ASTRO 2003: High dose Tx for Lung Ca
Agenda
Pre-Treatment
Normal Tissue Imaging
•
•
Normal tissue definition: not always so obvious
Anatomy vs. function
During Treatment (not much)
• Changes in normal anatomy/function
• Secondary changes due to tumor response (Kong)
Lawrence B. Marks, M.D.
Radiation Oncology
University of North Carolina at Chapel Hill
Post-Treatment
• Imaging to detect normal tissue injury
UNC
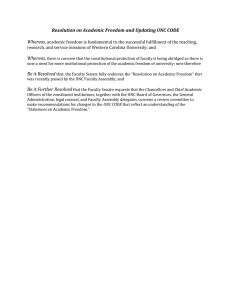
Anatomy
Function
UNC
L. Marks/jh
Anatomy
Function
•CTCT-based planning
•Actually pretty good!
•Physiologic understanding
•Better!
UNC
ASTRO 2003: High dose Tx for Lung Ca
Tubules that
go deeper into
the medullary
portion of the
kidney do
MORE urine
concentrating
UNC
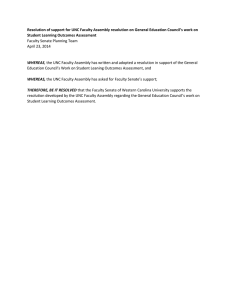
Incorporating
anatomic/functional
information to improve
CT-based planning:
Esophagus
UNC
L. Marks/jh
3D dose
distribution
DVH
Outcome
(symptom)
UNC
ASTRO 2003: High dose Tx for Lung Ca
3D dose
distribution
DVH
Outcome
(symptom)
Anatomy
Physiology
Spatial information
Esophagus contours:
variable area
(volume)
Anatomically
Correct DVH
UNC
Superior
UNC
Toxicity = f (Dosimetric Parameters)
Inferior
p-values
V 50
Uncorrected
Acute ≥ grade 2
V 50
Corrected
0.008
0.005
Acute ≥ grade 3
0.05
0.003
Adapted from Kahn et al. 2004 (Duke)
UNC
L. Marks/jh
Late ≥ grade 1
0.14
0.08
UNC
ASTRO 2003: High dose Tx for Lung Ca
CT + Anatomy,
physiology
>
CT alone
UNC
Pre-Treatment Normal Lung?
Volume, Perfusion, Ventilation
UNC
CT
SPECT (DFH)
UNC
Fan (Duke) : IJROBP 51:311-7, 2001
L. Marks/jh
of SPECT-Defined
Lung Volume
of CT-Defined
Lung Volume
Functional Imaging Paper
From Marks, Spencer, Sherouse et al. IJROBP 33:65-75 1995
UNC
ASTRO 2003: High dose Tx for Lung Ca
Frequency of heterogeneity on SPECT (%)
At
All Patients* (n
(n=50)
<1.3 (12)
FEV1a
≥1.3 (37)
DLCOa
<12 (11)
≥12 (34)
COPD hx yes (23)
no (27)
Tobacco yes (45)
no (5)
Adjacent to Separate from
tumor site
tumor site
tumor site
84
100
92
100
91
100
89
96
80
74
83
73
82
71
65
81
78
40
42
83
30
73
35
65
22
44
20
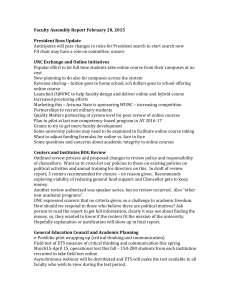
Traditional 3D planning
Not much
flexibility
Target
Size
Flexibility &
Need (gain)
Lesser need
Pulmonary Function
* With gross disease: i.e. excludes post-op
cases
Marks et al. IJROBP 33:65-75 1995
A Lowest vs upper 3 quartiles
Univ North Carolina
FunctionFunction-based Lung Treatment Planning
With IMRT
•More of this space is
applicable
Target
Size
•Complex shapes morereadily addressed
•Clinically useful??
Pulmonary Function
UNC
L. Marks/jh
UNC
• Duke (Marks 1995, McGuire
2005)
• NKI (Seppenwoolde
(Seppenwoolde 2000)
• MDAH (Sh
ioyama
ama 2007)
(Shioy
• Marsden (Lavrenkov 2007,
Christian 2005)
• Michigan (Ten Haken,
Haken, Kong)
• MRI; Sheffield (Ireland 2007)
SPECT
& IMRT
UNC
ASTRO 2003: High dose Tx for Lung Ca
CT Plan
PTV
Boost
SPECT Plan
SPECT Plan
optimizes
regions by
functionality
Duke
PTV
Boost
CTCT-based
plan
Duke McGuire et al.
IJROBP 66:15431552, 2006 UNC
Optimize per
DVH’
DVH’s
CTCT-based
plan
Compare
SPECTSPECT-based
metrics
SPECTSPECTbased plan
Optimized based
on SPECT
UNC
L. Marks/jh
UNC
Ha Ha:
SPECT is
better!!
SPECTSPECTbased plan
Optimize per
DVH’
DVH’s
Compare
SPECTSPECT-based
metrics
Optimized based
on SPECT
UNC
ASTRO 2003: High dose Tx for Lung Ca
Can’t assume IMRT will “clean it up”. Beam
direction selection matters
Dose Distributions
UNC
Imaging changes in normal
tissue during/after therapy
UNC
Patient #1
Pre-RT
SPECT
UNC
L. Marks/jh
Pre-RT
CT
6 month
Post-RT
SPECT,
67 Gy
UNC
From Marks et al. IJROBP 26:659-668 1993.
ASTRO 2003: High dose Tx for Lung Ca
PostPost-RT
33Gy
%
Reduction
Regional
Perfusion
PrePre-RT
33Gy
UNC
100
80
60
40
20
0
0
20 40 60 80 100
Regional Dose (Gy)
Slope of Dose Response Curve
Junan Zhang 2006
6-month Population DRC
Junan Zhang and Sumin Zhou 2006
UNC
L. Marks/jh
UNC
ASTRO 2003: High dose Tx for Lung Ca
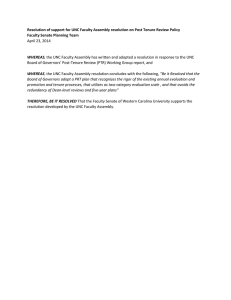
Overall Group
Predicting Changes in PFT’
PFT’s
Dmax
y=x
40
∑ [(fraction lung at dose i) ×
i=0
60
(effect at dose i)] = total loss
96 patients with followfollow-up
PFT’
PFT’s ≥ 6 months
Actual 20
Reduction
DLCO 0
(%) -20
-40
R = 0.30, p = 0.005
-60
0
10
20
30
40
50
Predicted Reduction in PFTs (%)
Fan et al. JCO and IJROBP 2001
Duke University
Duke University
New Defect
Pre-RT
Univ North Carolina
L. Marks/jh
Post-RT
UNC
% of Patients with New Defects
ASTRO 2003: High dose Tx for Lung Ca
Incidence = f (volume)
80
13
9
17
25
60
17
40
22
11
12 5-10% LV
11
9
10
9 > 10% LV
19
11
22
13
20
6 1-5% LV
< 1% LV
33
4
0
0
14
6
12
18
24
30
36*
Time post-RT (months)
UNC
Location: Anterior, RT Field
Microvascular injury
(Within months of RT)
20%
15%
EF decreases
10%
Decline in 5%
Ejection
0%
Fraction
(pre-post) -5%
Reduced collateral
flow/reserve
(often subclinical)
-10%
EF increases
-15%
UNC
Coronary Artery
Disease
(years/decades
post-RT)
Reduced flow to
myocardial “territory”
-20%
0
Marks 2005
5
10
15
Summed Rest Score
UNC
L. Marks/jh
Combine to
cause ischemia
UNC
ASTRO 2003: High dose Tx for Lung Ca
Brain
Summary
Pre-Treatment
•
•
(FDG) PET Registration
Planning MRI
Normal tissue definition: not always so obvious
Anatomy vs. function
During Treatment (not much- more coming)
• Changes in normal anatomy/function
• Secondary changes due to tumor response
Relative blood flow
%FDG ↓
Post-Treatment
• Imaging to detect normal tissue injury
↑
%15O↑
↑
Metabolism
Dose
Dose
3 weeks f/u
UNC
Duke, Hahn CA, et al: IJROBP 2009
Acknowledgements
Radiation Oncology/Physics
•
•
•
•
•
•
•
•
•
•
Janet Bailey
David Fried
Liyi Xie
Jessica Hubbs
Junan Zhang
Micheal Lawrence
Sumin Zhou, Ph.D
Shiva Das, PhD
Junan Zhang, PhD
Daniel Kahn, PhD
Pulmonary:
Pulmonary:
• Patricia Rivera, MD
• Rod Folz, MD
Nuclear Medicine
• William McCartney, MD
• Arif Sheik, MD
• Terrence Wong, MD, PhD
• Salvador BorgesBorges-Neto, MD
Data Management/Statistics
• Donna Hollis, MS
• Robert Clough, BA
UNC for PLUNC Tx Planning Software
NIH and DOD Grants
L. Marks/jh
UNC
UNC
 0
0