studies pregnancies were not dated
accurately by ultrasound and so the gestational
age at the time of the BMI calculation not known.
Some, such as the landmark Hyperglycaemia
and Adverse Pregnancy Outcome (HAPO) study,
calculated BMI only as late as 24-32 weeks
gestation.8 At this gestation, BMI does not reflect that
of early pregnancy and analysis of clinical outcomes
cannot distinguish between the influence of BMI
and pregnancy weight gain in the second trimester.
Gestational age is an important determinant not
only of GWG itself but also of the clinical outcomes
of GWG. Therefore clinical outcomes can only be
compared when there is accurate knowledge of
gestational age. This is particularly important when
examining outcomes such as birth weight or babies
classed as small-for-gestational age (SGA) or largefor-gestational age (LGA). Early pregnancy dating by
ultrasound should be a pre-requisite for any accurate
study of GWG.
30
UCD Student Medical Journal
Written by
GW G A ND A BE RRA NT
F O E TA L G RO W T H
Associations between GWG and aberrant
foetal growth have been reported, with higher
weight gain associated with LGA babies and
lower weight gain associated with SGA babies.9
However, since weight gain in pregnancy includes
the weight of the baby, it is hardly surprising that
women carrying larger babies have increased their
weight more than women carrying smaller babies.
Such epidemiological associations do not provide
evidence of causation.10
Despite a significant rise in the prevalence of
maternal obesity no increase in the number of babies
born with a birth weight in excess of 4.5 kg has
been identified.11 Studies have found, in spite of an
increase in the prevalence of obesity there has been
an associated decrease in babies with macrosomia.12
Therefore, recommendations regarding GWG and
excessive foetal growth must take into account the
evidence that causal factors for excessive foetal
growth have not been well established.13, 14
Emerging evidence demonstrates that birth weight
is related more closely to maternal fat-free mass
than maternal fat mass. A positive correlation was
found between birth weight and an increase in
maternal fat-free mass but not fat mass, in a study of
63 women.15 Previous studies showed that maternal
water gain is predictive of birth weight.16, 17 A recent
study from Dublin reported a correlation between
birth weight and maternal body composition in
2618 women studied prospectively.11 The mothers’
body composition was measured directly using
bioelectrical impedance analysis during the first
trimester. Multivariate regression analysis found that
birth weight correlated significantly with fat-free mass
but not fat mass, suggesting that attempts to reduce
maternal fat mass during pregnancy are unlikely to
decrease birth weight.
Lisa A O'Higgins, Dr. Amy C O'Higgins,
Sophie Gray, Thomas McCartan,
Dr. Ann Rowan, Dr. Anne Fennessey,
Prof. Michael J Turner
31
Review Article
# 1
GE STATIONAL DIABE TES
ME LLITUS
Even if evidence for a causal relationship between
GWG and excessive foetal growth were established,
interventions in pregnancy targeted at limiting GWG
have not been shown to prevent excessive foetal
growth. Reviews of interventions aimed at optimizing
GWG have concluded that the literature is of poor
quality and results are inconsistent.18
Gestational diabetes mellitus (GDM) has
been defined as ‘any degree of glucose intolerance
with onset or first recognition during pregnancy’.2 2
It is strongly associated with maternal obesity and
is increasingly common. Potentially it increases
morbidity for mother and baby.2 3 , 2 6 GDM also
carries a major resource-burden for maternity
services.2 4 , 2 5 Screening recommendations for
GDM vary throughout the world; in Ireland the
HSE recommends selective screening based
on the presence of risk factors.2 6 The findings
of the HAPO study showing increasing adverse
pregnancy outcomes for both mother and baby
with increasing levels of maternal glycaemia, even
below those defined as the threshold for GDM,
led to recommendations lowering the level of
glycaemia required for a diagnosis of GDM.2 7
These recommendations have been met with some
controversy, and while endorsed by the American
Diabetes Association, have not been endorsed
by the American College of Obstetricians and
Gynecologists.2 5 Micronutrient and macronutrient deficiencies in
pregnancy are associated with poorer clinical
outcomes for both mother and baby.19 Interventions
focused on losing weight during pregnancy should
ensure that the growing fetus is not deprived
of essential nutrients as a result. The promotion
of weight management programmes based on
increasing physical activity may be safer than those
focusing on dietary restrictions, with an overall
emphasis on the promotion of a healthy lifestyle.4
Attention has been drawn to an association between
obstetric morbidity and high pre-pregnancy
BMI.11, 20 Obesity in pregnancy is associated with
an increased risk of a number of serious adverse
outcomes, including miscarriage, foetal congenital
anomaly, pre-eclampsia, postpartum haemorrhage,
stillbirth and neonatal death. There is a higher
caesarean section rate and lower breastfeeding rate
in this group of women compared to women with a
healthy BMI.21 Pre-pregnancy interventions for BMI
optimisation may therefore be more successful at
reducing morbidity than interventions started during
pregnancy.
Gestational Weight Gain and Gestational Diabetes Mellitus:
Popular Beliefs and Emerging Evidence
→
Recently the UCD Centre for Human Reproduction
has examined the relationship between GWG and
the development of GDM. There were 582 white
European women with a singleton pregnancy
recruited to the study.
(KG)
20.0
Figure 1
Weight gain by
GDM status
(O'Higgins LA;
JOGS, 2014)
While the evidence for a link between pre-pregnancy
maternal obesity and GDM is strong, the association
between weight gain during pregnancy and the
development of GDM is conflicting.28 The IOM
stated an inability to comment on the relationship
between GWG and GDM due to a ‘lack of sufficient
evidence’.1 Of eleven studies reviewed by the IOM,
four showed an association between high weight
gain and the development of diabetes, three showed
an association between low weight gain and the
development of diabetes and four showed no
association between them. All but one examined
weight gain to term by which stage weight control
measures had already been commenced for women
with diabetes. All of these studies were limited by the
methodological problems previously outlined.
P < 0.001
15.0
10.0
5.0
0
-5.0
Index
NO GDM
GDM
32
UCD Student Medical Journal
Written by
Ultrasound dating of the pregnancy was performed
and only those women at less than 18 weeks
gestation at recruitment were included in subsequent
analysis. Height and weight were measured and BMI
calculated at recruitment. Body composition using
bioelectrical impedance was analysed at recruitment
and again at 28 weeks gestation. GWG and body
composition changes from baseline to 28 weeks
gestation were calculated. Women who developed
GDM (n=30) gained an average of 4.5kg by 28 weeks
gestation compared with 7.6kg in women who did
not develop GDM (p<0.001). When analysed by
BMI category the difference in weight gain between
diabetic and non-diabetic women was significant
only for obese women. No significant differences in
fat-free mass gain were found between GDM and
non-GDM women to 28 weeks gestation across any
BMI category. However the mean fat mass gain in
these obese women who developed GDM was 1.8kg
compared to 2.9kg in women who did not develop
GDM (p<0.001).29
These results provide evidence, for the first time,
that fat mass gain to 28 weeks gestation does not
influence the development of GDM. Therefore,
attempts to prevent GDM by limiting fat mass gain
during pregnancy are unlikely to be successful.
Lisa A O'Higgins, Dr. Amy C O'Higgins,
Sophie Gray, Thomas McCartan,
Dr. Ann Rowan, Dr. Anne Fennessey,
Prof. Michael J Turner
CO NCLUSIO N
GWG is a topic of increased interest
however, there are huge gaps in the research and
methodological shortcomings of studies and to date
little evidence for a causative relationship between
GWG and aberrant foetal growth or the development
of GDM has been shown. We recommend that
strategies promoting healthy pregnancy should focus
on providing resources to optimise pre-pregnancy
BMI and to promoting a healthy lifestyle in pregnancy
rather than focusing on weight gain during
pregnancy.4
33
Review Article
# 1
References
01 Institute of Medicine and National
Research Council of National Academy of Sciences. Weight gain during
pregnancy. Reexamining the guidelines.
Rasmussen KM, Yaktine AL, editors.
Washington: The National Academies
Press; 2009.
02 Institute of Medicine (Subcommittees
on Nutritional Status and Weight Gain
During Pregnancy and Dietary Intake
and Nutrient Supplements During Pregnancy, Committee on Nutritional Status
During Pregnancy and Lactation, Food
and Nutrition Board)Nutrition During
Pregnancy: Part I, Weight Gain; Part
II, Nutrient Supplements.Washington,
DC: National Academy Press; 1990
03 Alavi N, Haley S, Chow K, McDonald SD.
Comparison of national gestational
weight gain guidelines and energy
intake recommendations. Obes Rev.
2013;14:68–85.
04 O’Higgins AC, Doolan A, Mullaney L,
Daly N, McCartney D and Turner MJ ,
(2013) The relationship between gestational weight gain and foetal growth:
time to take stock?, Journal of Perinatal Medicine, 02,09.
05 Engstrom JL, Paterson SA, Doherty A,
Trabulsi M, Speer KL. Accuracy of
self-reported height and weight in
women: an integrative review of the
literature. J Midwifery Womens Health.
2003;48:338-45.
06 Turner MJ. The measurement of maternal
obesity: can we do better? Clin Obes
2011;1:127-9.
07 Fattah C, Farah N, Barry SC, O’Connor
N, Stuart B, Turner MJ. Materal weight
and body composition in the first
trimester of pregnancy. Acta Obstet
Gynecol Scand. 2010;89:952-5.
08 The HAPO Study Cooperative Research
Group. Hyperglycemia and adverse
pregnancy outcomes. N Engl J Med
2008;358:1991-2002.
09 Heslehurst N, Simpson H, Ells LJ,
Rankin J, Wilkinson J, Lang R, et al.
The impact of maternal BMI status on
pregnancy outcomes with immediate
short-term obstetric resource implications: a meta-analysis. Obes Rev.
2009;9:635–83.
10 Hill AB, The environment and disease:
association or causation? Proc R Soc
Med1965;58:295-300.
Gestational Weight Gain and Gestational Diabetes Mellitus:
Popular Beliefs and Emerging Evidence
11 Kent E, O’Dwyer V, Fattah C, Farah N,
O’Connor C, Turner MJ. Correlation between birthweight and maternal body composition. Obstet Gynecol. 2013;121:46–50.
12 Klienman KP, Oken E, Radesky JS, RichEdwards JW, Peterson KE, Gillman MW.
How should gestational weight gain be
assessed? A comparison of existing
methods and a novel method, area under
the weight gain curve. Int J Epidiomol.
2007;36:1275–82.
13 Rasmussen KM, Abrams B, Bodnar LM, Butte
NF, Catalano PM, Maria Siega-Riz A.
Recommendations for weight gain during
pregnancy in the context of the obesity
epidemic. Obstet Gynecol. 2010;116:1191–
5.
14 Turner MJ, Farah N. Gestational
weight gain and birthweight. Ir Med J.
2010;103:293–4
15 Butte NF, Ellis KJ, Wong WW, Hopkinson
JM, Smith EO. Composition of gestational
weight gain impacts maternal fat retention and infant birth weight. Am J Obstet
Gynecol. 2003;189:1423–32.
16 Lawerence M, McKillop FM, Durnin JV. Women who gain more fat during pregnancy may
not have bigger babies: implications for
recommended weight gain during pregnancy.
Br J Obstet Gynaecol. 1991;98:254–9.
17 Suitor CW. Maternal weight gain: a report
of an expert work group. Arlington: National Center for Education in Maternal
and Child Health; 1997.
18 Oken E, Gillman MW. Intervention strategies to improve outcome in obese pregnancies: focus on gestational weight
gain. In: Gillman MW, Poston L, editors.
Maternal obesity. Cambridge: Cambridge
University Press; 2012. p. 151–78.
19 Black RE, Allen LH, Bhutta ZA, Caulfield
LE, de Onis M, Ezzati M, et al. Maternal
and child undernutrition: global and regional exposures and health consequences.
Lancet. 2008;371: 243–60.
20 O’Brien T, Ray JG, Chan WS. Maternal body
mass index and the risk of pre-eclampsia:
a systematic overview. Epidemiology.
2003;14:368–74.
21 CMACE/RCOG Joint Guidelines, Management
of Women with Obesity in Pregnancy March
2010 available at http://www.hqip.org.uk/
assets/NCAPOP-Library/CMACE-Reports/15.March-2010-Management-of-Women-with-Obesity-in-Pregnancy-Guidance.pdf Royal
22 BE Metzger, DR Coustan Diabetes Care
21, B161-B167, 1998
23 Diagnostic criteria and classification of hyperglycaemia detected first
detected in pregnancy, WHO, 2013
24 Sathyapalan T, Mellor D, Atkin SL.
Obesity and gestational diabetes.
Semin Foetal Neonate Med 2010;15:8993.
25 Farren, M, Daly N, O’Higgins AC,
McKeating A, Maguire PJ, Turner MJ,
The interplay between maternal obesity
and gestational diabetes mellitus, J
Perinatal Med, 2014 Nov 11.
26 HSE Guidelines for the Management of
Pre-gestational and Gestational Diabetes Mellitus from re-Conception to the
Postnatal Period, Office of the Nursing and Midwifery Services Director,
HSE, July 2010, Dublin.
27 Hyperglycemia and Adverse Pregnancy
Outcomes (2008), New England Journal
of Medicine, 2008; 358(19):1991-2002.
28 Chu SY, Lau J, Callaghan WM, England LJ, Kim SY, Dietz PM, et al.
Maternal obesity and risk of gestational diabetes mellitus. Diabet Care
2007;30:2070-6.
29 O’Higgins LA, O’Higgins AC, Fennessey
A, McCartan T, Mullaney L, Turner MJ
Junior Obstetrics and Gynaecological
Society November 2014
UCD Student Medical Journal
Keywords
Considering
the Policy
of Indefinite
Deferral
Imposed on
MSM Blood
Donors in
Ireland
35
Blood, Safety, HIV, MSM, Blood Donation, Donor Deferral,
Risk Behaviour
34
Written by
Kevin O'Malley1
Reviewed by
Dr. Sinead McDermott, MB MRCPI FRCPath, Consultant Microbiologist,
Beaumont Hospital & Our Lady of Lourdes Hospital, Drogheda
Dr. John Lambert MD PhD, Consultant in Infectious Diseases,
Medicine and Sexual Health (GUM), Mater, Rotunda and University College Dublin
UCD School of Medicine and Medical Science,
University College Dublin, Belfield, Dublin 4, Ireland
1
Review Article
# 2
Considering the Policy of Indefinite Deferral Imposed on MSM
Blood Donors in Ireland
36
UCD Student Medical Journal
A BSTRACT
Written by
Kevin O’Malley
Reviewed by
Dr. Sinead McDermott
Dr. John Lambert
The Irish Blood Transfusion Service currently enforces a policy of
indefinite deferral (lifetime exclusion) on blood donation from Men who have
Sex with Men (MSM), a measure introduced in the 1980s in response to the
emerging AIDS epidemic. While Human Immunodeficiency Virus (HIV) continues
to affect disproportionate numbers of the MSM population in Ireland, major
advances in serological testing and a greater understanding of high risk sexual
behaviour have called into question the indefinite deferral period enforced
against MSM. In approaching this issue, various factors will be considered
and addressed. To provide context for the current donor screening policies, a
brief synopsis of two infamous contamination scandals within the Irish Blood
Transfusion Service are provided. Criteria for donor eligibility are examined, as
are modern serological testing methods used to identify blood borne pathogens.
The ontologically diverse nature of both hetero- and homo- sexual behaviour
is discussed, with reference to the latest HIV statistics in Ireland. Countries that
have revised and shortened their lifetime MSM deferral periods are considered,
as are retrospective studies of the implications these changes have had on
blood supply. Finally, recommendations are given for alterations to the current
screening system that could be made without compromising the safety and
integrity of the blood supply.
37
Review Article
# 2
Considering the Policy of Indefinite Deferral Imposed on MSM
Blood Donors in Ireland
I NTRODUCTION
A troublesome past can cast a long
shadow over any organisation, but especially one
whose sole purpose is the health of a nation.1 The
Irish Blood Transfusion Service (IBTS) (formerly the
Blood Transfusion Service Board) employs a rigorous
screening policy of potential blood donors. Aside
from the obvious paramount duty to maintain the
safety of blood product recipients, the screening
policies adopted by the IBTS embody the relics
of unfortunate past incidents at the organisation.
Specifically, two contamination scandals which were
described at the time as “the worst … in the history of
the State”2 blight the record of the IBTS and continue
to cast a shadow over two decades later.
The first of these incidents occurred during the
1970’s and involved the infection of over 1000
women with Hepatitis C through contaminated anti-D
blood products. Anti-D immunoglobulin derived
from human plasma is typically given prophylactically
to Rhesus D-negative mothers pregnant with Rhesus
D-positive babies. In such situations, ante- or intrapartum mixing of maternal and foetal blood could
trigger an immune response in the mother resulting
in significant complications in later pregnancies.
Anti-D immunoglobulin reacts with and neutralises
any foetal red blood cells that enter the maternal
circulation, before the mother’s immune system is
triggered and sensitised. Even at the time, guidelines
advised that individuals who had received a
transfusion within the preceding six months were
not eligible to donate. Unfortunately, a supply
shortage caused these guidelines to be disregarded
and plasma was obtained from donors who were
concurrently undergoing plasma exchange therapy.
Hepatitis C (known then as Hepatitis-Non-A-Non-B)
ultimately entered the Anti-D blood product supply,
infecting hundreds of recipients.
The second incident coincided with the emergence
of HIV/AIDS and involved the supply of HIVcontaminated blood plasma concentrates to Irish
haemophilia patients. Concentrates are so called
as they are compiled using plasma obtained from
thousands of donors. This pooling of donations
greatly increased the risk posed to recipients as
an entire batch could be contaminated by a single
donation. In 1974, the Irish Department of Health
granted a licence to American pharmaceutical
company Travenol for the distribution of their
concentrate product ‘Hemofil’.3 The provision of a
financial incentive for blood donations was at the
time a common practice in the United States. The
practice has since been abandoned for a number
of reasons including the emergence of research
suggesting that such remuneration attracted donors
from high-risk populations (e.g. intravenous drug
users). In addition, financial incentive meant certain
donors were less inclined to be entirely truthful when
completing screening surveys in order to avoid
rejection. In this instance, HIV-infected concentrates
were imported and distributed among Irish
haemophiliac individuals.3
The subsequent fallout from these events damaged
the reputation of the IBTS enormously. It is therefore
unsurprising that the organisation is reluctant to
revise its lifetime deferral policy of MSM blood
donation.
HIV/AID S , TH E MS M B LOOD
BAN & C URRE N T
S EROLOGICA L TE STIN G
Deferral periods - defined restriction
periods from the last time that an individual engaged
in a risk behaviour to the time they regain eligibility
to donate - are now common at blood transfusion
agencies across the globe. The theory behind such
deferral periods is that any donors infected with
a blood-borne pathogen will have seroconverted
by the time they are again eligible to donate. This
significantly reduces the likelihood of donating
within a “window period” between exposure and
seroconversion. In 1985, as the full extent of the
Acquired ImmunoDeficiency Syndrome (AIDS)
epidemic was becoming apparent, the United States
Food and Drug Administration (FDA) introduced
an indefinite deferral period, i.e. lifetime exclusion
on MSM blood donations.4 Most other countries
promptly followed suit. Given that so little was known
about HIV (other than it predominantly affected
sexually active gay men) and there were no available
tests to accurately ascertain HIV status, most will
agree this was an appropriate course of action.5
The ban was introduced in 1985 as a temporary
measure yet three decades later it is still in place in
many countries. Today in Ireland, any man who has
ever had sex with a man is excluded from blood
donation for life.
In the years that have passed since these bans
were introduced, serological testing has advanced
exponentially.6 Highly sensitive assays are used to
detect the presence of various known blood-borne
viruses and pathogens including HIV, Hepatitis B,
Hepatitis C, Human T-lymphotropic virus and syphilis.
In the case of HIV, extremely sensitive combination
antigen/antibody ELISA assays can detect the virus as
early as a week following exposure. Where infection
is suspected, the Western blot test - considered
the gold standard in HIV confirmatory testing -
38
UCD Student Medical Journal
Written by
Kevin O’Malley
Reviewed by
Dr. Sinead McDermott
Dr. John Lambert
identifies specific proteins associated with the
Human Immunodeficiency retrovirus which can be
detected in blood as early as three weeks following
initial exposure. Of most relevance to this paper is
the fact that over 99% of those infected with HIV will
demonstrate a seropositive test result within three
months.6 In light of these advancements many now
question indefinite deferral policies - indeed even
the American Association of Blood Banks (AABB)
have described them as “medically and scientifically
unwarranted”.7
There is no denying that HIV/AIDS continues to
affect a disproportionate number of MSM in Ireland
compared to their heterosexual counterparts,
statistics which are mirrored in most other Western
countries. According to the latest figures released by
the National Health Protection Surveillance Centre,
MSM accounted for the highest proportion of new
HIV diagnoses in 2013 as it has done every year since
2009. Of the total number of new diagnoses made,
131 were heterosexual while 159 were MSM.8
RI S K B E H AV I O U R & T H E DI V E RS I TY O F S E XUA L P RACT I CE
Speaking on their own behalf as well
as on behalf of the the American Red Cross, the
AABB agree that to differentiate between disease
transmission via male-male sexual activity and malefemale activity on scientific grounds is irrational.7 At
the crux of this stance lies the fact that, among both
hetero- and homo- sexual people, patterns of sexual
activity are ontologically complex and diverse.9
A major criticism of blanket bans and homogenised
risk groups are that they commit an ecological
fallacy - that is, the drawing of conclusions about
individual behaviour based on a group as a whole.
Failure to disaggregate broad population-level risk
groups means that the reported risk they embody is
obscured relative to population level statistics. It is
incorrect to infer that all men who have sex with men
engage in high risk behaviour just as it is incorrect to
assume that all heterosexual activity is low risk.9, 10
Studies on risk rarely take into account MSM in
monogamous relationships or those who engage
in low risk activity and/or regularly use condoms.
Examination of data reviewed by the Advisory
Committee on the Safety of Blood, Tissues and
Organs (SaBTO) reveals that half of MSM surveyed
had no penetrative experience and almost 45%
had only ever had one sexual partner.11 Critics also
point out that research often compares MSM and
heterosexual males despite the fact heterosexual
females are biologically at greater risk of infection
from unprotected sex.9 Nevertheless, lifetime
deferral persists: in the words of one member of the
US FDA Blood Products Advisory Committee (BPAC),
although it is “non-specific...(and)...overinclusive… it
works… because it captures the high-risk subset”.1 2
According to the IBTS website, those donors who
exhibit “a particularly high risk of carrying bloodborne viruses” are asked not to donate blood. They
further state that the total MSM exclusion policy “is
not based on sexuality or orientation, only specific
actions.” If exclusion policies are (as the IBTS claim)
truly based on specific high-risk actions, then their
donor screening policy should reflect this: at present,
it does not. Any man who has ever has sex with
another man is excluded from donation for life even
if both are negative for HIV and despite their sexual
history or the potential risk of their sexual practices. In
contrast, the deferral period for heterosexual donors
who have knowingly engaged in unprotected sex
with a person with HIV or hepatitis is only 12 months.
Comparing the zero tolerance approach to MSM
donors to that applied to risk-associated heterosexual
behaviours, the difference is arguably inequitable.
Risk associated with heterosexual behaviour is rarely
acknowledged or scrutinised in studies despite the
fact that, as epidemiologist Geoffrey Rose stated, “a
large number of people at small risk may give rise to
more cases than a small number of people at high
risk”.13, 14 For example, examination of a study by
Sanchez et al. involving over 25,168 male American
blood donors, shows that while approximately 17
contaminated donations could be attributed to
MSM who did not defer appropriately (accounting
for 6% of MSM donors), the number attributable
to heterosexual donors was approximately 418
(approximately 1.7% of heterosexual male donors).1 5
The percentage of MSM is evidently higher, however
that of heterosexual donors is significant. Despite the
high number of contaminated heterosexual samples,
the MSM figures dominate policy discussion. In
addition, there is concern that indefinite exclusion
policies perpetuate the impression in the public
psyche that HIV is a selectively "gay" disease, and that
heterosexuals are somehow at lower risk of acquiring
a sexually transmitted infection.16
39
Review Article
# 2
Considering the Policy of Indefinite Deferral Imposed on MSM
Blood Donors in Ireland
DEFERRAL POLI CIE S ABROAD
When considering viable alternatives to
the lifetime deferral policy, it is useful to look to other
countries where deferral periods have already been
revised. Leiss et al. highlight two benefits that such
a policy change might bring about. First, revised
deferral would lead to an increased pool of future
donors. This pool would consist of newly eligible
MSM donors and those who currently decline to
donate due to disagreement with the perceived
discriminatory nature of the current MSM lifetime ban.
Second, there would be a social benefit in terms of a
reduction of the stigmatising association of HIV and
homosexuality.1 7 Various studies also suggest that
revision of deferral policies can reduce the risk of an
infected donation entering the blood supply due to
improved donor compliance.1 0
Italy has one of the shortest deferral periods
exercised in the world excluding countries where no
deferral period is in place. For over a decade Italy has
used extensive assessment of donor sexual history
(both heterosexual and homosexual) to ascertain
risk and suitability.1 8 Those demonstrating ‘risk’
behaviours (e.g. sex with a HIV-positive individual)
are deferred for four months following which they
are reassessed for eligibility. Lifetime exclusion
only applies to those who have engaged in high
risk behaviour such as intravenous drug use, sexual
activity with sex workers, or sex with multiple HIVpositive partners. Crucially, studies have shown
that the absence of an MSM ban “has not led to a
disproportionate increase in HIV-seropositive MSM”
donors.1 8
Twelve-month MSM donation deferral is now
practiced in various countries including Australia,
the United Kingdom (excl. N. Ireland), Sweden,
Czech Republic and Hungary.1 Lifetime deferral was
reduced to one year in the United Kingdom (excl. N.
Ireland) following recommendations from an advisory
committee on the Safety of Blood, Tissues and
Organs (SaBTO).1 9 SaBTO concluded that the levels
of risk associated with indefinite deferral and with
12-month deferral, were no different. Recent studies
in Australia, where one-year MSM deferral has been in
place since 1997, have found no evidence of increase
in HIV transmission following the implementation of
this policy.2 0 Here, assessment takes into account not
only MSM but heterosexual risk behaviour including
males who have sex with prostitutes or intravenous
drug users, and females who have sex with males
from high-risk countries.2 1
Despite the number of countries adopting the
policy, the available literature does not unanimously
support 12-month deferral as a risk-free option.
Although no exact figures are referenced, Leiss et al.,
(2008) postulate a “low incremental risk” associated
with 12-month deferral policies that they deem an
unacceptable increased risk to the safety of blood
recipients.1 7 They cite work by Germaine et al. which
suggested an increase as high as 8% in infected
donations should a one-year deferral policy be
implemented.2 2
Beyond 12-month policies, five-year deferral periods
are another option in place in various countries. Leiss
et al., who expressed reservations about a 12-month
deferral, note that there is no evidence of risk
associated with a five-year deferral period, and thus
this alternative passes “the risk hurdle”. Subsequent
to the publication of this paper, a five-year deferral
period was introduced in Canada.5 Sanchez et al.,
also note that the risk posed by a male with 5-year
deferral from MSM activity was comparable to that of
a male who had never engaged in such activity.15, 17
New Zealand also operates a five-year deferral policy
for MSM donors.1
40
UCD Student Medical Journal
Written by
Kevin O’Malley
Reviewed by
Dr. Sinead McDermott
Dr. John Lambert
RE CO M M E N DATI O NS/ CO N CLU S I O N
Revocation or revision of policy in
jurisdictions with a history of tragedy is especially
difficult and proponents of change are likely to meet
considerable resistance.1 In light of its past, it is
understandable that the IBTS is reluctant to consider
alteration of its current donor restrictions. The
aforementioned research and examples of policies
abroad suggests that changes could be introduced to
the IBTS screening process without compromising the
safety and integrity of the blood supply.
First, the IBTS could consider shortening its MSM
deferral period to five years. While opinions
regarding 12-month deferral remain divided, research
demonstrates a consensus that five-year deferral
policies have no impact on risk. The lack of substantial
evidence of increased risk associated with such a
change calls into question whether it is necessary
or appropriate to continue such an exclusionary
policy, regardless of the state of the blood supply
or financial feasibility. As Leiss and his colleagues
(2008) eloquently state: “there are very few rules
involving noncriminal personal choices in our society
that carry, as a penalty for violating them, a lifetime
ban on being able to perform one of the noblest
acts, namely, donating blood freely and without
recompense.”17( PP51)
The current prospective donor questionnaire could
also be revised to facilitate a more comprehensive
screen of high-risk donors based on sexual behaviour
as opposed to orientation. In a paper regarding
the efficacy of excluding population-based risk
groups, Kesby and Sothern advocate practice-based
exclusion. They point out that the risk of disease
transmission varies depending on three variables:
the likelihood that an individual’s sexual partner is
infected; the nature of sexual activity engaged in; and
the frequency of exposure.9 An accurate risk screen
should therefore aim to establish such information
from all prospective donors regardless of sexual
orientation. Such a revision could only enhance the
identification of risk donors, ultimately buttressing the
safety of the blood supply.
41
Review Article
# 2
References
01 Wilson K AKKJ. Three Decades of
MSM Donor Deferral Policies- what
have we learned? Int J Infect Dis.
2014; 18 1-3. v
02 Dail Eireann Debate. Report of
the Tribunal of Inquiry into the
Blood Transfusion Service Board.
[Internet] Dublin: House of the
Oireachtas; 1997 [updated 2011 May
21; cited 2015 Jan 2]. Available
from http://debates.oireachtas.ie/
dail/1997/03/20/00017.asp..
03 Power M. Legal Responses to public
crisis: Tribunals of Inquiry and
the blood crisis in the Republic
of Ireland. J Soc Crim. 2010; 1(2
(36-63)).
04 Martucci J. Negotiating exclusion:
MSM, Identity and blood policy in
the age of AIDS. (40); 215-241.
Soc Stud Sci. 2010; 40(215-241).
05 Cohen IG FJAE. Reconsideration of
the lifetime ban on blood donation by men who have sex with men.
JAMA. 2014; 312(4 (337-338)).
06 Gilbert M KM. Don’t wait to test
for HIV. BCMJ. 2010; 52(6).
07 United States FDA. Blood Products
Advisory Committee: Transcript,
minutes of meeting, Bethesda,
MD: FDA. 2006.[CITED 2015 Jan
2] Available from http://www.
fda.gov/ohrms/dockets/ac/06/
transcripts/2006-4206t1.pdf. .
08 HSE Health Protection Surveillance
Centre. HIV in Ireland: 2013 Report. [Internet] Dublin: HSE. 2014
[cited 2015 Jan 2]. Available from
http://www.hpsc.ie/A-Z/HIVSTIs/
HIVandAIDS/SurveillanceReports/
File,14651,en.pdf. .
Author's note: In January 2015,
Irish Minister for Health Leo
Varadkar announced that he had
requested a review of the deferral
policies employed by the Irish Blood
Transfusion Service. Minister Varadkar
stated that he favours a one-year
deferral policy but that any changes
will be based on scientific evidence.
09 Kesby M SM. Kesby M & Sothern M.
Blood, sex and trust: The limits
of the population-based risk
management paradigm. Health &
Practice. 2014; 26 21-30.
10 Flanagan P. How should we assess
risk behaviour when considering
donor deferral? Reflections on the
MSM deferral. Biologicals. 2012;
40. 173-175.
11 Advisory Committee on the
Safety of Blood, Tissues & Organs
(SaBTO). Donor Selection Criteria
Review. [Internet] United Kingdom: Department of Health. 2011.
[cited 2015 Jan 2 ] Available from
https://www.gov.uk/government/
publications/donor-selection-criteria-review
12 Blood Products Advisory Committee
Considering the Policy of Indefinite Deferral Imposed on MSM
Blood Donors in Ireland
67th Meeting, Thursday September 14, 2000 transcript. US FDA
Centre for Biologics evalusation
and research, Department of Health
and Human services. Available at
www.fda.gov/ohrms/dockets/ac/00/
transcripts/3649t1.rtf.
13 Galarneau C. Blood donation,
deferral and discrimination: FDA
Donor deferral policy for men who
have sex with men. American Journal of Bioethics. 2010; 10(2).
14 Rose G. The Strategy of Preventive
Medicine Oxford: Oxford University
Press; 1992.
15 Sanchez AM SGNCea. Retrovirus Epidemiology Donor Study: The impact
of male-to-male sexual experience
on risk profiles of blood donors.
Transfusion. 2005; 45.
16 Vamvakas E. Relative Risk of reducing the lifetime blood donation
deferral for men who have had sex
with men versus currently tolerated Transfusion risks. Tranfus
Med Rev. 2011; 25 1 (47-60).
17 Leiss W TM&KDMhswmddraAaurmpTMR,
35-57 2(. Men having sex with men
donor deferral risk assessment:
An analysis using risk management principles. Transfus Med Rev.
2008; 22 1 (35-57).
18 Suligo B PSRVea. Changing blood
donor screening criteria from permanent deferral for men who have
sex with men to individual sexual
risk assessment: no evidence of a
significant impact on the human
immunodeficiency virus epidemic in
Italy. Blood Transfus. 2013; 11 3
(441-448).
19 Hurley R. UK lifts lifetime ban on
gay men giving blood. BMJ. 2011;
11(343).
20 Seed CR KPLMKA. No evidence of
a significantly increased risk
of transfusion-transmitted human
immunodeficiency virus infection
subsequent to implementing a 12
month deferral period for men who
have had sex with men. Transfusion. 2010; 50 (2722-2730).
21 Musto JA SCLMKA&KJ. Estimating the
risk of blood donation associated
with HIV risk behaviours. Transfus
Med. 2008; 18 49-54.
22 Germain M&SG. Men who have had
sex with men and blood donation:
Is it time to change our deferral
criteria? J Int Assoc Physicians.
2002 1: 86-88.
UCD Student Medical Journal
Keywords
Food
Poverty
and
Policy
in Ireland:
A Review
of the
Literature
43
Food Poverty, Ireland, Health and Behaviour in School-aged Children
(hbsc), Diet, Policy, Public Health
42
Written by
Diarmuid D Sugrue1
Edited by
Prof. Ivan Perry, MD, PhD, Professor of Public Health &
Head of the Department of Epidemiology & Public Health,
University College Cork
UCD School of Medicine and Medical Science,
University College Dublin, Belfield, Dublin 4, Ireland
1
Review Article
# 3
Food Poverty and Policy in Ireland:
A Review of the Literature
44
UCD Student Medical Journal
A BSTRACT
Written by
Diarmuid D Sugrue
Edited by
Prof. Ivan Perry
Food poverty has emerged as a public health issue in the Republic
of Ireland and Northern Ireland in the last decade. Dietary patterns have
reflected the increasing numbers at risk of or living in consistent poverty. The
aim of this literature review was to: quantify food poverty in Ireland, the effect it
has on personal health, the implications for our health system, and to examine
national policies aimed at alleviating it. The review focused primarily on research
conducted by government, public health institutes, international bodies, allisland bodies, non-governmental organisations (NGOs) and charities. A definite
trend in nutritional discrepancies across the Irish population was highlighted,
with self-reported food deprivation higher in the lowest quintiles of income
and social class. Children are particularly affected by food poverty, with 1 in
5 having reported going to school or bed hungry because of a lack of food at
home. Major problems in the calculation of food poverty in the Irish population
were found; for example many marginalised groups such as Travellers and
asylum seekers have not been included in national surveys. There is currently
no coordinated policy in Ireland to guide initiatives which might address social
inequality in dietary behaviour. Given the changed economic landscape of the
last 7 years, it is apparent that the official figures for food poverty in Ireland
must be reviewed. The creation and acceptance of a standardised measure of
food poverty is paramount in order to comprehensively understand the scale of
the issue. An updated and coordinated all-island policy is urgently needed to
prevent the impending tsunami of chronic disease caused by poor nutrition.
45
Review Article
# 3
Food Poverty and Policy in Ireland:
A Review of the Literature
I NTRODUCTION
Food poverty is defined as “the inability
to afford or have reasonable access to food which
provides a healthy
diet”.1
This term has come to
prominence in an era of plenty, where technology
has enabled the mass production of food, at ever
cheaper cost to the consumer. Much of the cheapest,
processed food on the market is high in saturated
fats, sugars and salt, and data has shown that
those on lower incomes have a diet predominantly
based around such foods. Living in poverty
shapes dietary patterns; with food affordability,
accessibility, availability and awareness being
four main determinants.2 , 3 Thus, food poverty is a
multidimensional issue encompassing economic,
cultural and social inequalities leading to poor
and social exclusion. Using three basic deprivation
indicators from SILC, and adding a fourth, a definition
of food poverty was constructed. The indicators were:
»»
Not being able to afford a meal containing meat
or vegetarian equivalent every second day
»»
Not being able to afford a roast dinner once a
week
»»
Missing at least one substantial meal over a twoweek period due to lack of money
»»
Inability to have family or friends for a meal or
drink once a month
It found that 10% of the Irish population was living in
food poverty, defined as those who had experienced
one of the first three factors in the preceding month.4
nutrition.
This figure was higher for particular groups such
Food poverty has emerged as a social policy issue in
parent families and unemployed persons in food
Ireland and Northern Ireland in the last decade, with
seminal studies by Friel and Conlon (Food Poverty
and Policy) in 2004 and Purdy et al (Food Poverty:
Fact or Fiction) in 2006 highlighting the issue in these
respective jurisdictions. This was followed by Carney
and Maître in 2012, who created a food poverty
indicator for Ireland, designed to monitor food
poverty trends on an annual basis.
The purpose of this review is to heighten awareness
of food poverty as a public health issue in Ireland,
and to critique what is being done to curb it. Part A
quantifies food poverty in Ireland, the effect it has on
personal health and the implications for our health
system; Part B examines national policies aimed at
alleviating food poverty. The review focuses primarily
on research conducted by government, public health
institutes, international bodies, non-governmental
as low income earners, with almost 1 in 4 onepoverty.4 ( P P 2 8 ) Factors 1-3 relate to affordability as
the indicator of food poverty. The fourth factor was
not considered appropriate for the final composite
measurement – it dominated a 2 out of 4 scale,
doubling the percentage of those experiencing one
or more deprivation items. Trends from 2008 to 2010
showed an increase in food poverty in this period.
2 . HBS C
Children are particularly affected by food poverty.
Health Behaviour in School-aged Children (HBSC) is
a multinational longitudinal study coordinated by the
World Health Organisation (WHO) Regional Office
for Europe. The Health Promotion Research Centre,
based in NUI Galway, was invited to join HBSC in
1994, and has so far conducted four surveys of Irish
schoolchildren (1998, 2002, 2006 and 2010).5 In
2010, it found that overall 21% of Irish schoolchildren
organisations (NGOs) and charities.
reported going to school or bed hungry because of a
in 2006. In keeping with Carney and Maître’s study,
PART A:
FOOD POVERTY I N I RE LAND
1 . FOOD POVERTY I NDICATOR
Although never measured directly in Ireland, Carney
and Maître constructed a food poverty indicator
based on Central Statistics Office (CSO) figures
contained in the annual Survey on Income and Living
Conditions (SILC) between 2004 and 2010. This
study was the first of its kind in Ireland, attempting to
distinguish food poverty from other types of poverty,
such as material deprivation, fuel poverty, financial
lack of food at home. This had increased from 16.6%
it found that children from lower socioeconomic
groups were more likely to report going to school
or bed hungry (22.7%).6 However, food poverty in
children was encountered across all social classes.
46
→
UCD Student Medical Journal
Written by
Diarmuid D Sugrue
Edited by
Prof. Ivan Perry
47
Review Article
# 3
30
28.6
Figure 1
Percentage of
children reporting
they went to school
or bed hungryby age and gender
25.2
22.5
25
20.3
18.9
Source
Food Poverty among
schoolchildren
in Ireland - HSBC
Ireland Research
Factsheet No
13.2012
17.7
Food Poverty and Policy in Ireland:
A Review of the Literature
Vulnerable groups such as the homeless, asylum
According to the latest SILC (2013), the deprivation
seekers, Travellers and those living in institutions
rate (two or more types of enforced deprivation)
were excluded from SILC 2010 and therefore the
nearly tripled between 2007 and 2013, from 11.8%
food poverty indicator 2012, as SILC is a private
to 30.5% of the population.13 Given 3 of the 11
household survey. The Department of Social
“deprivation items” are food related,4(PP14) and
Protection commented at the time that this “limited”
the inadequacies in research alluded to previously,
the findings. Carney and Maître also failed to indicate
Carney and Maître’s 10% figure must be reviewed.
geographical variations in food inequalities across
the country. With Friel and Conlon having identified
these issues eight years previously,3 ( P P 4 2 ) it seems
20
there have been major, and as yet unrectified,
structural problems in how food inequality in the Irish
population has been quantified over last 10 years.
15
10-11 years old
Index
BOYS
12-14 years old
15-17 years old
GIRLS
3 . S O CI O E CO NO M I C VA R IAT IO N
Population-based studies worldwide have repeatedly
shown that people from lower socioeconomic groups
have less healthy dietary
habits.7,8
The Survey on
CR IT ICA L A NA LYSIS
Self-reported food deprivation was higher
in the lowest quintiles of income and social class in
each of the studies. Thus, there is a definite trend in
Lifestyle and Attitude to Nutrition (SLÁN) 2007
nutritional discrepancies across the Irish population.
noted that consumption of foodstuffs advocated by
Carney and Maître composed their index based on
healthcare professionals as being health promoting
three food deprivation items as this was considered
(such as low-fat milk, fruit, and white meat) is
more appropriate than using each item individually,
lower among the lowest socio-economic quintiles.
and more accurate as people may restrict spending
Conversely, consumption of fried foods at least four
in one area but may not in another.4(PP24) The
times per week was higher in every age group for
specificity of the “unable to afford family and friends
men and women in this bracket.9 Factors contributing
for a meal or drink” item was low, given how it
to this include affordability, accessibility, availability
augmented measurements. However, exclusion
and awareness. Although SLÁN pinpointed
of this item prevented measurement of the social
education as the dominant socio-economic factor by
participatory aspect of food poverty.
→
35
Figure 2
30
Poverty and
Deprivation Rates
by year - & of
individuals
25
Source
Centra Statistics
Office (CSO).
Survey on Income
and Living
Conditions (SILC)
2013
20
15
10
5
0
2004
Index
2005
2006
2007
AT RISK POVERTY
2008
2009
DEPRIVATION
2010
2011
2012
2013
CONSISTENT POVERTY
HBSC is a school-based survey with data collected
158 randomly selected schools have been completed
through self-completion questionnaires administered
for Ireland’s fifth instalment, and these data will offer
socially disadvantaged groups display awareness of
The available data on food poverty in Ireland are
by teachers in the classroom. Schools from across
a more up to date picture when they are published
what constitutes healthy eating, yet are constrained
now dated - Carney and Maître’s and HSBC’s figures
the country are randomly selected and invited to
in 2015.
Given the inverse
both come from 2010. Likewise, although important
participate. The strength of this research lies in
relationship between energy density of foods and
studies, the figures contained in Friel and Conlon
its longitudinal nature and standardisation across
Carney and Maître provide the most comprehensive
cost10 , it comes as no surprise that diets for those
(2004)3 for the Republic of Ireland and Purdy et al
participant countries, allowing direct comparison
guide for assessing food poverty in Ireland, and it
with limited resources are dominated by processed
(2006)12 for Northern Ireland are too dated so as
between jurisdictions. It also departs from previous
is certainly a persuasive and valuable document.
grains, fats and sweets. Although contentious, a
to be accurate given the economic changes of the
Irish convention of quantifying food poverty by
However, like Friel and Conlon and Purdy et al (whose
recent meta-analysis from the Harvard School of
last decade. As previously mentioned, no direct
affordability, instead focusing qualitatively on
figures focused primarily on Household Budget
Public Health comprehensively concluded that
population-wide analysis of food poverty has ever
the social and health impacts of food poverty on
Surveys), the indicators for food poverty were based
healthier diets cost significantly more than unhealthy
been carried out in Ireland – like previous studies,
children.5 However, one must take into account the
on affordability of food. The study then could only
ones in developed countries.11
Carney and Maître used secondary data analysis,
subjectivity of self-reported data, especially as this
allude to the more composite picture of food poverty
not designed to specifically answer their research
survey is carried out with young children, whilst also
incorporating accessibility, education, location and
questions. This limits the accuracy of the measures
noting how random selection of schools could miss
social exclusion. Unfortunately, this food poverty
used. SILC does not measure access to food, nor the
out on potential “black spots” of food deprivation
indicator stands alone in an Irish context; without
nutritional quality of that which is affordable.
across the country. Irish children are among those
detracting from its importance, it is therefore difficult
which nutrients vary, Friel and Conlon concluded that
primarily by affordability.3
( PP67)
from 43 countries taking part in HBSC 2014. As of
October 2014, nearly 10,000 questionnaires from
to critique in relation to anything else.
48
UCD Student Medical Journal
Written by
Diarmuid D Sugrue
Edited by
Prof. Ivan Perry
E F F E CT O N H E A LT H
The role of diet in chronic diseases such
stroke, obesity, and certain cancers has been well
documented since Ancel Keys’ “Seven Countries
Study” was first published in
1963.14
There has been
much debate in the interim as to what constitutes
the optimal diet; nonetheless there is a general
consensus that fresh fruits and vegetables, whole
communicable (chronic) diseases accounted for
(SVP) are all involved in the direct provision of food,
years of age in Ireland were overweight or obese.1 5
88% of total deaths in Ireland.2 0 With an ageing
with SVP alone spending €22 million on food and
However, obesity rates are not evenly distributed
population, this is set to rise. In 2009, the cost of
cash assistance in 2011.23 New charities such as
across society; the Survey of Lifestyle, Attitudes &
overweight/obesity in the Republic of Ireland was
Foodcloud use mobile apps to connect businesses
Nutrition in Ireland (SLÁN 2007) shows a clear social
estimated at €1.13 billion, and for Northern Ireland,
with surplus food to charities who can distribute it.
class pattern for obesity in Ireland.9
€510 million.2 1 With poor diet a major factor in
epidemic. A comprehensive analysis of worldwide
obesity prevalence carried out by The Lancet in 2013
found that 66.4% of men and 51% of women over 20
chronic disease, we are clearly in need of robust
public policies to address it in order to reduce the
food high in salt, added sugar and saturated/transfats.
Figure 3
Percentage selfreported as obese
in each social
class
Source
SLÁN 2007: Survey
of Lifestyle,
Attitudes and
Nutrition in
Ireland: analysis
by author
Food Poverty and Policy in Ireland:
A Review of the Literature
The charity sector has taken on much of the
grains, lean meat and fish are preferable to processed
→
Review Article
# 3
E FFE CT ON HE ALTH S E RVICE
According to a 2011 WHO report, non-
Ireland has not been spared from the global obesity
as hypertension, coronary heart disease, diabetes,
49
19
Crosscare and The Society of St. Vincent de Paul
2 . STATE PROV IS ION
Food cost, welfare, and direct provision are all
burden on our health system.
intervention targets. Employment is the central theme
with recent criticism that minimum wage falls below
18
burden of alleviating food poverty. Focus Ireland,
PART B: POLI CY
There is currently no coordinated policy
of poverty eradication policy in Ireland. However,
a “living wage”, it seems that employment alone does
in Ireland to guide initiatives which might address
not prevent poverty. The benchmarking of welfare
social inequality in dietary behaviour2 ; this despite
payments to average industrial earnings called for by
16
the undoubted rise in food poverty over the last
Friel and Conlon and other commentators is idealistic
number of years, particularly since the financial crisis
and unlikely given the country’s finances. In terms
15
of 2008. Friel and Conlon’s “Food Poverty and Policy”
of food cost, the reform of EU Common Agricultural
(2004) is now ten years old, yet remains the most
Policy (CAP) under Irish Presidency in 2013 may lead
applicable policy document in this area. Following
to increased competitiveness and reduced cost to the
its publication, an all-island charity, Healthy Food for
consumer. The removal of restrictions on production
All (HFfA), was set up to address the issue, supported
volume of dairy products will reduce prices, whilst
primarily by the Department of Social Protection
potentially driving other farmers towards vegetable
(DSP), Health Service Executive (HSE) and SafeFood.
or tillage farming. Although there is still an issue of
17
14
13
12
11
food waste, €3.5 billion has been allocated to the
10
SC 1-2
Index
MEN
SC 3-4
SC 5-6
WOMEN
‘Growing up in Ireland’ (2009) echoed this; 19% of
Self-reported health quality is inversely proportional
boys and 18% of girls from professional households
to food
were overweight/obese, while 29% of boys and
going to school or bed hungry in HBSC Ireland
38% of girls from semi- and unskilled social-class
2010 were less likely to report excellent health and
households were
overweight/obese.16
International
poverty.4(PP36)
Children who reported
feeling happy about their lives. They were more likely
The two pillars in addressing of food poverty have
Fund for European Aid to the Most Deprived for
been community-led initiatives and state provision.
2014-2020, to redistribute surplus food.24
1 . COMMUNITY BAS ED
Direct provision through the Schools Meals
Between 2003 and 2007, SafeFood – Ireland’s cross
Programme operated by the DSP provides food
border food safety and nutrition body – funded a
services for disadvantaged children. Currently, this
community-based project in Armagh and Dungannon
is implemented on a case-by-case basis, targeting
called Decent Food for All (DFfA). This was the
those most in need, incorporating over 60,000
first initiative specifically aimed at tackling food
children. The long-term objective is that all school-
poverty and obesity in deprived areas. It focused
going children should have access to meals in their
on educational sessions and practical workshops
school setting. Nutrition guidelines are in place for
to overcome the barriers of financial access,
each meal with breakfast, lunch and snacks aimed
physical access, and education.2 2 Similarly HFfA
at providing 25%, 33%, and 10% of recommended
daily allowance respectively.25 Since 2007, the Food
data reaffirm that the highest rates of obesity
to report current smoking, being injured, frequent
are found among minorities and the working
emotional and physical symptoms and to have
poor.17,18 Given that food poverty necessitates
bullied others.6 This suggests that food poverty has
the consumption of low cost (and therefore)
consequences for both physical and mental health.
has coordinated and promoted community food
initiatives since 2010. These include food growing
Dudes Healthy Eating Programme has been rolled
and these foods increase the risk of obesity and
It is clear that living in poverty directly affects food
projects, community food centres, education, food
out in primary schools across Ireland to encourage
cardiovascular disease, it is safe to say that food
intake, and therefore health status. In their 2008
banks and meals on wheels. Projects are awarded a
children to eat more fruit and vegetables. This has
poverty is a major contributing factor to the high
report for Combat Poverty Agency, Farrell et al
maximum of €45,000.2
now been augmented by the EU School Fruit scheme,
rates of obesity seen among lower socio-economic
reported that almost half (47%) of those who were
groups in Ireland. Thus, obesity is a socio-economic
consistently poor in Ireland reported they were
phenomenon with food poverty as a major risk factor.
suffering from a chronic illness, compared to just
energy dense foods high in fats and refined sugars,
23% of the general population.19 This reaffirms the
inextricable link between food poverty and chronic
illness.
and the Department of Agriculture aims to have run
the programme in 96.6% of all primary schools by the
end of the 2014/15 school year.26
50
UCD Student Medical Journal
Written by
Diarmuid D Sugrue
Edited by
Prof. Ivan Perry
CRI TI CA L A NA LY S IS
While the DFfA project was promising,
it was carried out in a small an area and there was
no follow up of participancts.. Although there was
positive feedback from those who participated in
the workshops, the level of understanding of term
“healthy eating” actually decreased during the
intervention period, and DFfA had no impact on
the percentage of adults who were overweight or
obese.22( PP53)
Comparatively, HFfA has no data
about how the community-based projects it runs
have alleviated food poverty. Although charity may
be beneficial, it is supportive not curative, and should
not be considered a sustainable policy.
potential benefits. Not only does this ensure that
children receive a balanced food intake, but can
educate them about what comprises a nutritious
meal. A move towards universal provision ensures
that all children benefit from enhanced nutrition
without those who need it most being stigmatised.
Secondary school interventions must also be
considered. Ireland has subscribed to international
agreements such as WHO’s Rio Political Declaration
on Social Determinants of Health (2011) and EU-2020,
aimed at reducing health inequalities. Healthy Ireland
2013 to 2025, the national framework for improving
health and wellbeing launched by the Department of
Health in 2013, recognises that “broad based policy
approaches are needed [...] to ensure that health is
an integral part of all relevant policy areas, including
environment social and economic
policies”.27
Healthy
Ireland’s council includes representation from HFfA
on the issue of food poverty. However much of this
framework is yet to be implemented and, despite
Carney and Maître’s stated aim of having their
indicator used to monitor food poverty trends on an
annual basis,4( PP11) there has seemingly been little
follow up from government on this issue outside of
the primary-school interventions already in place.
Review Article
# 3
“Health Literacy” is a concept which carries cache
References
in recent public health thinking; thus policies in
01 Institute of Public Health in
Ireland. Food poverty [Internet].
Dublin: Institute of Public Health
in Ireland; 2011 [cited 2014 Oct
07] Available at: http://www.publichealth.ie/healthinequalities/
foodpoverty.
Ireland have mirrored those worldwide which
have tended towards educating the consumer, as
opposed to modifying the food environment, to
remove disparities in healthy food consumption
across socioeconomic groups.10 Altering the food
environment pertains to reducing the cost of healthy
food while improving the nutritional value of cheap
food. This would mean lobbying industry, with
proposed measures including curbing advertising on
foods high in fat, salt and sugar, and the introduction
of a 20% tax on soft-drinks in conjunction with
subsidies for healthy food options.28 However
as Friel and Conlon pointed out, “the strength of
Resourcing the School Meal Programme has many
51
the food and agriculture industry should not be
undervalued in determining the food economy and
market”.
CO NCLUSIO N
The lead editorial in The Lancet in May
2014 warned how food poverty “lay at the heart of
appalling health”.29 The same issue contained an
open letter addressed to UK Prime Minister David
Cameron signed by 170 members of the United
Kingdom Faculty of Public Health, warning of the
looming public health crisis, and calling for an
independent advisory board to monitor nutrition and
hunger status. Given the analogous crisis in Ireland,
similar initiatives are required here. Firstly, it is evident
that the creation and acceptance of a standardised
measure of food poverty that includes all of society is
paramount in order to comprehensively understand
the scale of the issue. Secondly, an updated and
coordinated all-island policy is urgently needed,
coordinating numerous sectors: public health, social
work, charity, education and local government.
Finally, this policy should not merely focus on
education and community work, but on challenging
industry to improve our food environment. With
the impending tsunami of chronic disease caused
by poor nutrition, resolving food poverty should be
central to health policy in Ireland.
02 Healthy Food for All. Food poverty
[Internet]. Dublin: Healthy Food
for All; 2014 [cited 2014 Oct 21]
Available at: http://healthyfoodforall.com/food-poverty/
03 Friel S, Conlon C. Food poverty and policy. Dublin: Combat
Poverty Agency; 2004 [cited 2014
Oct 30] Available at: http://
healthyfoodforall.com/wp-content/
uploads/2013/11/FoodPovertyAndPolicy_2004.pdf
04 Carney C, Maître B. Constructing
a food poverty indicator for Ireland. Dublin: Department of Social
Protection; 2012 [cited 2014 30
Oct] Available at: http://www.
welfare.ie/en/downloads/dspfoodpovertypaper.pdf
05 NUI Galway. Health behaviour in
school-aged children (HSBC):
background information [Internet].
Galway: Health Promotion Research
Centre; last updated 2014 Jul 31
[cited 2014 Oct 21]. Available
at: http://www.nuigalway.ie/hbsc/
hbsc_ireland_background.html
06 Callaghan M and the HBSC Ireland Team. Food poverty among
schoolchildren in Ireland – HBSC
Ireland Research Factsheet No 13.
Galway: Health Promotion Research
Centre; 2012 [cited 2014 Oct 21]
http://www.nuigalway.ie/hbsc/documents/2010_fs_13_food_povertyjan.pdf
07 Darmon N, Drewnowski A. Does social class predict diet quality?
Am J Clin Nutr [Internet]. 2008
[cited 2014 Oct 21]. Available at:
http://ajcn.nutrition.org/content/87/5/1107.full
08 Konttinen H, Lähteenkorva S, Silventoinen K, Männistö S, Haukkala
A. Socio-economic disparities in
the consumption of vegetables,
fruit and energy-dense foods: the
role of motive priorities. Public
Health Nutr [Internet]. 2012 Aug 3
[cited 2014 Oct 21]; doi:10.1017/
S1368980012003540 Available at:
http://journals.cambridge.org/
download.php?file=%2FPHN%2FPHN16_0
5%2FS1368980012003540a.pdf&code=49
9da552b0cb80a00e528452fc6608c7
09 Morgan K, McGee H, Watson D, Perry
I, Barry M, Shelley E, Harrington
J, Molcho M, Layte R, Tully N,
van Lente E, Ward M, Lutomski J,
Conroy R, Brugha R. SLÁN 2007:
Survey of Lifestyle, Attitudes &
Nutrition in Ireland: Main Report.
Dublin: Department of Health and
Children; 2008
Food Poverty and Policy in Ireland:
A Review of the Literature
10 Drewnowski A, Darmon N. Food
choices and diet costs: an economic analysis. J Nutr [Internet]
2005 [cited 2014 Oct 21]. Available at: http://jn.nutrition.org/
content/135/4/900.full
20 World Health Organisation. Noncommunicable diseases country profiles – Ireland. WHO Europe: 2011
Sep [cited 2014 Oct 30] Available
at: http://www.who.int/nmh/countries/irl_en.pdf?ua=1
11 Rao M, Afshin A, Singh G,
Mozaffarian D. Do healthier
foods and diet patterns cost
more than less healthy options? A systematic review and
meta-analysis. BMJ Open [Internet] 2013 [cited 2014 Oct 21];
doi:10.1136/bmjopen-2013-004277
Available at: http://bmjopen.
bmj.com/content/3/12/e004277.
full?sid=820d6e1a-280e-47a6-b8c5498bfa4657e3
21 SafeFood. The cost of overweight and obesity on the Island
of Ireland – executive summary.
Dublin: 2012 Nov [cited 2014 Oct]
Available at: http://www.safefood.
eu/safefood/media/safefoodlibrary/
documents/publications/research%20
reports/final-exec-summary-theeconomic-cost-of-obesity.pdf
12 Purdy J., McFarlane G., Harvey
H., Rugkasa J. and Willis K. Food
Poverty Fact or Fiction? 2006.
Belfast: Public Health Alliance
13 Central Statistics Office (CSO).
Survey on income and living conditions (SILC) 2013. Dublin: CSO;
2015 Jan 21[Cited 2015 Jan 27]
Available at: http://cso.ie/en/
releasesandpublications/er/silc/
surveyonincomeandlivingconditions2013/#.VMvGSv6sWSp
14 Seven Countries Study. About the
study [Internet]. 2014. [Cited
2014 Oct 21] Available from
http://sevencountriesstudy.com/
about-the-study
15 Ng, M. et al. Global, regional,
and national prevalence of overweight and obesity in children
and adults during 1980–2013: a
systematic analysis for the Global
Burden of Disease Study 2013. Lancet 6736, 1–16 (2014)
16 Economic and Social Research
Institute. Growing up in Ireland.
Dublin: 2009 [cited 2014 Oct 30]
Available from: http://www.growingup.ie/
17 Paeratakul S, Lovejoy JC, Ryan
DH, Bray GA. The relation of gender, race and socioeconomic status
to obesity and obesity comorbidities in a sample of US adults.
Int. J. Obes Relat Metab Disord:
2002 Sep; 26(9): pp1205-1210
18 Flegal KM, Carroll MD, Ogden CL,
Johnson CL. Prevalence and trends
in obesity among US adults, 19992000. JAMA: 2002 Oct 9; 288(14):1723-7
19 Farrell C, McAvoy H, Wilde J and
Combat Poverty Agency. Tackling
health inequalities – an all-Ireland approach to social determinants. Dublin; Combat Poverty
Agency/Institute of Public Health
in Ireland; 2008 [cited 2014 Oct
30] Available at: http://www.
publichealth.ie/files/file/Tackling%20health%20inequalities_0.pdf
22 Balanda KP, Hochart A, Barron S,
Fahy L. Tackling food poverty:
Lessons from the Decent Food for
All (DFfA) intervention. Dublin:
Institute of Public Health in Ireland, 2008
23 The Society of St. Vincent de
Paul. Pre Budget Submission 2014.
Dublin: SVP; 2013 Jun [cited 2014
Oct 30] Available at: http://www.
svp.ie/getattachment/d93aed215bdf-43ef-ad20-1519f9500078/SVPPre-Budget-Submission-2014.aspx
24 European Federation of Food Banks.
European food aid [Internet].
FEBA; 2010 August [cited 2014 Oct
30] Available at: http://www.
eurofoodbank.eu/portail/index.
php?option=com_content&view=catego
ry&layout=blog&id=26&Itemid=45&lang=en
25 Department of Social Protection.
Urban & district school meals
meals schemes [Internet]. Dublin:
DSP; Updated 2008 Sep 30 [cited
2014 Oct 30] Available at: http://
www.welfare.ie/en/Pages/Publication---Urban-_-District-SchoolMeals-Meals-Schemes.aspx
26 Department of Health. Healthy Ireland 2013 to 2025. Dublin; 2013.
Available at http://www.hse.ie/
eng/services/publications/corporate/hieng.pdf
27 Department of Agriculture, Food
and the Marine. Strategy for
school fruit scheme submitted by
Ireland under Council Regulation
(EC) No 1308/2013 & Commission
Regulation 288 of 2009 for the
2014/2015 school year. Dublin;
2014 [cited 2014 Oct 30] Available at: http://ec.europa.eu/
agriculture/sfs/documents/strategies-2014-2015/ie_national_strategy2014_2015_en.pdf
28 Royal College of Physicians of
Ireland Policy Group on Obesity.
The race we don’t want to win:
Tackling Ireland’s obesity epidemic. Dublin: RCPI; 2014 Aug
29 Horton R. Economic austerity, food
poverty, and health [Editorial].
The Lancet 2014 May 10. 383(9929):
1609
The Use of Aspirin
for Primary
Prevention of
Cardiovascular
Disease:
Review of Literature
and Sample
Evidence of
Common
Practice in Ireland
Written by
John Travers1
Edited by
Dr. Helen Gallagher PhD, Senior Lecturer,
School of Medicine and Medical Science, University College Dublin
UCD School of Medicine and Medical Science,
University College Dublin, Belfield, Dublin 4, Ireland
1
53
Aspirin, Cardiovascular Disease, Primary Prevention, Bleeding Risk,
GP Practice, Audit, Preventative Medicine
UCD Student Medical Journal
Review Article
# 4
O
The Use of Aspirin for Primary Prevention of Cardiovascular
Disease: Review of Literature and Sample Evidence of Common
Practice in Ireland
OH
O
O
Key words
52
54
UCD Student Medical Journal
Written by
John Travers
Edited by
Dr. Helen Gallagher
A BSTRACT
The use of aspirin and broader anti-platelet therapy is well
established for secondary prevention of cardiovascular (CV) events such as
myocardial infarction, stroke or transient ischaemic attacks. However, there
is significant and growing evidence in the literature to conclude that the net
benefits from taking aspirin for primary prevention (an unlicensed indication) are
minimal and are counter balanced by harms such as gastrointestinal and extracranial bleeding.
Audits of GP practices suggest that prescription of aspirin for primary
prevention is in fact common, despite the risks. Almost a fifth of patients taking
aspirin in two practices in Dublin and Cork use the drug for primary prevention.
The risks and potentially fatal complications of bleeding should
be carefully considered and discussed with patients when prescribing aspirin
for secondary prevention of CV events and, on the basis of the most recent
evidence, aspirin should not be routinely prescribed for primary prevention. A
broader preventative approach such as addressing modifiable risk factors with
patients at planned health checks can instead yield better overall outcomes.
Guidelines on the use of aspirin in prevention of CV events should be updated to
reflect the bleeding risks outlined in recent research.
55
Review Article
# 4
The Use of Aspirin for Primary Prevention of Cardiovascular
Disease: Review of Literature and Sample Evidence of Common
Practice in Ireland
I NTRODUCTION
Aspirin and its precursors have played
a role in healthcare for millennia. It is said that
Hippocrates offered pregnant women willow leaves
in order to ease labour pains c400BC. The active
ingredient of this traditional analgesic, salicylic acid,
was first extracted from willow in the 19th century.
Aspirin was synthesised by adding an acetyl group
to salicylic acid to make it more tolerable for taking
orally. Although one of the earliest drugs developed,
aspirin is today one of the most commonly taken. Its
use has expanded from pain relief to helping in the
management of conditions such as cardiovascular
disease (CVD), colon cancer and dementia.
Aspirin irreversibly inhibits cyclooxygenase (COX)
enzymes that produce the prostanoid mediators
of inflammation, resulting in anti-inflammatory,
analgesic and antipyretic effects. COX inhibition
also blocks aggregation of platelets. This reduces
the risk of myocardial infarction (MI) or stroke due to
thrombus formation following atherosclerotic plaque
rupture.
The mechanism by which platelet aggregation
is blocked begins with COX enzyme acetylation.
There is a consequent reduction of thromboxane
A2 (TXA2) synthesis in platelets and prostaglandin
I2 (PGI2) synthesis in vascular endothelium. TXA2
promotes platelet aggregation by up-regulating
integrin surface receptors that cross-link other
platelets with fibrinogen to stabilize a platelet
plug, while PGI2 inhibits aggregation by disrupting
arachidonic acid induced adhesion. TXA2 can only
be replenished by new platelets that develop after
about 10 days. However, PGI2 can be renewed much
sooner by vascular endothelium. Therefore, the
overall balance of activity is shifted against platelet
aggregation. A low dose of aspirin is efficacious due
to the irreversibility of COX enzyme inhibition and
an accumulation effect over a few days. Some 50%
of TXA2 is suppressed with a first dose of aspirin.
A second dose increases suppression to 90% and
full suppression can be maintained by a regular low
dose.1 , 2
The beneficial use of aspirin as an anti-platelet
therapy is widely accepted in secondary prevention
of CV events.3 However, the anti-platelet effect also
increases the risk of bleeding. For patients who have
not yet experienced a CV event, the benefits of the
anti-platelet effect in primary prevention of CV events
do not outweigh the bleeding risks associated with
aspirin.
STUDIE S ON E F F E CTIV E N E S S OF AS P IRIN US E IN PRIMARY P RE V E N TION
Multiple published studies consistently
show that the use of low dose aspirin for primary
prevention of CV events does not provide net benefit
to patients. Perhaps the most comprehensive of
these studies in recent years was the Antithrombotic
Trialists’ Collaboration in 2009.4 Researchers
assessed trials of aspirin use in 95,000 individuals
in primary prevention and 17,000 individuals in
secondary prevention. They undertook collaborative
meta-analyses of serious vascular events (i.e., MI,
stroke, vascular death) as well as major bleeds. They
found that aspirin allocation for primary prevention
yielded a 12% reduction in serious vascular events
(mainly due to a reduction of just under a fifth of
non-fatal MI) though had no significant net effect
on stroke and no significant difference in vascular
mortality was found. However, they found that aspirin
use increased major gastrointestinal and extra-cranial
bleeds by just over 40%. The study strongly supports
the view that aspirin does not achieve net benefit in
primary prevention as the reduction in CV events is
offset by an increase in major bleeds.
The point is further underlined by researchers at
the Drugs and Therapeutics Bulletin. They reviewed
several meta-analyses in 2009 and found that the
benefits of MI or stroke prevention do not outweigh
the increased risk of gastrointestinal bleeding.5
They proposed that the use of low dose aspirin for
primary prevention of MI and stroke in patients with
no CVD had no effect on mortality and should not be
routinely initiated, even in those with elevated blood
pressure or diabetes. Furthermore, they suggested
that people currently on aspirin for primary
prevention should review with their doctor whether
to continue taking the drug.
56
UCD Student Medical Journal
Written by
John Travers
Edited by
Dr. Helen Gallagher
In fact, findings that highlight how bleeding risks
counterbalance benefits of aspirin use in primary
prevention have been echoed in compelling
results from several other international studies for
several decades. For instance, a randomised trial
of prophylactic daily aspirin in 5,139 British male
doctors with no known CVD between 1978 and 1984
found no clear indication of a decrease in mortality
from CV events.6 A similar, contemporaneous US
study found no reduction in mortality from all CV
causes in 22,071 healthy men treated with aspirin or
placebo in a randomized trial. The study identified
that aspirin helped reduce the risk of MI by 44% but
that moderate-severe and fatal haemorrhagic stroke
risk was more than doubled.7
More recent studies such as the ‘Hypertension
Optimal Treatment’ (HOT) trial further strengthen
the argument against the use of aspirin for primary
prevention. Aspirin use had no significant effect
on cerebral vascular accidents or CV mortality in
trials conducted with 18,790 patients for primary
prevention across 26 countries. 8 While the HOT
study recorded a reduction in MI, it also recorded an
increase in major non-fatal bleeds and minor bleeds.
Furthermore, a 2005 Women’s Health Study with a
randomized trial of 39,876 healthy women treated
with aspirin or placebo failed to show any significant
improvement in the primary prevention of non-fatal
MI, stroke or death from CVD.9
Some guidelines recommend the use of low dose
aspirin in patients with type 1 or 2 diabetes for
primary prevention of CV events. However, the
Prevention of Progression of Arterial Disease and
Diabetes (POPADAD) and the Japanese Primary
Prevention of Atherosclerosis with Aspirin for
Diabetes (JPAD) trials both concluded in 2008 that
there is no evidence to support the use of aspirin
in primary prevention in patients with type 1 or 2
diabetes. In fact, POPADAD found that deaths from
coronary heart disease or stroke among were higher
among aspirin users compared to non-aspirin users
(6.7% v 5.5%).10,11
57
Review Article
# 4
A random sampling study of 88,698 aspirin users in
Taiwan published in 2015 showed that the bleeding
risk of regularly taken low dose aspirin cancelled any
contribution to preventing major vascular disease.
Patients who used low dose aspirin occasionally (less
than 20% of the time) had better health outcomes
than those who used it regularly (more than 80% of
the time).12
A BMJ editorial on the use of aspirin in prevention
of cardiovascular events reported that studies have
consistently failed to demonstrate net benefits for
primary prevention in patients without CVD.13
It cited a review by the US Food and Drug
Administration (FDA) of the proposed labelling of
aspirin for primary prevention, which evaluated five
primary prevention trials, none of which showed net
benefits from aspirin use in primary prevention.1 4
These trials also failed to show a benefit in patients
with diabetes or a Framingham risk score greater than
8-10% over 10 years.
Three key guidelines are as follows:
RELE VANT GUI DE LINE S
There are several UK and European
guidelines that describe aspirin use in patients for
primary prevention of CVD. However, it should be
noted that these guidelines were published between
2005 and 2008, prior to the most recent research,
which highlights the risks of aspirin in primary
prevention.
»»
The Joint British Societies issued guidance
in 2005, recommending aspirin 75mg daily
for people over 50 years with a total CVD 10
year risk above 20%, as well as for people with
diabetes aged over 50 (or younger if they have
had diabetes for more than 10 years or have
been receiving treatment for hypertension),
once blood pressure has been controlled to
150/90 mmHg or less.1 5
»»
All of the literature reviewed points to a consistent
conclusion: any benefits of aspirin use for primary
prevention of CV events are counterbalanced by
potentially fatal bleeding risks.
The Use of Aspirin for Primary Prevention of Cardiovascular
Disease: Review of Literature and Sample Evidence of Common
Practice in Ireland
The Fourth Joint Task Force of the European
Society of Cardiology (ESC) guidelines
recommended in 2007 that patients take aspirin
75mg daily if their 10-year risk of CVD mortality
is over 10% and blood pressure is less than
140/90mmHg.1 6
»»
The National Institute for Health and Clinical
Excellence (NICE) published a guideline in 2008,
recommending aspirin 75mg daily for people
over 50 years with type 2 diabetes if their blood
pressure is below 145/90mmHg.1 7
In the light of the most recent research (specifically
the Drugs and Therapeutics Bulletin research
described above), the Irish College of General
Practitioners confirmed that aspirin should only
be taken on the advice of a GP or healthcare
professional. The National Medicines Information
Centre at St. James’s Hospital, Dublin, outlined that
aspirin mono-therapy is no longer recommended for
certain primary prevention such as atrial fibrillation
related thromboembolic events, due to the risk
of bleeding as well as the observation that the
anti-thrombotic effect of aspirin appears to lessen
with age.1 8 The ESC also updated its guidelines
based on recent research to state that aspirin is not
recommended in individuals with cardiovascular or
cerebrovascular disease due to the increased risk of
major bleeding. It appears that the guidelines are
slowly changing to reflect the evidence on risks of
aspirin use in primary prevention.1 9
S AMPLE E V ID E N C E OF COMMO N US E OF A S P IRIN FOR PRIMA RY P RE V E N TION
An audit was conducted at the Dun
Laoghaire Surgery, Co. Dublin, as part of this review
to identify patients who were taking aspirin for
primary prevention that did not meet any of the
above guidelines.
All patients at the practice that had been taking
aspirin (75mg daily) in the 24 months prior to July
1, 2013, were identified by a medications search of
electronic records. This amounted to 385 patients. 19
of these had either passed away or left the practice
in the interim. The histories of each of the remaining
366 patients were reviewed. All those who had
experienced a MI, CVA or TIA and therefore were
being managed for secondary prevention were
excluded. Furthermore, patients with a high CVD or
high CV event risk – for instance, those diagnosed
with peripheral vascular disease, had demonstrable
CV symptoms such as unstable angina or intermittent
claudication or who had stents or prosthetic valves in
place – were also excluded.
70 patients that had not experienced a CV event
and did not fall into the CVD high risk category
described above were taking aspirin for primary
prevention. These patients had conditions such as
controlled hypertension, ‘once-off’ chest pain or
had a family history of CV events. These patients
amounted to 19% of all current patients taking aspirin
for secondary or primary prevention. The 70 patients
ranged in age from 35 to 91 years. The median age
was 74.5 years, while the average age was 72.4 years.
58
UCD Student Medical Journal
Written by
John Travers
Edited by
Dr. Helen Gallagher
→
Number of patients
prescribed aspirin
(75mg daily) in the
period July 1 2011
- July 1 2013
8 11
296
70
Dun Laoghaire
Surgery
*Patient had
emigrated or left
the practice,
**Secondary =
following MI, CVA
or TIA.
High Risk = patient
with peripheral
vascular disease,
unstable angina,
stents in situ,
heart valve
impairment or CVD
mortality risk over
10 years >10%.
Review Article
# 4
The Use of Aspirin for Primary Prevention of Cardiovascular
Disease: Review of Literature and Sample Evidence of Common
Practice in Ireland
BROADENING How might we broaden preventative medicine
in Irish GP practices to address CVD risk factors?
PRE VE NTATI VE ME DICINE
Interestingly, financial incentives do not appear
FOR CVD MANAGE MENT
Figure 1
Source
59
RECORDS
DISCONTINUED*
RIP
SECONDARY
PREVENTION
OR
HIGH RISK**
PRIMARY
PREVENTION
TOTAL 385
An audit conducted in the Broadline Family Practice,
Blackpool, Cork, in 2011 and 2012 and published
in 2013 found results comparable with the Dun
Laoghaire audit. 333 patients were identified to be
taking aspirin and 62 patients (18.6%) were taking
aspirin for primary prevention. Their average age
was 64.9 years. It was further determined that 10 of
these 62 (16.1%) were at a low risk of cardiovascular
disease by calculating their 10-year QRISK2 score.20
Both of these audits indicate that patients in Ireland
are often prescribed low dose aspirin for primary
prevention of CV events, despite clear and consistent
research results showing no net benefit to patients
and the introduction of potentially fatal bleeding risk.
Inappropriate use of aspirin for primary prevention
does not appear to be an issue unique to Ireland.
A study published in 2015 reviewed aspirin use by
68,808 patients in 119 practices across the US and
determined that 11.6% of these patients were using
aspirin “inappropriately”. The patients had no CVD
and their 10-year CVD risk was low. Their use of
aspirin introduced risks of gastrointestinal bleeding
and haemorrhagic stroke that outweighed benefits in
primary prevention.21
Prevention of CVD, and all chronic
conditions, is a priority for general practice.
However, GPs continually make a trade-off between
time consuming pro-active preventative medicine
and the immediate demands of reacting to acute
health conditions. It is estimated that a typical GP
would need 7-8 hours to implement best practice
preventative medicine each day, precious time
that GPs do not have.2 2 It is possible therefore
that offering aspirin as a preventative measure for
CVD may sometimes be seen as an alternative to
a more time-consuming assessment of risk factors
and investment in education and counselling. For
instance, primary care physicians in the US and
Australia discuss alcohol consumption with less than
a fifth of patients, smoking with two-thirds, exercise
with a third and diet with 15-30% - all key modifiable
risk factors for CVD.2 3 , 2 4 Although these interactions
may take time, the US Preventative Services Task
Force identified such risk factor discussions as among
the most valuable preventative services to patients in
reducing mortality and overall healthcare costs.2 5
The November 2014 conference of the Irish National
Institute for Preventive Cardiology (NIPC) highlighted
how 50% of over 50s are overweight or obese, 3050% have elevated blood pressure, 34% have low
rates of exercise, 20% smoke and 16% report alcohol
problems.v2 6 Speakers at the NIPC conference
also outlined how CVD was the single largest cause
of death in Ireland and that more than 50% of
reductions in CVD relate to risk factor changes.2 7 It
would appear there is much room for improvement
in reducing risk factors for CV events that can make a
major difference to the health of patients.
to help. Only one out of eight financial incentive
programmes implemented between 1966 and 2002
in English speaking countries motivated doctors to
provide more preventative care.28
The answer may lie instead in introducing planned
health checks for all patients over the age of 45.
A randomised controlled trial of 1,507 Danish
patients showed that the number of patients at
elevated cardiovascular risk was halved as a result of
biannual health screenings in family practices over
five years.2 9 The approach is similar to the ‘Managed
Care’ philosophy implemented by Kaiser Healthcare
in the US, which offers five annual planned health
checks to patients over 65, reducing the incidence of
acute care emergencies, decreasing the days spent in
a hospital bed and improving overall outcomes.
Health check activities could be shared between
practice nurses and doctors to help manage limited
time resources. This form of preventative medicine
where patients and healthcare professionals actively
collaborate on managing smoking, alcohol, diet and
exercise would lead to improved health outcomes,
lower healthcare costs and help avoid unnecessary
prescription of aspirin and consequent bleeding risks
in primary prevention.
60
UCD Student Medical Journal
CO N CLU S I O N
Written by
John Travers
Edited by
Dr. Helen Gallagher
Evidence in the literature points to
significant risks of bleeding associated with aspirin
use that counterbalance benefits in primary
prevention of CV events. Despite this, fact-based
audits highlight that use of aspirin for primary
prevention of CVD and CV events is common. The fact
that UK and European guidelines do not reflect the
most recent research on the issue may contribute to
this. This paper offers three suggestions to address
the issues of aspirin use in primary prevention in
light of the above findings. Firstly, doctors should
engage with patients who take aspirin for primary
prevention to review the full benefits and risks.
Secondly, it is worthwhile for doctors and patients to
invest time in identifying and managing modifiable
risk factors for CVD and conduct regular, planned
health checks. Lastly, relevant guidelines should be
updated to reflect recent research on the bleeding
risks of using aspirin in the prevention of CVD and CV
events. These findings and suggested actions could
be communicated effectively through the medium
of the National Institute for Preventative Cardiology
Alliance, which brings together healthcare providers,
institutions and industry in preventive action. Putting
these suggestions into practice would improve overall
healthcare and patient outcomes.
61
Review Article
# 4
Acknowledgements
Thanks to Dr. Nicola Boyle, Dr.
Paul Lacey and Dr. Ray Murphy of
the Dun Laoghaire Surgery for inviting me to participate in their
audit and for their mentorship.
References
01 Pignone M, Williams C. Aspirin for
primary prevention of cardiovascular disease in diabetes mellitus. Nat Rev Endocrinol. 2010;
6(11):619-28.
02 Rang H, Dale M, Ritter J, Moore P.
Pharmacology. 5th edition. London:
Elsevier Churchill Livingstone; 2003.
03 Antithrombotic Trialists’ Collaboration. Collaborative meta-analysis of randomised trials of antiplatelet therapy for prevention of
death, myocardial infarction and
stroke in high risk patients. BMJ.
2002; 324(7330):141.
04 Antithrombotic Trialists’ Collaboration. Aspirin in the primary and
secondary prevention of vascular
disease: collaborative meta-analysis of individual participant data
from randomized trials. Lancet.
2009; 373(9678):1849-60.
05 Aspirin for primary prevention of
cardiovascular disease? Drug Ther
Bull. 2009; 47:122-5.
06 Peto R, Gray R, Collins R, Wheatley K, Hennekens C, Jamrozik K,
Warlow C, Hafner B, Thompson E,
Norton S, Gilliland J, Doll R.
Randomised trial of prophylactic
daily aspirin in British male doctors. BMJ. 1988; 296 (6618):313-16.
07 Final report on the aspirin component of the ongoing Physicians’
Health Study. Steering committee
of the Physicians’ Health Study
research group. N Eng J Med. 1989;
321(3):129-35.
08 Hansson L, Zanchetti A, Carruthers
G, Dahlof B, Elmfeldt D, Julius S,
Menard J, Heinz Rahn K, Wedel H,
Westerling S. Effects of intensive blood pressure lowering and
low dose aspirin in patients with
hypertension: principal results of
the Hypertension Optimal Treatment
(HOT) randomized trial. Lancet.
1998; 351(9118):1755-62.
09 Ridker P, Cook N, Lee I, Gorden
D, Gaziano J, Manzon J, Hennekens
C, Buring J. A randomized trial of
low dose aspirin in the primary
prevention of cardiovascular disease in women. N Eng J Med. 2005;
352(13):1293-304.
10 Belch J, MacCuish A, Campbell I,
Cobbe S, Taylor R, Prescott R, Lee
R, Bancroft J, MacEwan S, Shepherd
J, Macfarlane P, Morris A, Jung
R, Kelly C, Connacher A, Peden N,
Jamieson A, Matthews D, Leese G,
McKnight J, O’Brien I, Semple C,
Petrie J, Gordon D, Pringle S,
MacWalter R. The prevention of
progression of arterial disease
and diabetes (POPADAD) trial:
factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes
and asymptomatic peripheral arterial disease. BMJ. 2008; 337:a1840.
The Use of Aspirin for Primary Prevention of Cardiovascular
Disease: Review of Literature and Sample Evidence of Common
Practice in Ireland
11 Ogawa H, Nakayama M, Morimoto T,
Uemura S, Kanauchi M, Doi N, Jinnouchi H, Sugiyama S, Saito Y,
Japanese primary prevention of
atherosclerosis with aspirin for
diabetes (JPAD) trial investigators. Low-dose aspirin for primary
prevention of atherosclerotic
events in patients with type 2
diabetes: a randomized controlled
trial. JAMA. 2008; 300:2134-41.
12 Wu I, Hsieh H, Wu M. A short-term
risk–benefit analysis of occasional and regular use of low-dose
aspirin in primary prevention of
vascular diseases: a nationwide
population-based study. BMJ Open
[Internet]. 2015 Jan;5:e006694.
Available from: http://bmjopen.
bmj.com/content/5/1/e006694.full
13 Editor. Aspirin for prevention of
cardiovascular events. BMJ. 2008;
337:a1806.
14 Fleming T, Nissan S, Borer J,
Armstrong P. Report from the 100th
cardiovascular and renal drugs
advisory committee: US Food and
Drugs Administration. Circulation.
2004; 109:e9004-5.
15 JBS 2: British Cardiac Society,
British Hypertension Society, Diabetes UK, Heart UK, Primary care
cardiovascular society, The Stroke
Association. Joint British Societies’ guidelines on prevention of
cardiovascular disease in clinical
practice. Heart. 2005; 91:v1-52.
16 Fourth Joint Taskforce of the
European Society of Cardiology and
other societies on cardiovascular
disease prevention in clinical
practice. European guidelines on
cardiovascular disease prevention in clinical practice. Eur
J Cardiovasc Prev Rehab. 2007;
14(suppl2):S1-113.
17 The National Collaborating Centre
for Chronic Conditions. Type 2
diabetes: National clinical guideline for management in primary and
secondary care (update). London:
NICE, 2008.
18 National Medicines Information
Centre. Update on management of
non-valvular atrial fibrillation,
volume 19, number 1. Dublin: St.
James’s Hospital, 2013.
19 Perk J, De Backer G, Gohlke H,
Graham I, Reiner Z, Verschuren
M, Albus S, Benlian P, Boysen
G, Cifkova R, Deaton C, Ebrahim
S, Fisher M, Germano G, Hobbs R,
Hoes A, Karadeniz S, Mezzani A,
Prescott E, Ryden L, Scherer M,
Syvanne M, Scholte op Reimer W,
Vrints C, Wood D, Zamorano J, Zannad F. European guidelines on cardiovascular disease prevention in
clinical practice. The fifth joint
taskforce of the European Society
of Cardiology and other societies
on cardiovascular disease prevention in clinical practice. Eur
Heart J. 2012; 33:1635-1701.
20 Hallihan P, Horgan T, English T.
Who should and shouldn’t be on
aspirin? ICGP Forum. 2013; Nov:44-45.
21 Hira R, Kennedy K, Nambi V, Jneid
H, Alam M, Basra S, Ho M, Deswal
A, Ballantyne C, Petersen L, Virani S. Frequency and practice-level
variation in inappropriate aspirin
use for the primary prevention of
cardiovascular disease. J Am Coll
Cardiol. 2015; 65(2):111-121.
22 Russell G. Is prevention unbalancing general practice? Med J Aust.
2005; 183(2):104-105.
23 Stange K, Flocke S, Goodwin M,
Kelly R, Zyzanski S. Direct observation of rates of preventive service delivery by community family
practice. Prev Med. 2000; 31:167-76.
24 National Preventative Health Taskforce. The role of primary health
care in preventing the onset of
chronic disease, with a particular focus on the lifestyle risk
factors of obesity, tobacco and
alcohol. Sydney: UNSW Centre for
Primary Health Care and Equity, 2008.
25 Maciosek M, Coffield A, Edwards N,
Flottemesch T, Goodman M, Solberg
L. Priorities among effective
clinical preventive services:
results of a systematic review and
analysis. Am J Prev Med. 2006;
31(1):52-61.
26 Smyth B. The challenges for prevention in Ireland. In: Pushing
the boundaries in cardiovascular
disease prevention; 2014 November
29; Galway, Ireland. Dublin: NIPC;
2014.
27 Graham I. Enhancing CVD prevention in Ireland. In: Pushing the
boundaries in cardiovascular
disease prevention conference;
2014 November 29; Galway, Ireland.
Dublin: NIPC; 2014.
28 Town R, Kane R, Johnson P, Butler
M. Economic incentives and physicians’ delivery of preventive
care: a systematic review. Am J
Prev Med. 2005; 28:234-240.
29 Engberg M, Christensen B, Karlsmose B, Lous J, Lauritzen T. General health screenings to improve
cardiovascular risk profiles:
a randomized controlled trial
in general practice with 5-year
follow-up. J Fam Pract. 2002;
51(6):546-52.
62
UCD Student Medical Journal
A
Day
in the
Life…
of
an Intern
in Ireland
Written by
Maeve Montague
Featuring
Dr. Ken Fitzpatrick
63
Healthcare Perspectives
# 1
A Day in the Life... of an Intern in Ireland
64
UCD Student Medical Journal
Written by
Maeve Montague
Featuring
Dr. Ken Fitzpatrick
You made it through the Leaving Cert, the years spent
in the lecture theatres of the Health Sciences Building on
college campus, and then it is time to don the white coat as
the clinical years begin. But what happens next? The life of a
medical intern can be hard to understand past the headlines
dominating the media - long hours, fatigue, a fluctuating payscale – so what is the reality?
According to Dr. Ken Fitzpatrick, “It’s not so bad. You’ll enjoy it – really”. A current surgical intern at St.
Vincent’s University Hospital, the experience is not how Ken initially expected. “During your clinical years you
don’t really have the chance to see the interns at work, so when you start it can seem like you’re in at the deepend at first. But I can honestly say I learned more in my first month working, than the entire previous four years of
graduate medical school”.
After applying competitively for schemes following graduation, interns in Ireland find themselves
across the country, becoming the newest team member, and the one responsible for managing the patient list.
A list of all those in the care of your team, it is “the most important thing for an intern. It can change drastically,
whether your team was on-call the night before or not”. This list keeps the team focused on their patients, and is
the source of all information – from what tests and imaging have been taken, to those that are still outstanding
- and what is next in the treatment plan. With 7am morning rounds led by the Specialist Registrar, it is the
intern who makes a list of jobs that needs to be carried out for each patient before evening rounds. And with
20-40 patients to be seen within 30-60 minutes, focus and attention are imperative. On how to manage these
jobs, while balancing other duties, such as admitting new patients, Ken stresses the need for organisation and
teamwork skills. “There are usually at least two interns on any team, so it’s useful to meet up after rounds and split
the workload to avoid double jobbing”.
In times of a greater workload, epitomised by the sounds of a never-ending bleeper, it is the
supportive network of the team that allows interns to work without feeling too overwhelmed. “There can be a
feeling of guilt when you call someone, but it’s specified that no-one minds. The Senior House Officers (SHOs)
are really approachable, and while there is a chain-of-command, in that Registrars prefer to be called by SHOs
who are called by you (the intern), patient safety is what ultimately matters – that’s the rule”.
“PATIENT SAFETY IS WHAT
ULTIMATELY MATTERS –
THAT’S THE RULE”
65
Healthcare Perspectives
# 1
A Day in the Life... of an Intern in Ireland
With the recent ‘24 No More’ campaign, and regular media coverage of doctors' working hours, it
might not be a surprise to learn that it is the on-call shift which most worries new interns. “The first couple of
shifts were pretty terrifying – I was definitely nervous. You have this idea in your head that you’re not going to be
able to deal with, what could be, a vast number of problems. But the assessments are all the same at the end of
the day, so as long as you get the wheels in motion you’re keeping up with the team’s expectations”.
For surgical interns on-call, it is the medical Registrar on-call who becomes their saviour. Unlike surgical
Registrars, who can go home if not needed in theatre, the medical Registrar stays in the hospital and is often at
the other end of the phone, willing to give advice. “You definitely feel like a student at first. Being on-call teaches
you that you need to get things done. When you no longer have an SHO to turn to, you realize that you have to
keep trying. This makes you learn fast and, while it might seem a lot of pressure at first, it stands to you in the
long run. By the second or third on-call shift the worry fades – physical exams and taking a history followed by
collecting bloods and taking cultures become part of the motion”.
During a night shift interns are ruled by ‘sweeps and bleeps’. Sweeps - a list of non-urgent jobs put up
by the nurses on each ward – can range from rewriting drug card indexes to placing cannulas; while bleeps are
usually a call to assess a patient. Interns prioritize these duties, and while a 24-hour shift can be hard to adjust to
“it can be fun – there’s usually a great camaraderie between the two interns on-call. There’s a chance for some
down-time and to order-in food - generally the work load is divided to allow each intern to take 2-3 hours of
sleep at a time”.
With interns starting at 6:45am, mornings need to quickly be adjusted to – there are, however, a few
silver linings. “There’s very little traffic at 6am, and always plenty of parking”. Another matter is breakfast - which
really does become the most important meal of the day - as being busy, while good for time passing by, can
often lead to missed meals. “You never know when you’re going to be bleeped, so be prepared to take any
opportunity you have to grab something”.
Formal teaching continues throughout the year, with two lunchtime meetings per week, via the Dublin
Academic Medical Centre (DAMC) Intern Training Program. As well as teaching, this also offers interns the
opportunity to present interesting cases, and network with other interns across different schemes. Within the
surgical team, there are further opportunities to learn more after morning ward rounds during the week – from a
radiology meeting on Tuesday, to a Journal Club across general surgery on a Wednesday, or a research meeting
on Thursday.
Though much of current media has focused on the rising emigration of Irish doctors, Ken is more
hopeful on the subject. “Irish doctors have always emigrated. I think a lot of graduates want the experience
of working in a different country, but most intend to return with new skills”. He also feels that the issue of the
European Working Time Directive is being tackled within hospitals, but wider changes have to be implemented
before progress becomes apparent.
When asked what medical students should be doing now to help pave the way for the intern year,
Ken’s advice is clear: “Put yourself forward. Talk to as many patients as possible, practice taking histories, and
performing physical exams when you get the chance. Don’t hold back - everything that’s good for you as a
student is nerve-wracking!”
66
UCD Student Medical Journal
The
Long
Game
Interview
with
Dr. Rhona
Mahony
Written by
Neasa Conneally
Sarah Murphy
67
Healthcare Perspectives
# 2
The Long Game... Interview with Dr Rhona Mahony
68
UCD Student Medical Journal
Written by
Neasa Conneally
Sarah Murphy
Dr. Rhona Mahony; Consultant Obstetrician and the first
female Master of the National Maternity Hospital, on her career,
memories of her time in UCD and being a prominent voice and
advocate for better maternal and infant care in Ireland.
→ Is there such thing as a
typical day for you?
No, that’s the beauty of it. I am usually
in the hospital by 7AM to get a feel of
how things have been overnight. At 7.30
we have a handover meeting so all our
NCHDs (non-consultant hospital doctors)
meet, we look at what happened the
night before and we try to identify the
patients that we’re worried about and
make sure that we have identify women
with potential problems so that that
nobody gets dropped on the handover.
We also use it as an opportunity to
debrief a little bit; sometimes it can be
traumatic for young staff who might have
had a very difficult delivery. We’re very
into learning from everything; we’re not
into blaming or into pointing the finger.
We might say, “Look, we might have done
that a bit better” but in a very positive
way.
At 8AM, I have to have my slice of toast
and my cup of tea. I always say there’s
no point asking me for something until
I am fed because invariably it will be a
negative answer!
After that it varies, so on a Thursday I
might be scanning all day, on Wednesday
I might have be operating in theatre,
but very often I have a lot of business
meetings as well, we are carrying out
lots of renovations around the hospital
just to keep it safe for the next few
years while we progress with our major
redevelopment plan, moving to the St
Vincent’s University Hospital campus.
→ How do you find balancing
your clinical practise with
your duties as Master?
Lots of hours, I have to say, but I love
clinical practice. People say to you “As
Master, perhaps you shouldn’t do any
clinical practice, you should just be the
CEO”, but in terms of motivating myself
and inspiring myself - seeing babies
being born keeps me sane and keeps
me connected. On a very important
level it also keeps me very connected to
the hospital so I’m not seen to be some
distant figure issuing instructions. People
see me at four in the morning, up to my
tonsils in trouble, like everyone else! I
also take part in the call rota, I think that
does help when you’re trying to bring
change with you, that people feel that
you’re part of the team and they will
come with you.
69
Healthcare Perspectives
# 2
→ Do you think being
a woman makes any
difference to how you carry
out your role?
Not at all. People say “The first female
Master!” well, I’m the first female that
applied to the job here so that takes care
of that!
→ What do you need to be
Master?
You need to be a good obstetrician. You
need a good insight into complex foetalmaternal medicine problems because
we might have very difficult decisions to
make for patients and its really helpful
having a clinical background like I have
because it helps me understand, when it
comes to complex decisions, what are the
pitfalls, what are the difficulties and what
might the outcomes be. On a strategic
level, I think of my own daughters
growing up and wonder how maternity
and gynaecological services will be for
that generation. I like to think they will
be better. I think I’m very driven by that
overall picture of how should it be and
could be for women in Ireland
→ You really came to
prominence in the public
eye when you spoke at the
Oireachtas hearings for the
Protection of Life During
Pregnancy Bill, was being an
advocate for women in that
role something you felt very
strongly about?
I felt very much that a medical opinion
should be given during the hearings
because they addressed the very
restrictive domain of risk to life for
women and I am aware from my practice
that at times there are complications
of pregnancy that can result in women
dying. They’re rare, they’re very
infrequent, but they are there.
The Long Game... Interview with Dr Rhona Mahony
So I felt that if there was to be a
discussion, that doctors should take part
in that and give their medical experience
over many years because the issue of
maternal mortality very much belongs in
our sphere and it was very important that
any myths might be dispelled.
I didn’t appreciate the level of attention
that it would bring upon me and I
suppose I found that quite difficult
because I wasn’t prepared for it. It’s
not that I didn’t think there’d be some
attention given but it was a little more
than I had anticipated.
So it was a very interesting time. Would I
do it again? Yes, I think it was my duty and
I think I gave my honest medical opinion
based on my factual experience and I
think that was the right thing to do.
→ Recent events have
shown that perhaps there is
still some uncertainty over
what the legislation actually
means, would you agree
with that?
I think that the law changes nothing
really; it essentially legislates for the X
Case. I think a lot of people thought the
law was introduced in response to the
Savita Halappanavar case but not at all, it
was actually in response to the A, B and C
v Ireland cases in the European Court.
The Supreme Court interpreted the
Constitution in the X Case to permit
termination of pregnancy if there was a
substantial risk to a mother’s life caused
by complications of pregnancy – a
risk which could only be removed by
terminating the pregnancy. However,
there was no clear process whereby a
woman could determine if she qualified
termination of pregnancy on the grounds
of risk to her life. So the European Court
charged Ireland with providing women
with such a process.
I think that a lot of people thought
that the law was going to somehow
revolutionise things, it never set out to
do that and so it caused disappointment
on both sides, because for the people
that get labelled "pro-life", and I hate
labels, they felt that it went too far and for
the group that might get labelled "prochoice", they felt that perhaps it didn’t go
far enough but the law was never going
to do anything different. Some people
were unhappy that it did not deal with
other aspects of complex pregnancy
including rape and fatal fetal abnormality.
These remain uncomfortable topics, not
least for women affected, and I think the
discussions and debates are far from
over.
I also don’t think that any law will take
away the complexity of life. The law is
there to protect as much as possible,
but humans are very complex, life is very
complex, and reproduction has got to be
one of the most complex aspects of life
- glorious and fantastic, but fraught with
all kinds of physical, ethical and moral
challenges.
70
UCD Student Medical Journal
→ On the topic of fatal
foetal abnormalities, do you
personally feel the need for
it to be legislated for and
further laws to deal with
the lacunas in these sorts of
cases?
I think it’s really hard. It’s interesting
because this is my area of practice and
my experience is that some women with
a fatal foetal abnormality will know this
and carry their baby to term and their
baby may only live for 5 minutes, 10
minutes, but those 10 minutes are the
most precious moments of their life and
they would never give that back. It is
so important we acknowledge that and
we give all the support we can to these
women and their families to navigate that
very tragic circumstance.
Some women, on the other hand, will find
the idea of going through that pregnancy
and delivering just absolutely impossible,
so everyone is different and the question
is how do we within our society cater for
people with different opinions? I think
that’s where Ireland really struggles, we
like everything to be black and white and
we like everyone to think the same way,
but people don’t think the same way,
and we have got to realise that people
will approach things differently and what
really matters is that we take really great
care of our women and our babies.
Written by
→ When talking about
increasing staffing levels,
how would you improve
the retention of medical
graduates in Ireland?
There are a number of interesting things
happening in Health at the moment. One
is that we have lost some of our senior
consultants because of induced voluntary
retirement schemes. Approximately 7080% of a budget in any hospital is spent
on staff; if you want to save money the
big economical thing is to reduce staff.
But that can have devastating
consequences. So we lost a lot of our
most senior doctors and midwives;
that was the first thing. The moratorium
on staffing levels was a very blunt
tool and resulted in gaps, which were
subsequently filled by agency staff
at great financial expense and at the
expense of local departments stability
and progress.
Then we find that we have graduates
coming out of medical school who are
some of the best trained in the world
but 50% of them are not taking Irish
registration. Some of that will be because
they were never going to, they came
from abroad and now are going back.
But some of that is because they don’t
see a future in Ireland. And when that
starts to happen you have really got to
wake up and smell the coffee, both as
professionals and as a country.
So you have to ask Why? What could it
be about working in Ireland that would
put young people like you off? First thing
is Ireland has got to start by providing
the best teaching and training. It won’t
do that unless it increases the number of
Consultants. Training requires supervision
and there is no point in running, as we
do, our health service with lots of people
in training and only a few people at the
top. I think if people know that they
would get the very best training then they
would consider staying.
Neasa Conneally
Sarah Murphy
We have to address the long hours in
some specialties, particularly obstetrics
and surgery; you have to address those
things so that people can still have a life. I
wouldn’t like people coming up through
the system that I came up; where we
worked over 100 hours a week and I have
done so pretty much ever since I was
23. I don’t think that that’s a sensible or
necessary approach.
Pay is also an issue. We’ve got to take a
whole new view of "How do we attract
these brilliant new doctors", and not
"These doctors are lucky to get a job in
Ireland", which is where I think we have
been. We have a reputation for being
toxic employers, which we do deserve
and we must now start to come away
from that and start making big changes.
→ How do you balance
your long working days with
having a young family?
Very badly! Honestly, I’m really lucky; I
have a huge amount of support from my
husband. He hates me mentioning him
but he is extraordinary in his ability to
multitask and look after the children and
do everything. He’s a total rock - he just
keeps the whole house running and he
works himself, I don’t know how he does
it.
I do give up a lot and others give up a lot
on my behalf. I’m aware that I’d love to
spend more time with the children. I have
missed loads of things and that’s a very
difficult thing about being an obstetrician,
that your job absolutely comes first, you
can’t let people down, you can’t just not
go on call, so you have to be there all the
time and it does require certain sacrifices
to be made. I think it’s worth it in the
long run but it is really difficult at times.
I always say to my kids, “I’m not always
here all of the time but I’m loving you all
of the time”.
71
Healthcare Perspectives
# 2
→ As a woman in a high
leadership role, how would
you suggest that the medical
profession works with
women to allow them to
progress in their careers but
also have families?
I think it comes back to part of providing
training and flexibility. So many young
doctors who are coming through now are
female and that‘s fantastic, but there are
going to be differences. People always
say you’re being politically incorrect but
actually it’s a fact and it means we might
have to plan our work force a little bit
differently and we might need to add in
a buffer so that maternity leaves can be
taken care of.
If you can support women through
having their young children, then women
will continue to work bringing all their
skill and experience to the work place..
So you must always take a long view, but I
think with the number of women coming
though we will have to change how our
work force planning is.
→ Speaking of having a life,
what is it you like to do when
you’re not working?
When I have a life! I joke that if I wrote a
biography recently, it would be “I went to
work and then I slept”, that’s it. It would
be a short book!
No, I’m very interested in life outside
of medicine; in fact one of the best
things about being Master has been
my exposure to all kinds of different
organisations, and to things outside of
medicine.
The Long Game... Interview with Dr Rhona Mahony
But off-duty, I go running because you
can do that at any time, you just take a
pair of runners and off you go. I love to
run around Howth Hill because it’s so
beautiful all the time. I like to read, I love
theatre. I’m a geek; I love anything that
will elevate me. I love eating and the
odd glass of wine, if I’m honest. So I love
Sunday dinner when everyone’s around
the table, my mum and dad, all the family,
everyone is talking at each other and no
one is listening, that’s really what I love.
I’m a very simple girl!
→ What was your fondest
memory of your time in
UCD?
Pre-med was just the best year of my life.
I met such lovely people and it was so
exciting. I loved the intellectual freedom
in university, you were surrounded by
really clever people, and yet it wasn’t like
school. You had a bit of time and when
you go out on Tuesday evening, you can
catch up on Wednesday so you had a bit
more autonomy in how you ran your life.
It was very exciting to go into the
hospitals as well and be part of that,
but I think it was definitely pre-med and
that whole feeling of being set free and
intellectual stimulation. It was just so
much fun but I nearly failed my pre-med
exams, I have to say!
→ If you had one piece of
advice for a medical student
today, what would it be?
It’s a long game. A career in medicine is
going to take a lot of courage, it’s going
to take a lot of tenacity and it’s going to
take a lot of resilience. So you’ve always
got to take the long view all of the time
and don’t let the short term knock you.
Always be fixed on your longer goal.
And the other bit of advice to everyone
is really mind each other, because you
are the next generation of doctors. You’re
really important and your contribution
is going to be enormously important
because you shape the next generation
coming behind you. So if you have
a collaborative way of working, you
can achieve so much more by being
synergistic. Avoid the petty politics; keep
out of it because the kinds of people who
love office politics don’t get things done.
Getting involved in bitching is a waste of
time, it doesn’t get you anywhere. Always
look, the whole time, at what you are
trying to achieve because getting things
done is very exciting.
Want to read more?
Go to www.ucdsmj.com
72
UCD Student Medical Journal
Top 10
Apps
for
Health Care
Students
Written by
Sarah Murphy
Nora Tadros
73
Feature Article
# 1
Top 10 Apps for Healthcare Students
74
UCD Student Medical Journal
Written by
Sarah Murphy
Nora Tadros
75
Feature Article
# 1
Top 10 Apps for Health Care Students
1 . D RO P B OX
Dropbox is extraordinarily simple, but its usefulness can not be overstated. It is an online storage space that
provides multitudes of students the relief of knowing their files are always safe. It can be used as a backup
for all of your lectures, assignments, and any other important documents, academic or not! If any disastrous
circumstances strike, whether it involves a crashed or missing laptop, or an accidental delete, all of your
documents are completely safe and you can redownload them at any point! Any documents that you choose to
upload are well protected and are shown to others only if you allow them to be. Another extremely useful feature
is the ability to share documents so others are able to access this information as well. This makes it extremely
useful for group projects or any situation where multiple people need access to one source of information.
Famed as the "Instagram for Medical Professionals", Figure 1 will allow you to share, rank and discuss medical
images from around the world. Similar to Instagram, by using a description or hashtag you can search for images
and if no such image exists, you will be redirected to a different search engine, such as Google. Figure 1 allows
you to discuss diagnosis and treatment with other experienced peers, to broaden your knowledge by viewing
both rare and textbook cases and give you the opportunity to familiarise yourself with x-rays, charts, MRI and
CAT scans. Whether you want to learn or want to mindlessly scroll through another social networking app (with a
twist), this is an invaluable app to get!
2 . B LACK BOA RD
An absolute must for almost any college course in UCD! The Blackboard app allows you to access any
information about your modules while you’re on the go, including lectures, and announcements. Additionally,
you can allow Blackboard to send you notifications to update you when any lectures, announcements, or other
material has been uploaded. This app is fundamental for easily staying up to speed with your academic modules
at all times!
3 . N E W E NG LA ND JO UR NA L O F MEDICINE, T H IS WEEK
This app from New England Journal of Medicine (NEJM) allows medical students to easily keep up to date with
recent NEJM articles. It includes articles on medical research, and review articles on topics important to clinical
practice as well as biomedical science. It also has an images, audio, and video section which serve to educate
students on important medical conditions and procedures. The NEJM also has a couple other apps, such as the
NEJM Image Challenge App, which are dedicated solely to education on medical conditions, as well as allowing
the student to test their knowledge.
4. EPONYMS
Not just a medical dictionary, Eponyms also contains definitions of procedures, syndromes, signs, anatomical
locations and everything under the sun associated with medicine. This app is immensely handy if there is a
term you come across in a lecture or assignment that you have not seen before. The explanations are clear and
concise so it’s just like having wikipedia in your pocket. An important feature of this app is that this knowledge
base can be accessed anywhere at all because no access to the internet is needed!
5 . D I AG NO ST I C RADIO LO GY
A must for anyone trying to understand and visualise radiology. This app includes clear pictures of different
anatomical regions and organs from multiple different planes. You are also able to zoom through the images to
see different perspectives of the region. All the images are exceptionally well labelled so you actually know for
sure what you are looking at! There are actually a few different versions of this app with most of them being free
and one paid.
6 . FIGURE 1
7 . FACE BOOK
So universal it is often over-looked, the Facebook app allows you to keep up to date on social events and course
groups. Additionally, it keeps you in the loop for group projects and every academic resource shared by your
peers. Although a small amount of willpower is needed to close the app during lectures, it more than makes up
for it’s potential distraction by allowing students to stay in both the social and academic loop effortlessly.
8 . ME DS CAPE
For anyone who is already familiar with the desktop version of Medscape, there is no doubt you can appreciate
all it has to offer. Incredibly the mobile app has even more features. Firstly a drug reference for current
prescribing, dosing and even pregnancy guidelines, furthermore it offers over 120 medical calculators for
anyone who struggle to remember any of those pesky calculations. There are also disease and condition
references, complete with presentation, work-up and treatment. Finally, their news section will keep you totally
up to date with the latest articles written by a team of experts in a range of specialties.
9 . FI RST AI D BY I RIS H RE D CROS S
Simple and free. This app is perfect for any health care professional, or anyone period. It will provide one with
instant access to information that will enable one to handle common first aid emergencies, as well allow one to
ring 112 directly from the app itself. The app is complete with videos, step-by-step advice and quizzes, which
make it very easy to to know first aid. One of the best things about this app, is that all content is preloaded,
which means you can access all information even if you don’t have reception or internet connection. This app is a
definite must.
1 0 . RE AD BY QXMD
An app that allows you to bring medical journals and literature together in a magazine format. It also enables
you to download studies, journals and articles from a variety of sources, including Pubmed, so you can reference
them at any time, even on the go. This will ensure you are kept up to date in all specialties and will allow you to
reference when writing reviews or even studying.
76
UCD Student Medical Journal
UCD
Student
Summer
Research
Awards
Programme
2014:
Three
Experiences
Written by
Cathal Ahern
Peter Fryc
Caroline Moran
77
Feature Article
# 2
Student Summer Research Awards Programme 2014:
Three Experiences
78
UCD Student Medical Journal
Written by
U CD ST U DE NT S U MMER RE S E A RCH AWA RDS ( SSR A ) P RO G RA M M E 2 0 14:
T H RE E P E RS P E CT I V ES
The SSRA provides students with the
unique opportunity to experience lab-based, clinical,
patient advocate or educational research during the
summer, aiming to promote a greater appreciation
of the critical role which research plays in modern
medicine, and encouraging students to develop a
life-long passion for discovery. Three students discuss
their experience of the SSRA.
1 . CAT H A L A H E RN , STAG E 4 U NDE RG R A DUAT E M E DI CI NE A ND S SR A
F I NA L I ST 2 0 1 4
Project Title
A novel mind-map-slideshow hybrid for the
standardised, interactive and graphical presentation
of pathology topics.
Supervisors
Dr Peter Holloway, Mr Adam Tattersall
Location
Teaching and Learning Education Group, School of
Medicine and Medical Science, UCD
“Power corrupts. PowerPoint corrupts
absolutely.” – Edward Tufte
The summer of 2014 brought with it the pleasure
of working with Dr Peter Holloway, Special Lecturer
and Educationalist at UCD SMMS, on an SSRA
project. Our work concerned the development and
evaluation of a new presentation platform, inspired
by perceived problems with the use of presentation
software (e.g. PowerPoint) in education.
Cathal Ahern
Peter Fryc
Caroline Moran
PowerPoint is widely criticised in educational and
psychological literature1, 2, 3 for having little
grounding in the theories and science of learning.
Edward Tufte, a pioneer in the field of information
design, leads the charge against PowerPoint. His
book ‘The Cognitive Style of PowerPoint’1 , argues
that PowerPoint’s linearity and rigid structure - the
way it progresses as a series of equal-sized boxes forces simplification of complex content.
PowerPoint also suffers, says Tufte, from a narrow
visual bandwidth - the way in which the majority of
content is concealed at all times (i.e. only one slide is
shown at a time). This can make it difficult to present
information that exists as multiple stages or steps, or
is inter-related in nature. Consider how to present in,
PowerPoint, the muscles and movements of the lower
limb, the coagulation cascade, or the life cycle of
malaria. You might be able to cram these topics into
80 slides, but, viewers are likely to forget the slide
that went before as you advance to the next, focusing
on snippets of information without being able to
appreciate the information’s relationship to what has
gone before.
Enter Dr. Holloway, who whipped up a new
presentation format: a ‘web-based hybrid mind-mapslideshow’, designed with pathology topics in mind.
That phrase wasn't really rolling off our tongues, so
we later called it 'OverPath'.
OverPath couples a left-sided mind-map to a rightsided presentation slide area in a web browser. The
JavaScript-based mind-map gives a visual, interactive
overview of a topic. Exploring the interactive mindmap calls up HTML-based slides, which explore the
topic in more detail.
79
Feature Article
# 2
Student Summer Research Awards Programme 2014:
Three Experiences
→
Figure 1
OverPath
in-browser.
Exploring the
mind map reveals
relevant slides
on the right.
Graphical representations like mind-maps are
justified in learning theory as providing overviews
of concepts, offloading some processing burden to
the visual brain and relating new learning to previous
knowledge.4 The brain organises knowledge
into hierarchical frameworks. Tools that emulate
or facilitate this process can enhance learning.4
Learning is also enhanced when continuous and
large topics are broken down into small, learnercontrolled sections,5 as in the mind-map.
As a student, it is a great feeling to be able to
contribute to the future of medical education. This
is part of what the SSRA programme offers you.
Medical education projects, specifically, benefit from
the counsel of their peers and faculty advisors and
at weekly meetings. This real-time feedback helped
substantially with staying on top of an evolving
project and with solving problems as they arose. This
was something that other SSRA students, working
mostly alone, ran into issues with.
Why not try it out yourself at the link below?
The next step for our team is to investigate whether
or not OverPath objectively enhances learning.
We hope to conduct such a case-control-like study
looking at OverPath’s effect on exam performance
soon.
http://www.url.ie/velo
The methods and results for this project have been
published elsewhere, so I won’t go into detail
here, but – after developing OverPath further, we
conducted a survey, to which 40 medical students
responded, which found a statistically significant
(p=<0.001) preference for OverPath over a static PDF
analogue in terms of perceived usefulness. This was a
great vindication of our work.
References
01 Tufte ER. The Cognitive Style of
PowerPoint. 2nd ed. Cheshire:
Graphics Press; 2006.
02 Gopal K, Morapakkam K.
Incorporating Concept Maps in a
Slide Presentation Tool for the
Classroom Environment. In Proc.
ED-MEDIA 2002. AACE, 2002.
03 House R, Watt A, Williams J.
What is PowerPoint? Educating
Engineering Students in its
Use and Abuse. In 35th ASEE/
IEEE Frontiers in Education Co
nference. IEEE, 2005.
04 Novak JD, Cañas AJ. The Theory
Underlying Concept Maps and How to
Construct and Use Them. Pensacola:
Florida Institute for Human and
Machine Cognition; 2006. http://
goo.gl/URIiN3.
05 Mayer RE. Applying the science of
learning to medical education.
Med Educ. 2010; 44(6): 543‐549.
doi:10.1111/j.1365‐2923.2010.03624.x
80
UCD Student Medical Journal
Written by
2 . P E T E R F RYC,
STAG E 4 U NDE RG R A DUAT E M E DI CI NE
Project Title
Opposing Effects of the HTLV-1 HBZ Protein on
Interferon Regulatory Factors 3 and 7 and Interferon
Production
Supervisors
Dr. Noreen Sheehy, J Murphy
Location
Centre for Research in Infectious Diseases, School of
Medicine and Medical Science, UCD
As part of the 2014 UCD Student Summer Research
I got to spend eight weeks working alongside an
inspiring group of scientists in the UCD Centre
for Research in Infectious Diseases, located by the
National Virus Reference Laboratory, in a building
that, as weeks went by, started to resemble a T4
bacteriophage due to its unusual architecture. The
research project focused on a relatively obscure
part of the oncogenic Human T Cell Leukemia
Virus (HTLV), the HBZ protein, and its interactions
with host immune system proteins. The crux of my
activities involved preparing plasmids, transfecting
HEK 293T cells with said plasmids and measuring
the corresponding transcriptional and translational
activity of the innate immunity Interferon pathway, via
Luciferase assays and Western Blotting respectively.
The noble, if not deluded goal was to add to
scientific knowledge, seeing further by standing on
the proverbial shoulders of giants, and to find out
whether HBZ is a viable therapeutic target in HTLV-1
infections.
Getting immersed in a scientific environment was a
serene and enjoyable experience. The hours were
quite flexible but generally the project involved a
nine-to-five schedule in the laboratory with outof-hours time spent reading papers and filling out
the infamous laboratory notebook. I also devoured
weekly instalments of ‘This Week in Virology’ (TWiV)
a podcast for virology aficionados. At times, reading
the scientific literature on molecular biology felt
like deciphering Sumerian cuneiform, a completely
foreign, esoteric language full of hard to grasp
acronyms and diagrams. But with persistence I
experienced amazing moments of clarity in which
Cathal Ahern
Peter Fryc
Caroline Moran
I made leaps in understanding the topic. The
acquisition of in-depth knowledge on one given
topic was very rewarding and put into perspective
the complexity of biological processes and the
potential for improvements in medicine when such
processes are fully understood. The literature review
made me realise how much modern medicine still
suffers from scant understanding of the molecular
mechanisms and still relies on clinical outcomes.as
was the case with the initial use of aminopterin in
leukemia.
The SSRA experience allows medical students a nice
start on the path to becoming proficient translational
practitioners. The projects allow students to improve
critical thinking skills, and the scientific literacy
involved with conducting research, presentation and
publishing of it. Even application writing, I learned
while submitting for the Wellcome scholarship, is
an art form in itself and a highly touted skill when it
comes to grants for the laboratory. Participants gain
valuable laboratory experience in key techniques
used commonly in medical investigations and
research. Understanding the processes and minutiae
of laboratory tests allows students to appreciate the
results, as in the case of Western Blotting and its use
in anti-HIV antibody testing in the clinical setting.
Feelings of ineptitude crept up every now and
then, as it felt almost absurd trying to get proficient
and confident in laboratory work in a short eight
week period. When it came to the experiments, I
sometimes wondered whether a small mistake or
omission on my part could skew the results. I lacked
confidence when providing conclusions. However
after some rumination, doubts turned into moderate
assertiveness. I realised that I did the work to the best
of my abilities. This realisation allowed me to take
pride in the results and conclusions that I presented
at the 2014 SSRA adjudications and in the abstract for
publication in the Irish Journal of Medical Sciences.
81
Feature Article
# 2
Student Summer Research Awards Programme 2014:
Three Experiences
3 . CAROLINE MORAN, STAGE 3 BI OMEDICAL, HE ALTH AND LIFE S CI E NCE S AND S S RA GOLD ME DALI ST 2 0 1 4
Project Title
Assessment of the development of neutralising
antibodies in mice following administration of
F/HN-lentivirus
Supervisors
Professor Uta Griesenbach, Dr. Kamila Pytel
Location
Imperial College London
The enticing possibility of spending the summer
abroad prompted me to take a different approach to
the normal SSRA process in which students apply for
advertised projects. I began searching for a research
project abroad by contacting various groups and
came across the UK Cystic Fibrosis Gene Therapy
Consortium based at Imperial College London.
The main focus of the Consortium at the moment
is to develop a viral vector carrying the CFTR gene
administered by inhalation. While this viral vector
is anticipated to treat Cystic Fibrosis, it may also be
exploited for the treatment of other lung diseases
such as chronic obstructive pulmonary disease.
Captivated and intrigued, I began to realise the true
impact of this innovative approach. Could this finally
be the cure that so many have hoped for? Following a
short trip to London in March to meet the coordinator
of the Consortium, preparations were put in place
and the idea of spending two months in London
during the summer soon became a reality.
Gene therapy, as with many things in research, is a
much more complex process than it appears and
many significant challenges currently impede its
clinical utility. Prior to progression to clinical trials, the
Consortium must establish the safety of CFTR viral
administration. While results obtained thus far appear
promising, the possibility of this virus inducing
antibody development and therefore stimulating
a potentially fatal cytokine storm is an important
aspect of safety which must be addressed. As part
of ongoing pre-clinical toxicology studies, I had the
task of analysing mice serum to determine whether
mice developed antibodies in response to repeated
viral administration and, if so, whether antibody
development depended on the viral dose.
Upon arrival in London, I was equipped with the
necessary background knowledge and essential
skills required to carry out the project. In addition
to regularly passaging cells, the project primarily
involved transduction inhibition assays whereby
cells were seeded, mixed with mice serum,
transduced with the virus and then whisked
away to the flow cytometry lab in Hammersmith.
Although I had no previous exposure to tissue
culture or virology laboratory procedures, I soon
became quite comfortable with the techniques as
I performed them on a daily basis. While acquiring
indispensable laboratory skills has been immensely
beneficial, the research process itself also allowed
me to further develop my analytical skills and to
consider alternative approaches to answering the
research question. Literature reviews, journal club
presentations and public engagement events
afforded me the opportunity to gain further insight
into the challenges facing the field of gene therapy.
To complement the lab research, I regularly visited
the nearby Royal Brompton Hospital where I
witnessed various tests being carried out as part of
clinical studies. I also had the opportunity to spend
time at the cystic fibrosis outpatient clinic in order
to understand the burden which this devastating
disease imposes and how gene therapy may
contribute to relieving the affliction.
In addition to gaining invaluable skills and a positive
insight into the field of inquiry, the promising results
obtained from the project itself have played a pivotal
role in confirming my desire for research. The simple
finding that prior treatment with a low dose of the
virus may induce immune tolerance in mice to
prevent antibody development has since prompted
further investigation. This discovery may play a role
in the dosing strategy used in clinical trials in the
future as subsequent administration of higher doses
of the virus may provide a means to increase efficacy
without increasing toxicity. Knowing that this research
may help contribute towards the clinical application
of viral gene therapy for cystic fibrosis someday
has added great value to an extremely rewarding
experience.
Bibliography: The UK Cystic Fibrosis Gene
Therapy Consortium, (2015). United Kingdom
Cystic Fibrosis Gene Therapy Consortium.
[online] Available at: http://www.
cfgenetherapy.org.uk/ [Accessed 23 Jan.
2015].
82
UCD Student Medical Journal
83
Feature Article
# 3
Bewilderment: A Symptom of, & Solution for Empathotoxicity
Bewilderment:
A Symptom
of, &
Solution
for
Empathotoxicity
Written by
Matthew Shipsey
Original Artwork
Photograph
Maser
Fay Teo
Follow the genius, Mandelstam. Totalitarian in his pursuit
of being, of truth, pursued by, and soon to succumb to,
Stalin’s agents of terror and icy exile:
Follow our poet, Seamus, and noli timere. Don’t be afraid.
(And, if you can, see the sheen of truth through the stain
of trite.)
How to be enchanted? How to be beguiled, by bewilderment?
Bewildered by the blossom
of now right up to
the rupture, and rapture,
of not.
There he is, answering
the call.
Blossoms rupture and rapture the air,
All hover and hammer,
Time intensified and time intolerable,
sweetness raveling rot,
It is now. It is not vii
What is this dire delight, flowering fleeing always earth?
What is being? What is truth?
And I was alive in the blizzard of the blossoming pear,
Myself I stood in the storm of the bird-cherry tree.
It was all leaflife and star-shower, unerring, self-shattering
power,
And it was all aimed at me.
Feature Article
# 3
While the collapse sounds familiar, it is the enchantment
with which we should try to relate, and on a daily basis.
Bewilderment, writes one American poet, is “a way of
entering the day… an enchantment that follows a complete
collapse of reference and reconcilability.”vi
But bewilderment is a fascinating condition, and the
natural history does not necessitate sleep-deprivation and
anxiety, the prognostication need not end morbidly.
85
Bewilderment. This is a condition with which all medical
students are well acquainted. Walk into an embryology
anatomy lecture, and the symptoms will be writ large. Take
a peek into the library before finals, the signs will be
screaming in their tortured silence. The etiology can be
traced to the seemingly endless amount of things we can
know about a seemingly endless amount of things we need to
know.
Matthew Shipsey
“What is being?” “What is truth?” v
Jaysus... is that not lovely, and subtle?
olé, some say, is etymologically linked to Allah, interjected by spectators of the Spanish Sufi whirling dervishes and their
hypnotic, heavenly dances.
There we are, answering the call. The chant heard around the country, proclaiming or invoking the sublime. Did you ever
wonder... how it got here though? Go ask our sallow-skinned kinsfolk in mighty Mayo.
Written by
Olé! Olé, olé, olé!
But sometimes, the call is answered.
UCD Student Medical Journal
Our rejoinder? A dull percussion of blank faces, poker players all. Sympathetic, but
noncommittal sniggers. What arithmetic underlies our calculated indifference?
“Did you ever wonder…” he begins.ii
“Is that not lovely, and subtle?” she asks.iii
“If you think about that, it’s pretty amazing,” he says.iv
But sometimes, the call is answered.
Usually, it seems to resonate dull, or to a chorus
of sympathetic, but noncommittal sniggers.
The call comes through the lecture hall now, and again.
“Attention! Here
and now!”i
84
Bewilderment: A Symptom of, & Solution for Empathotoxicity
And if you think about that, it’s pretty amazing.
The bottom line is that we have all worked so hard for our privileged seat at the
precipice of life’s circumference. Being alive to the amazing experience of being alive,
of being and of life, the glimmerings of your soul in communion with the elegance of
hairpin loops and hand-held human-hearts, is to be enchanted by the bewilderment. It
requires attention, and discipline, “this is water, this is water,” but someday quite
soon, it may well help you to heal, to restore a life to wholeness, to health. xvi
- Mary Oliver
Newman, John Henry. The Idea of a
University Defined and Illustrated.
Chicago: Loyola University Press.
1987
Frankl, Victor. Man’s Search For
Meaning. London: Rider. 2004
Oliver, Mary. Red Bird. Newcastle:
Bloodaxe Books. 2008
xvi Wallace, David Foster. This is
Water: Some Thoughts, Delivered on a
Significant Occasion, about Living a
Compassionate Life
xv
xivIbid
xiii Wiman, Christian. My Bright Abyss:
Meditation of a Modern Believer. New
York: Farrar Straus Giroux. 2014
xii Heaney, Seamus. Station Island.
London: Faber & Faber. 2011
xi
x
ixhttp://opinionator.blogs.nytimes.
com/2013/10/02/who-will-heal-thedoctors/
viiihttp://opinionator.blogs.nytimes.
com/2013/09/18/medicines-search-formeaning/
Feature Article
# 3
Pay attention. Be astonished.
Tell about it.xv
Howe, Fanny. The Wedding Dress:
Meditations on Word and Life.
Oakland: University of California
Press. 2002
vi
vii Mandelstam, Osip. Stolen Air:
Selected Poems of Osip Mandelstam.
Trans. Christian Wiman. New York:
Ecco, 2012.
Mandelstam, Osip. Stolen Air:
Selected Poems of Osip Mandelstam.
Trans. Christian Wiman. New York:
Ecco, 2012.
Jones, James. UCD School of Medicine
& Medical Science
v
iv
87
Instructions for living a life:
Taylor, Cormac. UCD School of
Medicine & Medical Science
Huxley, Aldous. The Island. London:
Vintage Classics, 2005
iii Costello, Christine. UCD School of
Medicine & Medical Science
ii
i
Matthew Shipsey
“The soul is not simply the agent that does the seeing, it is in
some way the things that are seen; or, perhaps more accurately,
the soul is the verb that makes an exchange between the self
and reality – or the self and other selves – possible. It is the
soul that turns perception into communication, and
communication – even if it’s just between one man and the
storm of atoms around him – into communion.” xiv
To entertain the possibility that there is wisdom in this discussion of
truth, and knowledge, let us pare back the burdensome “R” word, the same
way “faith itself sometimes needs to be stripped of its social and
historical encrustations and returned to its first, churchless incarnation
in the human heart,” as Christian Wiman, an American poet has it.xiii This,
I think, leaves us in view of the soul’s glimmering splendor, and it is in
this light, and through this light, that one might find a way to answer
the call. Wiman again:
Venturing to mention a word like “soul” to a postmodern audience, let
alone a scientific one, is a precarious undertaking. Aligning “religious”
beside “truth,” and putting both astride “general knowledge,” as our
college founder Cardinal Henry Newman famously did in his “Ideas on a
University,” is probably as likely to induce apoplexy as grade IV
hypertension.
“Religious Truth is not only
a portion, but a condition of
general knowledge.” xi
“Glimmerings are what the
soul’s composed of.” xii
Written by
The call is to be answered.
The compassionate and
miraculous doctor you’ve
dreamt of becoming may well be
pleading at the other end of
the line.
But, if Viktor Frankl is to be
believed, “everything can be
taken from a man but one
thing: the last of the human
freedoms – to choose one’s
attitude in any given set of
circumstances, to choose one’s
own way.”x Seventy years ago,
Frankl emerged from the
concentration camps with this
message to tell: the choice is
always there, and it is yours
to make.
A system predicated on
restoring humans to the full
health which instead is
destroying the mental and
physical health of the humans
dedicated to that restoration;
insidious, indeed.
educators’ call to
bewilderment fails to enchant,
I fear the choice of fear is
being made for us. And all the
rumblings from downfield
suggest that this is a choice
not easily-unchosen.
UCD Student Medical Journal
My fear is that the
dehumanizing process of the
medical system has already
begun, insidiously. When the
“zoo of the new” in which we
traipse daily effects only
wringing of hands, when our
By many, many accounts, there
is much to fear in our
particular, precarious future
as physicians. Indeed, there
seems to be a philosophical
pandemic in the profession, an
outbreak of dissatisfaction,
distress, depression. Only 40%
of American physicians would
recommend the career to their
children.viii Moreover, burnout
is said to begin as soon as
you enter the hospitals. That
is to say, it begins in
medical school. The notion of
medical school as an
“empathotoxin” began picking
up serious traction when a
systematic review of research
in medical students and
residents found nearly one
half of those surveyed met the
criteria for burnout
(exhaustion,
depersonalization, and reduced
satisfaction in performance).
Painful though it is to
report, 11% were found to have
being suffering from suicide
ideation.ix
“Noli
Timere”
86
Bewilderment: A Symptom of, & Solution for Empathotoxicity
http://ucdsmj.com
UCD Student Medical Journal
Edition 2
Student
Credit Card,
your travel
insurance is
on us
Get a BOI student
credit card with
free worldwide
multitrip travel
insurance included
Talk to us in Montrose branch today
076 6231266
Lending criteria and terms and conditions apply, which are available on bankofireland.com/studentcreditcard. You must be over 18 years of age. Credit
cards are liable to Government Stamp Duty of €30. This feature is available to Bank of Ireland third level current account holders whose accounts remain
open and active for the duration of the insurance policy to ensure claims are paid. Bank of Ireland reserves the right to withdraw this feature at any time, but
will notify you if this change takes place. BOI refers to Bank of Ireland. Travel insurance is arranged by Bank of Ireland Insurance Services Limited. Bank of
Ireland Insurance Services Limited is a member of the Bank of Ireland Group. Bank of Ireland Insurance Services Limited is regulated by the Central Bank of
Ireland. The Travel Insurance cover is underwritten by AIG Europe Limited. AIG Europe Limited is authorised by the Prudential Regulation Authority of the United
Kingdom and is regulated by the Central Bank of Ireland for conduct of business rules. Travel insurance terms and conditions are available at bankofireland.
com/studentcreditcard. Bank of Ireland is regulated by the Central Bank of Ireland.