15 Role of Ocular Motor Assessment in Diagnosis and Research
advertisement

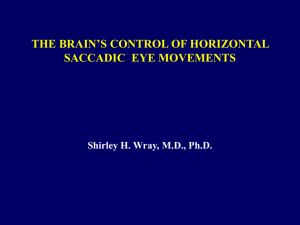
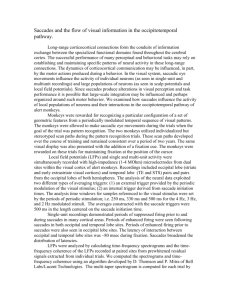
Role of Ocular Motor Assessment 235 15 Role of Ocular Motor Assessment in Diagnosis and Research R. John Leigh and David S. Zee INTRODUCTION The clinical evaluation of eye movements can contribute substantially to the diagnosis of parkinsonian disorders, provided the physician performs a proper examination and interprets the findings by referring to a simple scheme of the neurobiology of eye movements (1). Further diagnostic information can often be obtained by recording eye movements, which are more accessible to measurement and analysis than limb movements or gait. A good part of the neurobiological substrate of eye movements has been defined, which makes it possible to attribute disordered properties of eye movements to dysfunction of specific neuronal populations or structures in the brain. In this chapter, first, we review pertinent aspects of the ocular motor examination; second, we highlight some important test paradigms and technical aspects of measuring eye movements; and third, we summarize disorders of ocular motility reported with parkinsonian disorders and diseases affecting the basal ganglia. CLINICAL EXAMINATION OF EYE MOVEMENTS IN PARKINSONISM The systematic examination of eye movements is summarized in Table 1. The most useful part of the examination concerns saccades, which are the rapid eye movements by which we voluntarily move our line of sight (direction of gaze). Saccades are perhaps the best understood of all movements both in terms of their dynamic properties and neurobiology (1–3). It is important to differentiate between limited range of movement, especially upward, and speed of saccades, especially vertically. Normal elderly subjects show limited upgaze (4), and this may be because of changes in the connective tissues of the orbit (5). Nonetheless, some normal elderly subjects make vertical saccades that have normal velocities, within their restricted range of motion (6). Range of movement is conventionally elicited as the patient attempts to follow the examiner’s moving finger, but this does not test saccades. It is important to ask the patient to shift gaze on command between two stationary visual targets, displaced horizontally or vertically, such as a pencil tip and the examiner’s nose. After each verbal cue (e.g., “look at the pencil; now look at my nose”), note the time taken to initiate the saccade, its speed, and whether it gets the eye on target, or whether further corrective saccades are needed. It is also useful to ask parkinsonian patients to make saccades voluntarily at a rapid pace back and forth between two stationary targets (e.g., a finger from the left and right hand of the examiner. Patients with idiopathic Parkinson’s disease (PD) often have difficulty making such self-generated sequences and several saccades, rather than one, are needed for the eye to reach the target (see video 1). From: Current Clinical Neurology: Atypical Parkinsonian Disorders Edited by: I. Litvan © Humana Press Inc., Totowa, NJ 235 236 Leigh and Zee Table 1 Summary of Eye Movement Examination • Establishment of the range of ocular motility in horizontal and vertical planes • Fixation stability in central and eccentric gaze (looking for nystagmus or saccades that intrude on steady fixation) • Horizontal and vertical saccades made voluntarily between two fixed visual targets (noting initiation time, speed, and accuracy) • Horizontal and vertical pursuit of a smoothly moving target (looking for “catch-up” saccades) • “Optokinetic nystagmus” induced with horizontal or vertical motion of a hand-held drum or tape • Ocular alignment during fixation of a distant target, and vergence responses to smooth or stepping motion of targets aligned in the patient’s sagittal plane • The vestibular ocular reflex in response to smooth sinusoidal, or sudden, head rotations in horizontal and vertical planes (looking for corrective saccades that accompany or follow the head rotation) Another important feature of many parkinsonian disorders is inappropriate saccades that intrude on steady fixation; the most common are small “square-wave jerks” that are most easily appreciated during ophthalmoscopy as to-and-fro movements of the fundus. Smooth pursuit is not usually helpful, because many elderly normal subjects and even some younger subjects may have impaired pursuit that requires catch-up saccades to keep the line of sight on the moving target. Optokinetic stimulation at the bedside may be useful in some patients who have difficulty initiating voluntary saccades (e.g., progressive supranuclear palsy [PSP]); vertical drum motion may induce tonic vertical deviation of the eyes in affected individuals or evoke reflexive “quick phases” of nystagmus. Vergence is also often impaired in normal elderly subjects, and identification of abnormalities may require laboratory assessment. A NOTE ON LABORATORY METHODS FOR STUDYING EYE MOVEMENTS IN PARKINSONIAN DISORDERS Perhaps the most important diagnostic contribution to be made by recording eye movements in parkinsonian disorders concerns tests of vertical saccades (7,8). Reliable measurement of horizontal or vertical saccades requires methods with adequate bandwidth (0–150 Hz), sensitivity (0.1°), and linear range (±30°). DC-amplified electro-oculography (EOG) is adequate to signal horizontal eye position and timing at the beginning and end of a saccade, but is unreliable for measuring vertical movements. Infrared methods provide better bandwidth but inferior range to EOG, and also cannot be used to measure vertical movements. The most reliable method is the magnetic search coil which, in our experience, is well tolerated by frail and elderly subjects, and has the added advantage of being calibrated independently of the patient’s voluntary range of movements (1). Fast frame-rate videobased techniques are suitable for measuring dynamic properties of horizontal and vertical saccades (9), but their calibration depends on the ability of the patient to look at visual targets, and this may be impaired, for example, in PSP. Saccades show consistent relationships between their size, speed, and duration (2,10). Thus, the bigger the saccade, the greater its peak velocity and the longer it lasts. Examples of the “main sequence” relationships between peak velocity, duration, and amplitude are provided from normal subjects in Fig. 1; exponential or power-function equations have been used to describe these relationships and define prediction intervals for normal subjects (2,10,11). Deviations of measured eye movements from these relationships indicate either abnormal saccades, or nonsaccadic eye movements. Thus, in Fig. 1, we also provide an example of abnormally slow vertical saccades from a patient with PSP. Role of Ocular Motor Assessment 237 Fig. 1. Plots summarizing important dynamic properties of saccades. (A) Plot of peak velocity vs amplitude of vertical saccades. Data points are saccades from 10 normal subjects. The data are fit with an exponential equation; also plotted are the 5% and 95% prediction intervals. The + indicate vertical saccades from a patient with PSP, which lie outside the prediction intervals for normals. (B) Plot of duration vs amplitude. The data from 10 normal subjects are fit with a power equation. The + indicate vertical saccades from a patient with PSP, which have greater duration than control subjects. Aside from measurement of saccadic dynamics, substantial effort has been put into using saccades as a behavioral index of motor programming in basal ganglia and associated cortical disorders (12). Thus, although the frontal and parietal eye fields project directly to the brainstem centers, such as the superior colliculus and pontine nuclei, a second pathway running through the basal ganglia plays an important role, and comprises the caudate, substantia nigra par reticulata (SNpr), subthalamic nucleus, and superior colliculus (Fig. 2). A simplified view of this basal ganglia pathway is that it is composed of two serial, inhibitory links: a caudate-SNpr inhibition, which is only phasically active, and a SNprcollicular inhibition, which is tonically active (13). If frontal cortex causes caudate neurons to fire, then the SNpr-collicular inhibition is removed and the superior colliculus is able to activate a saccade. In addition, the subthalamic nucleus contains neurons that discharge in relation to saccades and 238 Leigh and Zee Fig. 2. (A) Block diagram of the major structures that project to the brainstem saccade generator (premotor burst neurons in PPRF and riMLF). Also shown are projections from cortical eye fields to superior colliculus. FEF, frontal eye fields; SEF, supplementary eye fields; DLPC, dorsolateral prefrontal cortex; IML, intramedullary lamina of thalamus; PEF, parietal eye fields (LIP); PPC, posterior parietal cortex; SNpr, substantia nigra, pars reticulata. excites (SNpr), which in turn inhibits the superior colliculus. Animal studies indicate that this pathway appears important for programming of saccades to targets for which there is an expectation of reward (14,15). The caudate nucleus also probably contributes to smooth pursuit (16). For these reasons, studies of the effects of human diseases affecting basal ganglia have focused on behaviors such as memory-guided or predictive saccades (Fig. 3). Memory-guided saccades are made in darkness several seconds after a visual target has been flashed. Predictive saccades are made in anticipation of a target appearance or jump. In the anti-saccade task, the subject is required to look in the opposite direction (mirror image position) to a visual stimulus. Thus, a reflexive, visually guided saccade must be inhibited and a saccade to an imagined target made instead (17). Such testing is still mainly a research tool, but it has provided insights into the pathogenesis of parkinsonian disorders, as we will mention in discussing each type of disorder. Role of Ocular Motor Assessment 239 Fig. 3. Schematic summary of stimulus paradigms that have been used to test saccades in Parkinsonian disorders. (A) Simultaneous switching of fixation target off and visual target on (overlap paradigm). (B) Gap paradigm, in which fixation target is switched off before visual target is switched on. (C) Memory target task. The subject views the fixation target during the time that the visual target is flashed and after several seconds (the memory period), the fixation light is switched off and the subject looks toward the remembered location of the target. (D) The antisaccade task. The subject is required to look in the opposite direction when the visual stimulus is presented. (E) Predictive task. Subject makes saccades to a target that jumps to a predictable location with predictable timing. 240 Leigh and Zee IDIOPATHIC PARKINSON’S DISEASE (TABLE 2) Clinical Findings in PD Most patients with PD show relatively minor abnormalities at the bedside that may also occur in healthy elderly subjects. For example, steady fixation may be disrupted by saccadic intrusions (square-wave jerks) (18–20), but these are also seen in some normal elderly subjects. Moderate restriction of the range of upward gaze is common in elderly individuals (4), with or without parkinsonism, and has been attributed to changes in the orbital tissues (5). Similarly, smooth pursuit can be impaired in PD but is also abnormal in some healthy normals (21). Convergence insufficiency is common and sometimes symptomatic (22). Patients with PD often have lid lag. Patients with advanced PD may show some slowing of vertical saccades, but PSP should always be considered in such cases. A characteristic sign in PD is that hypometria becomes more marked when patients are asked to rapidly perform self-paced refixations between two continuously visible targets (e.g., a finger of the examiners right and left hand about 60–80° apart; the normal horizontal ocular motor range is about 45° to either side) (video 1). Laboratory Findings in PD Saccades Saccades in PD usually undershoot the target (i.e., they are hypometric), especially vertically (20,21). Patients may show a “stair-case” of saccades to acquire the target (especially with remembered targets); this “fragmentation” has been interpreted as a robust correction mechanism to compensate for the underlying hypometria (23). It has been possible to investigate the pathogenesis of the hypometria, which becomes more marked when patients are asked to make self-paced refixations between two continuously visible targets. This phenomenon is not simply because of the persistence of the visual targets, because saccades made in anticipation of the appearance of a target light at a remembered location are also hypometric (24,25). Patients with PD have difficulty in generating sequences of memory-guided saccades (26–28), whereas saccades made reflexively to novel visual stimuli are normal in size and promptly initiated (7). Furthermore, visually guided adaptation of saccades is preserved whereas memory guided adaptation of saccades is impaired (29). Thus, it appears that PD patients are unable to generate internally guided saccades to accurately shift gaze (7,30). Despite this hypometria, patients can still shift their gaze with a series of saccades to the location of a briefly flashed target; this indicates a retained ability to encode the location of objects in extrapersonal space (20,24). The reaction time (latency) of saccades made in response to nonpredictable target jumps may be normal or mildly increased (20,30). During self-paced refixations between two visible targets, intersaccadic intervals increase above the latency of responses to nonpredictable target jumps (30,31) If the fixation light is turned out 100 msec before a target light appears (“gap” paradigm—Fig. 3) PD patients are able to make short-latency (100–130 ms) “express saccades” like normal subjects (7). The pathophysiology of saccadic disorders in PD is not fully understood. One possible mechanism is via the subthalamic nucleus (Fig. 2), which contains neurons that discharge in relation to saccades. The subthalamic nucleus is hyperactive in PD, and excites the substantia nigra, pars reticulata (SNpr), which in turn inhibits the superior colliculus. It may be that excess activity in SNpr in PD leads to a defect in generation of the more voluntary, internally guided saccades such as those during prediction and to memorized targets. Functional imaging studies have suggested that the basal ganglia are important for processing of temporal information (32), which may be important for generating a regular series of saccades. Furthermore, during predictive visuomanual tracking, there is an underactivity of sensorimotor cortex, but increase in premotor areas, such as pre-SMA (supplementary motor area), which may represent compensation or impaired suppression (33). Finally, PD also affects the dopaminergic Role of Ocular Motor Assessment 241 Table 2 Summary of Disordered Eye Movements in Some Basal Ganglia Disorders Progressive Supranuclear Palsy (PSP) • Slow vertical saccades, especially down, with a preserved range of movement, may be the first sign of the disorder; later, loss of vertical saccades and quick phases • Horizontal saccades become slow and hypometric • Disruption of steady gaze by horizontal saccadic intrusions (square-wave jerks) • Impaired smooth pursuit, vertically (reduced range) and horizontally (with catch-up saccades) • Smooth eye-head tracking may be relatively preserved, especially vertically • Preservation of slow phases of vestibular ocular reflex but quick phases are affected as saccades • Horizontal disconjugacy suggesting INO • Loss of convergence • Ultimately, all eye movements may be lost, but vestibular movements are the last to go • Eyelid disorders: apraxia of lid opening, lid lag, blepharospasm, inability to suppress a blink to a bright light. Parkinson’s Disease • Fixation may be disrupted by square-wave jerks • Hypometria of horizontal and vertical saccades, especially when patients are asked to perform selfpaced refixations between two continuously visible targets • Normal saccadic velocity except in some advanced cases • Impaired smooth pursuit, horizontally and vertically, owing partly to inadequate catch-up saccades • Vestibular eye movements normal for natural head movements • Impaired convergence • Oculogyric crises • Lid lag Huntington’s Disease • • • • • Difficulties initiating saccades (without an associated head thrust and blink) Difficulties suppressing saccades to novel visual stimuli (especially during the antisaccade task) Slow saccades, especially vertically, and in patients with early age of onset Impairment of smooth pursuit Preservation of VOR and gaze-holding cells within the retina. PD patients have abnormalities of color vision and in detection of spatially and temporally modulated gratings (34). Smooth Pursuit Mildly affected PD patients differ little from age-matched control subjects in their smooth-pursuit performance (21,35). During tracking of a target moving in a predictable, sinusoidal pattern, eye speed is less than target speed, leading to catch-up saccades (20,36). In addition, the catch-up saccades are hypometric; thus, the cumulative tracking eye movement is less than that of the target (35). Despite these impairments, the phase relationship between eye and target movement is normal,30 implying a normal predictive smooth tracking strategy. This is in contrast to saccadic tracking of predictive target jumps which, as described earlier, is deficient. Vestibular Responses Both caloric and low-frequency rotational vestibular responses, in darkness, may be hypoactive in patients with PD (37,38). However, at higher frequencies of head rotation, and particularly during visual fixation, the vestibular ocular (VOR) reflex adequately compensates for head perturbations, which accounts for the lack of complaint of oscillopsia in patients with PD. 242 Leigh and Zee Effects of Disease Course and Treatment Patients with advanced PD may show greater defects on more demanding tests, such as making memory-guided saccades, and on the anti-saccade tasks (Fig. 3), which requires inhibiting a reflexive saccade, and looking in the opposite direction to the target (its mirror location). In addition, patients with advanced disease may show some slowing of vertical or horizontal saccades. In general, L-dopa treatment of PD does not seem to improve the ocular motor deficits except for improvement of saccadic accuracy (i.e., saccades become larger) (36,39). Some newly diagnosed patients with idiopathic PD may show improved smooth pursuit after the institution of dopaminergic therapy (39). Memory-guided saccades are reported to be impaired after pallidotomy for PD (40), but improved with subthalamic nucleus stimulation (41), possibly by improving learning abilities in the corticobasal ganglia network (42). Pallidotomy increases saccadic intrusions on steady fixation (square-wave jerks) (43,44). Toxic Parkinsonism In patients with parkinsonism owing to methyl-4-phenyl-1,2,3,6-tetrahydropyridine (MPTP) toxicity, saccadic latency is shortened and saccadic accuracy improved by dopaminergic agents; in addition, reflex blepharospasm was improved (45). In monkeys that received MPTP, saccadic abnormalities, including increased latency, increased duration, decreased rate of spontaneous saccades, and inappropriate saccades, were all reversed by dopaminergic therapy (46,47). PROGRESSIVE SUPRANUCLEAR PALSY Clinical Features PSP is a degenerative disease of later life characterized by abnormal vertical saccades; the early appearance of falls, usually within a year of onset, owing to disturbance of tone and posture; difficulties with swallowing and speech; and mental slowing (48). Median survival time is about 6 yr. The disturbance of eye movements is usually present early in the course, but occasionally develops late, or is sometimes not noted by the patient’s physicians (49). Patient may complain of blurred vision, double vision, or photophobia (48), and have often been fitted with several different spectacle refractions, without improvement. On direct questioning, it is usually possible to determine that these visual complaints are a result of loss of the ability to voluntarily shift gaze in the vertical plane so that, for example, patients cannot look down to see a plate of food, tie their shoes, or confidently navigate going down the stairs. The initial ocular motor deficit consists of slowing of vertical saccades and quick phases, either down or up or both (see video 2). Sometimes vertical saccades take a curved or oblique trajectory (“round the houses”) (21,50). Vertical smooth pursuit is relatively preserved, but of decreased gain (51). Larger targets may elicit greater responses (52), and could be used to evaluate the range of eye movements in patients in whom neck stiffness makes testing of the VOR technically difficult. Similarly, full-field optokinetic stimuli may induce responses that are useful for analysis (11). Combined eye-head tracking may also be relatively spared. As the disease progresses, the range of movements possible with vertical saccades and pursuit declines and eventually no voluntary vertical eye movements are possible. However, the VOR is preserved until late in the disease (although a characteristic rigidity of the neck may make the vertical doll’s head maneuver difficult to elicit). Horizontal eye movements also show characteristic changes: steady fixation is disrupted by squarewave jerks (11,18,21), which are more common than in other parkinsonian disorders. Horizontal saccades are initially hypometric but normal in speed (see video 3) (53); as the disease progresses, they also become slow. In some patients, the involvement of horizontal saccades resembles inter- Role of Ocular Motor Assessment 243 nuclear ophthalmoplegia (INO), although vestibular stimulation may overcome the limitation of adduction (54). Horizontal smooth pursuit appears impaired, in part, because of square-wave jerks. Convergence eye movements are commonly impaired (55). Late in the disease, the ocular motor deficit may progress to a complete ophthalmoplegia. Patients with absent quick phases but intact vestibular eye movements may also show sustained deviation of the eyes in the orbit during body rotation, and if the head is free to move it too may deviate opposite to the direction of body rotation (56). There are a variety of eyelid abnormalities in PSP: blepharospasm, lid-opening apraxia, eye-closing apraxia, lid retraction, and lid lag (21). Patients typically show an inability to suppress a blink to a bright light—a visual Meyerson’s (glabella) sign (see video 4) (57). A single patient may have more than one of these abnormalities. Bell’s phenomenon is usually absent. Laboratory Findings in PSP Saccades Reliable measurements of saccades in PSP have demonstrated that vertical saccades are slower than horizontal saccades of similar size (21,58). For patients who are able to make only small saccades, it is still possible to determine whether the movements are slowed using an appropriate statistical approach (59). Vertical saccades are generated by “burst neurons” in the midbrain but horizontal saccades are generated by burst neurons in the pons. Thus, the selective involvement of vertical saccades in the early stage of PSP has indicated that the brunt of the disease initially falls on midbrain burst neurons, or their local circuitry (superior colliculus and the adjacent central mesencephalic reticular formation) (60,61). The latency (reaction time) of horizontal saccades in PSP is prolonged in some patients, but others retain the ability to make short-latency or “express” saccades (62). Patients with PSP also make errors when they are required to look in the opposite direction to a suddenly appearing target (the antisaccade task—Fig. 3). Both the presence of express saccades and errors on the antisaccade task suggest defects in frontal lobe function and, although neuropathological changes there are mild, positron emission scanning indicates profound frontal hypometabolism (63). Vestibular Eye Movements Measurements of vestibular eye movements during horizontal rotation, either in darkness, or during fixation of a stationary target, confirms that PSP patients show similar slow-phase responses to normal subjects but quick phases are commonly impaired leading to tonic deviation of the eyes in the contraversive direction in the oribit during rotation in the dark (51). Smooth-Pursuit, Optokinetic, and Vergence Movements Smooth pursuit is usually impaired in both horizontal and vertical planes (21). In the vertical plane, no corrective “catch-up” saccades can be made. The combined impairment of vertical saccades and pursuit constitutes voluntary gaze palsy. During large-field, vertical optokinetic stimulation, PSP patients often show tonic deviation of the eyes in the direction of stripe motion, with small or absent resetting quick phases (11). When PSP patients shift their fixation point between distant and near targets, the vergence movement is slowed compared to control subjects (64). EYE MOVEMENTS IN OTHER DISORDERS CAUSING PARKINSONIAN SYNDROMES: DIFFERENTIATION FROM PSP (TABLE 3) The clinical challenge often posed to neurologists is to diagnose parkinsonian patients with abnormal eye movements. As noted above, most patients with PD have normal eye movements for their age, whereas as most patients with PSP do not. In fact, a number of other parkinsonian disorders have been reported to produce abnormal eye movements, and it is those disorders that we review in this section, noting features that help to differentiate from PSP. 244 Leigh and Zee Table 3 Comparison of Findings in Some Parkinsonian Syndromes SWJ During Fixation PD Increased following pallidotomy Visually Guided Saccades Laboratory Testing of Saccades Hypometric, when self-generated and especially when instructed to generate successive saccades back and forth at a rapid pace; slow vertically in advanced casedes Difficulty generating memorized sequences Advanced cases make errors on antisaccade task Increased errors on antisaccade task PSP Markedly increased Slow; hypometric; initiated with difficulty MSA Increased in some patients Slow and hypometric in some patients CBGD Increased in some patients Hypometric and increased latency; deficit more marked in the presence of a visual background Increased errors on antisaccade task HD May be increased Difficulty with initiation; may be slow and hypometic Markedly increased errors on antisaccade task; impaired predictive saccade tracking Conditions that closely mimic PSP, causing slow vertical saccades, horizontal square-wave jerks, dysphagia, and frequent falls, include multiple infarcts affecting the basal ganglia, internal capsule, and midbrain (in the distribution of the perforating vessels arising from the proximal portions of the posterior cerebral artery) (65), infiltrative processes such as lymphoma, and paraneoplastic syndromes (66). Disorders causing the dorsal midbrain syndrome, such as tumor and hydrocephalus, can also produce a clinical picture that has some similarities to PSP with vertical-gaze palsy. Whipple’s disease can also closely mimic PSP, with vertical saccadic gaze palsy (67,68). In addition, there may be characteristic “oculomasticatory myorhythmia”— a pendular vergence oscillation with concurrent contractions of the masticatory muscles; occasionally the limb muscles also show rhythmic contractions (69). Whipple’s disease can now be diagnosed using polymerase chain reaction (PCR) analysis of involved tissues (70), and can be treated with antibiotics (71). Pure akinesia is characterized by profound disturbances of speech, handwriting, and gait, so that, for example, affected patients may suffer episodes during which they stand “frozen” for hours on end (72). Tremor, limb rigidity, akinesia, dementia, or responsiveness to levodopa are absent. Such patients may show slow and hypometric vertical saccades. The disorder may be a restricted form of PSP with a longer, more benign course. Cortical-basal degeneration (CBD) may lead to a defect in range of vertical eye movements but it usually does not cause marked slowing of saccades; instead the defect is an increased saccadic reaction time (latency), which is evident at the bedside (21,73). Hypometria of upward saccades may occur early in the course, and should be differentiated from restricted upward range, which is present in elderly normal subjects. Other occasional findings in CBD include some decrease in horizontal saccade speed in the direction of the more affected limb, and increased distractibility during the antisaccade paradigm (looking at, instead of way from, the visual target). The other features of this degeneration—focal dystonia, ideomotor apraxia, alien hand syndrome, myoclonus, asymmetric akinetic-rigid syndrome with late onset of gait or balance disturbances—are more important in securing the diagnosis (74,75). Multiple system atrophy (MSA) causes a parkinsonian syndrome with marked autonomic findings. Some patients show slowing of vertical saccades as well as hypometria (21,76), whereas other Role of Ocular Motor Assessment 245 have cerebellar eye movement findings, including downbeat nystagmus during positional testing (77), impaired smooth ocular and eye-head pursuit. Dementia with Lewy bodies, which causes parkinsonism and fluctuating dementia with florid visual hallucinations, may be associated with a vertical-gaze paralysis (78,79), but systematic measurements of vertical saccade are not yet available. Other basal ganglia disorders that have been reported to show features similar to PSP include idiopathic striopallidodentate calcification (Fahr’s disease) (80), and autosomal dominant parkinsonism and dementia with pallido-ponto-nigral degeneration (81). Some patients with Huntington’s disease (HD) may present with vertical saccadic palsy and axial rigidity; this condition is discussed in a later section. Patients with the syndrome of amyotrophic lateral sclerosis (ALS), parkinsonism, and dementia (Lytico-Bodig), which is encountered in the inhabitants of the islands of the South Pacific Ocean, including Guam, may show more severe deficits than those with idiopathic PD, including limitation of vertical gaze (82). A variant of ALS has been described, in which slow vertical saccades, gaze-evoked nystagmus, and impaired pursuit were prominent (83). In the French West Indies, a PSP-like syndrome thought to result from neurotoxic alkaloids is associated with ingestion of herbal teas and fruits (84). Slow saccades, with a supranuclear gaze palsy, are also characteristic of Creutzfeldt–Jakob disease but usually in both the horizontal and vertical planes (85). Periodic alternating nystagmus, rebound nystagmus, and centripetal nystagmus (slow phases directed eccentrically) on lateral gaze are also characteristic of this condition owing to cerebellar involvement (85,86). DRUG-INDUCED PARKINSONISM AND OCULOGYRIC CRISIS Drug intoxications, especially with phenothiazines such as the butyrophenones, may produce a parkinsonian picture with slowing of saccades and an “akinetic mutism” picture. A distinct syndrome is oculogyric crisis, which was once a common feature of postencephalitic parkinsonism, but is now a side effect of drugs, especially neuroleptic agents (87). Oculogyric crises may also rarely be a feature of Wilson’s disease (88), and disorders of amino acid metabolism (aromatic L-amino acid decarboxylase deficiency) (89). A typical oculogyric crisis is ushered in by feelings of fear or depression, which give rise to an obsessive fixation on a thought. The eyes usually deviate upward, and sometimes laterally; they rarely deviate downward. During the period of upward deviation, the movements of the eyes in the upper field of gaze appear nearly normal. Affected patients have great difficulty in looking down, except when they combine a blink and downward saccade. Thus, the ocular disorder may reflect an imbalance of the vertical gaze-holding mechanism (the “neural integrator”). Anticholinergic drugs promptly terminate the thought disorder and ocular deviation, a finding that has led to the suggestion that the disorders of thought and eye movements are linked by a pharmacological imbalance common to both (87). Delayed oculogyric crises have been described after striatocapsular infarction, and with bilateral putaminal hemorrhage (90). Oculogyric crises are distinct from the brief upward ocular deviations that occur in Tourette syndrome (91), Rett syndrome (92), children with benign paroxysmal tonic upgaze (93), and in many patients with tardive dyskinesia (94). In some patients with tardive dyskinesias, however, the upward eye deviations are more sustained and also have the characteristic neuropsychological syndrome of oculogyric crises (95). Episodic brief spells of tonic upgaze have also been reported after bilateral lentiform lesions (96). HUNTINGTON’S DISEASE Clinical Findings HD results from a genetic defect of the IT15 gene (“huntingtin”) on chromosome 4, causing increased CAG triplet repeat length. Disturbances of voluntary gaze are common in this disorder (97–100). Initiation of saccades may be difficult with prolonged latencies, especially when the sac- 246 Leigh and Zee cade is made to command or in anticipation of a target that is moving in a predictable fashion. An obligatory blink or head turn may be used to start the eye moving (101). Saccades may be slow in the horizontal or vertical plane; this deficit can often be detected early in the disease if eye movements are measured, but may not be evident clinically until late in the course. Longitudinal studies of saccades have documented progressive slowing and prolongation of reaction time (102). Saccades may be slower in patients who become symptomatic at an earlier age, and it has been suggested that such individuals are more likely to have inherited the disease from their father (99). Fixation is abnormal in some patients with HD because of saccadic intrusions (100). This defect of steady fixation is particularly evident when patients view a textured background. Smooth pursuit may also be impaired with decreased gain, but often is relatively spared compared with saccades. By contrast, gaze holding and the VOR are spared. Late in the disease, rotational stimulation causes the eyes to tonically deviate with few or no quick phases. Despite the near-ubiquitous finding of abnormal eye movements in HD, some individuals who have been studied at a presymptomatic point in their disease have shown normal eye movements (97,103,104). Thus, routine testing of eye movements cannot be regarded as a reliable method for determining which offspring of affected patients will go on to develop the disease. Some improvement of the eye movement abnormalities in HD has been reported with sulpiride (105). The paradoxical findings of difficulty in initiating voluntary saccades but with an excess of extraneous saccades during attempted fixation has been further elucidated using special test stimuli (Fig. 3). These have revealed an excessive distractibility in, for example, tasks in which patients are required to look in the opposite direction to a suddenly appearing target (antisaccade task) (106). A second finding is that saccades to visual stimuli are made at normal latency, whereas those made to command are delayed. These findings can be related to the parallel pathways that control the various types of saccadic responses. On the one hand, disease affecting either the frontal lobes or the caudate nucleus, which inhibits the SNpr, may lead to difficulties in initiating voluntary saccades in tasks that require learned or predictive behavior (107). On the other hand, HD also affects the SNpr (108). Since this structure inhibits the superior colliculus (nigro-collicular projection), and so suppresses reflexive saccades to visual stimuli, one might expect excessive distractibility during attempted fixation (107). The slowing of saccades might reflect involvement of saccadic burst neurons (109) but at least some pathologic evidence suggests that disturbance of prenuclear inputs, such as the superior colliculus or frontal eye fields, is responsible (110). Disorders to be considered in the differential diagnosis of HD include neuroacanthocytosis (111), although abnormal eye movements have not been described as an important feature of this disorder. Dentatorubropallidoluysian atrophy, also called the Haw River syndrome (112), is another CAG triplet repeat disease (B37, chromosome 12) and is characterized by slow saccades but more myoclonus and ataxia than in HD. OTHER DISORDERS THAT MAY AFFECT THE BASAL GANGLION DISORDERS AND MAY HAVE ABNORMAL EYE MOVEMENTS Wilson’s disease, hepatolenticular degeneration, is an autosomal recessive, inherited disorder of copper metabolism. The defect is in a copper-transporting ATPase with the gene at q14.3 on chromosome 13. CT typically shows hypodense areas, and positron emission tomography (PET) scanning indicates a decreased rate of glucose metabolism in the globus pallidum and putamen. The classic clinical picture is a movement disorder with psychiatric symptoms and associated liver disease. The Kayser–Fleisher ring is typical in the posterior cornea in Descemet’s membrane, and some patients may have a sunflower cataract. Ocular motor disorders in Wilson’s disease include a distractibility of gaze, with inability to voluntarily fix upon an object unless other, competing, visual stimuli are removed (e.g., fixation of a solitary light in an otherwise dark room) (113). Slow vertical saccades have also been reported in one patient with Wilson’s disease (114), but are often normal. A lid- Role of Ocular Motor Assessment 247 opening apraxia has also been noted (115). Oculogyric crises may occur (88). The eye movements of Wilson’s disease, therefore, show some similarities to those described in HD and Alzheimer’s disease. The distractibility in both conditions may be owing to involvement of the inhibitory pathways from the basal ganglia to the superior colliculus (Fig. 2). Ataxia telangiectasia results from a defect on chromosome 11q. Characteristic eye signs include an ocular motor apraxia with hypometria and increased latency, but normal velocity of saccades with head thrusts (116–119). Both vertical and horizontal saccades are affected. Other features are gazeevoked nystagmus, periodic alternating nystagmus, square-wave jerks, and unusual slow smoothpursuit-like movements that are used to change gaze voluntarily when saccades are difficult to generate. α-Feto protein levels are usually dramatically elevated. Niemann–Pick disease (Niemann–Pick type C [2S] disease), usually presents during adolescence with intellectual impairment, ataxia, and dysarthria, and a selective slowing of vertical saccades (120– 122). Other eye movements (including horizontal saccades) are normal. Diagonal saccades may show a curved trajectory evident during the clinical examination. A bone marrow examination shows sea blue histiocytes. Caudate hemorrhage has been associated with ipsilateral gaze preference (123), consistent with experimental dopamine depletion of this structure. Patients with bilateral lentiform nucleus lesions show abnormalities of predictive and memory-guided saccades (both internally generated), but visually guided saccades and antisaccades (both triggered by a visual target) are normal (124). It has been suggested that defects in the control of predictive smooth-pursuit eye movements are a feature of striatal damage (125), consistent with demonstration of pursuit projections to the caudate nucleus (16). Patients with Gilles de la Tourette syndrome may show abnormalities such as blepharospasm and eye tics that include involuntary gaze deviations (91). Routine testing of saccades, fixation, and pursuit is normal, but patients show increased latency and decreased peak velocity of antisaccades, as well as impaired sequencing of memory-guided saccades (126–131). The lid abnormalities of Tourette syndrome must be distinguished from benign eye movement tics, which children often outgrow (132,133). Patients with Lesch–Nyhan syndrome—a disorder of purine metabolism—show an impaired ability to make voluntary saccades, errors on the antisaccade task, blepharospasm, and intermittent gaze deviations similar to Tourette syndrome (134). Patients with essential blepharospasm generally show normal eye movements (135), although saccadic latencies may be increased in certain visually guided and memory-guided saccade tests (136,137). Patients with spasmodic torticollis may show abnormalities of vestibular function including the torsional VOR (138,139). Whether vestibular abnormalities are the cause or a secondary effect of spasmodic torticollis has not been settled, but affected patients do show changes in their perceptions of the visual vertical and straight ahead (140). Patients with tardive dyskinesia may display increased saccade distractibility (141). Patients with active Sydenham’s chorea are reported to show saccadic hypometria (142). Patients with essential tremor, which may sometimes be confused with PD, have eye movement disorders suggestive of cerebellar dysfunction (impaired pursuit and impaired modulation of the duration of vestibular responses by head orientation) (143). PROSPECTS FOR EYE MOVEMENTS IN PARKINSONIAN RESEARCH (TABLE 4) At present, much is known about the neurobiology of eye movements, especially saccades, which can be applied to understanding the pathogenesis of disturbed behavior in a range of movement disorders. It can be expected that the trend of using novel paradigms (such as shown in Fig. 3) along with functional imaging is likely to provide new insights. To the clinical movement disorder specialists, examination of eye movement remains a useful diagnostic tool that will likely become even more important with basic science advances. As more movement disorder specialists incorporate a systematic eye movement examination into their daily routine, not only will diagnostic accuracy 248 Leigh and Zee Table 4 Major Issues for Eye Movement Research in Parkinsonian Syndromes General significance: Eye movements can contribute to a better understanding of the pathogenesis of parkinsonian disorders, and conversely, the study of patients with parkinsonian disorders can contribute to a better understanding of how the brain controls movement in general and eye movements in particular. • • • • • Many functions are accessible to bedside clinic testing. Ease and reliability of eye movement measurement. Eye movements, and the stimuli that drive them, are readily quantified. Important aspects of the neurobiological substrate of eye movements have been defined. Paradigms are readily available that can test brainstem functions as well as the role of eye move ments in prediction, memory, learning, visual search, attention, and reward. Specific issues that can be addressed by eye movement research • • • • • • • • • What is the substrate for frequent saccadic intrusions (square-wave jerks) in PSP and in PD following pallidotomy? What is the pathogenesis of selective slowing of vertical saccades early in the course of PSP, and what accounts for the curved trajectories of saccades? Why do patients with PSP smoothly track a large visual target better than a small one? What is the role of the basal ganglia in generation of pursuit eye movements? Why do PD patients have difficulty generating voluntary saccades between visible targets without an external cue (such as an auditory prompt)? What are the effects of deep brain stimulation on the full range of saccadic and pursuit dynamics? Why do head thrusts and a blinks facilitate the generation of saccades in patients with HD? What is the neurobiological basis for ocular motor tics? What is the role of the basal ganglia in ocular motor learning? increase, but there will be more insights into the pathophysiology of the ocular motor disturbances in parkinsonian disorders and how they respond to treatment. ACKNOWLEDGMENTS Dr. Leigh is supported by the Office of Research and Development, Medical Research Service, Department of Veterans Affairs; NIH grant EY06717; Evenor Armington Fund. Dr. Zee is support by NIH grant EY01849 and the Robert M. and Annetta J. Coffelt endowment for PSP research. VIDEO LEGENDS Video 1: Voluntary saccades in Parkinson’s disease. During the initial part of the clip, the patient is verbally instructed to look between two visual targets (a pen and the camera); some mild hypometria is evident. Subsequently, the patient is instructed to make self-generate saccades between two stationary targets about 60–80° apart; hypometria becomes much more marked, as well as some delayed in initiation. Video 2: Vertical saccades in PSP. The patient is looking between two stationary targets about 40° apart in the vertical plane. The movements are slow, but carry the eyes to their targets. Their trajectories are slightly oblique or curved with a horizontal correction at the end (“round the houses”) (50). Video 3: Horizontal saccades in PSP. The patient is looking between two stationary targets separated about 60° in the horizontal plane. Horizontal saccades are faster than vertical saccades (Video 2), but tend to be hypometric. Role of Ocular Motor Assessment 249 Video 4: Light-induced blink response in a patient with PSP. This was tested by flashing a penlight repetitively into one eye at 1–2 Hz, as he viewed a distant target with both eyes. Unlike normals, or patients with PD, no habituation occurred. REFERENCES 1. Leigh RJ, Zee DS. The neurology of eye movements. New York: Oxford University Press, 1999. 2. Becker W. Metrics. In: Wutz RH, Goldberg ME, eds. The Neurobiology of Saccadic Eye Movements. Amsterdam: Elsevier, 1989: 13–67. 3. Scudder CA, Kaneko CS, Fuchs AF. The brainstem burst generator for saccadic eye movements: a modern synthesis. Exp Brain Res 2002; 142(4):439–462. 4. Chamberlain W. Restriction of upward gaze with advancing age. Am J Ophthalmol 1971;71:341–346. 5. Demer JL. Pivotal role of orbital connective tissues in binocular alignment and strabismus. Invest Ophthalmol Vis Sci 2004;45(3):729–738. 6. Huaman AG, Sharpe JA. Vertical saccades in senescence. Invest Ophthalmol Vis Sci 1993;34:2588–2595. 7. Vidailhet M, Rivaud S, Gouider-Khouja N, Bonnet A, Gaymard B, Agid Y, et al. Eye movements in parkinsonian syndromes. Ann Neurol 1994;35:420–426. 8. Bhidayasiri R, Riley DE, Somers JT, Lerner AJ, Buttner-Ennever JA, Leigh RJ. Pathophysiology of slow vertical saccades in progressive supranuclear palsy. Neurology 2001;57(11):2070–2077. 9. DiScenna AO, Das VE, Zivotofsky AZ, Seidman SH, Leigh RJ. Evaluation of a video tracking device for measurement of horizontal and vertical eye rotations during locomotion. J Neurosci Methods 1995;58:89–94. 10. Lebedev S, Van Gelder P, Tsui WH. Square-root relation between main saccade parameters. Invest Ophthalmol Vis Sci 1996;37:2750–2758. 11. Garbutt S, Riley DE, Kumar AN, Han U, Harwood MR, Leigh RJ. Abnormalities of optokinetic nystagmus in progressive supranuclear palsy, J Neurosurg Psychiatry 2004, in press. 12. Pierrot-Deseilligny C, Ploner CJ, Muri RM, Gaymard B, Rivaud-Pechoux S. Effects of cortical lesions on saccadic: eye movements in humans. Ann N Y Acad Sci 2002;956:216–229. 13. Hikosaka O, Takikawa Y, Kawagoe R. Role of the basal ganglia in the control of purposive saccadic eye movements. Physiol Rev 2000;80(3):953–978. 14. Itoh H, Nakahara H, Hikosaka O, Kawagoe R, Takikawa Y, Aihara K. Correlation of primate caudate neural activity and saccade parameters in reward-oriented behavior. J Neurophysiol 2003;89:1774–1783. 15. Sato M, Hikosaka O. Role of primate substantia nigra pars reticulata in reward-oriented saccadic eye movement. J Neurosci 2002;22(6):2363–2373. 16. Cui D, Yan Y, Lynch J. Pursuit subregion of the frontal eye field projects to the caudate nucleus in monkeys. J Neurophysiol 2003;89:2678–2684. 17. Crawford TJ, Bennett D, Lekwuwa G, Shaunak S, Deakin JF. Cognition and the inhibitory control of saccades in schizophrenia and Parkinson’s disease. Prog Brain Res 2002;140:449–466. 18. Rascol O, Sabatini U, Simonetta-Moreau M, Montastruc JL, Rascol A, Clanet M. Square wave jerks in Parkinsonian syndromes. J Neurol Neurosurg Psychiatry 1991;54:599–602. 19. O’Sullivan JD, Maruff P, Tyler P, Peppard RF, McNeill P, Currie J. Unilateral pallidotomy for Parkinson’s disease disrupts ocular fixation. J Clin Neurosci 2003;10(2):181–185. 20. White OB, Saint-Cyr JA, Tomlinson RD, Sharpe J. Ocular motor deficits in Parkinson’s disease. II: Control of saccadic and smooth pursuit systems. Brain 1983;106:571–587. 21. Rottach KG, Riley DE, DiScenna AO, Zivotofsky AZ, Leigh RJ. Dynamic properties of horizontal and vertical eye movements in parkinsonian syndromes. Ann Neurol 1996;39:368–377. 22. Repka MX, Claro MC, Loupe DN, Reich S. Ocular motility in Parkinson’s disease. Pediatr Ophthalmol Strabismus 1996;33:144–147. 23. Kimmig H, Haussmann K, Mergner T, Lucking CH. What is pathological with gaze shift fragmentation in Parkinson’s disease? J Neurol 2002;249(6):683–692. 24. Crawford T, Goodrich S, Henderson L, Kennard C. Predictive responses in Parkinson’s disease: Manual key presses and saccadic eye movements to regular stimulus events. J Neurol Neurosurg Psychiatry 1989;52:1033–1042. 25. Lueck CJ, Crawford TJ, Henderson L, Van Gisbergen JA, Duysens J, Kennard C. Saccadic eye movements in Parkinson’s disease: II. Remembered saccades - towards a unified hypothesis? Quart J Exp Psychol 1992;45A:211–233. 26. Nakamura T, Bronstein AM, Lueck CJ, Marsden CD, Rudge P. Vestibular, cervical and visual remembered saccades in Parkinson’s disease. Brain 1994;117:1423–1432. 27. Vermersch AI, Rivaud S, Vidailhet M, Bonnet A, Gaymard B, Agid Y, et al. Sequences of memory-guided saccades in Parkinson’s disease. Ann Neurol 1994;35:487–490. 28. Kimmig H, Haussmann K, Mergner T, Lucking CH. What is pathological with gaze shift fragmentation in Parkinson’s disease? J Neurol 2002;249(6):683–692. 250 Leigh and Zee 29. MacAskill MR, Anderson TJ, Jones RD. Saccadic adaptation in neurological disorders. Prog Brain Res 2002;140: 417–431. 30. Bronstein AM, Kennard C. Predictive ocular motor control in Parkinson’s disease. Brain 1985;108:925–940. 31. Ventre J, Zee DS, Papageorgiou H, Reich S. Abnormalities of predictive saccades in hemi-parkinson’s disease. Brain 1992;115:1147–1165. 32. Nenadic I, Gaser C, Volz H, Rammsayer T, Hager F, Sauer H. Processing of temporal information and the basal ganglia: new evidence from fMRI. Exp Brain Res 2003;148:238–246. 33. Turner R, Grafton S, McIntosh A, DeLong M, Hoffman J. The functional anatomy of parkinsonian bradykinesia. Neuroimage 2003;19:163–179. 34. Djamgoz M, Hankins M, Hirano J, Archer S. Neurobiology of retinal dopamine in relation to degenerative states of the tissue. Vision Res 1997;37:3509–3529. 1997. 35. Waterston JA, Barnes GR, Grealy MA, Collins S. Abnormalities of smooth eye and head movement control in Parkinson’s disease. Ann Neurology 1996;39:749–760. 36. Rascol O, Clanet M, Montastruc JL, Simonetta M, Soulier-Esteve MJ, Doyon B, et al. Abnormal ocular movements in Parkinson’s disease. Evidence for involvement of dopaminergic systems. Brain 1989;112:1193–1214. 37. White OW, Saint-Cyr JA, Sharpe JA. Ocular motor deficits in Parkinson’s disease. I. The horizontal vestibulo-ocular reflex and its regulation. Brain 1983;106:555–570. 38. Reichert WH, Doolittle J, McDowell FH. Vestibular dysfunction in Parkinson’s disease. Neurology 1982;32:1133–1138. 39. Gibson JM, Pimlott R, Kennard C. Ocular motor and manual tracking in Parkinson’s disease and the effect of treatment. J Neurol Neurosurg Psychiatry 1987;50:853–860. 40. Blekher T, Siemers E, Abel LA, Yee RD. Eye movements in Parkinson’s disease: before and after pallidotomy. Invest Ophthalmol Vis Sci 2000;41(8):2177–2183. 41. Rivaud-Pechoux S, Vermersch AI, Gaymard B, Ploner CJ, Bejjani BP, Damier P, et al. Improvement of memory guided saccades in parkinsonian patients by high frequency subthalamic nucleus stimulation. J Neurol Neurosurg Psychiatry 2000;68(3):381–384. 42. Carbon M, Ghilardi M, Feigin A, Fukuda M, Silvestri G, Mentis M, et al. Learning networks in health and Parkinson’s disease: reproducibility and treatment effects. Hum Brain Mapp 2003;19:197–211. 43. O’Sullivan JD, Maruff P, Tyler P, Peppard RF, McNeill P, Currie J. Unilateral pallidotomy for Parkinson’s disease disrupts ocular fixation. J Clin Neurosci 2003;10(2):181–185. 44. Averbuch-Heller L, Stahl JS, Hlavin ML, Leigh RJ. Square wave jerks induced by pallidotomy in parkinsonian patients. Neurology 1999;52:185–188. 45. Hotson JR, Langston EB, Langston JW. Saccade responses to dopamine in human MTPT-induced parkinsonism. Ann Neurol 1986;20:456–463. 46. Schultz W, Romo R, Scarnati E, Sundstrom E, Jonsson G, Studer A. Saccadic reaction times, eye-arm coordination and spontaneous eye movements in normal and MTPT-treated monkeys. Exp Brain Res 1989;78:253–267. 47. Brooks BA, Fuchs AF, Finochio D. Saccadic eye movement deficits in the MTPT monkey model of Parkinson’s disease. Brain Res 1986;383:402–407. 48. Nath U, Ben-Shlomo Y, Thomson R, Lees A, Burn D. Clinical features and natural history of progressive supranuclear palsy. A clinical cohort study. Neurology 2003;60:910–916. 49. Davis PH, Bergeron C, McLachlan DR. Atypical presentation of progressive supranuclear palsy. Ann Neurol 1985;17:337–343. 50. Quinn N. The “round the houses” sign in progressive supranuclear palsy. Ann Neurol 2003;40:951. 51. Das V, Leigh R. Visual-vestibular interaction in progressive supranuclear palsy. Vision Res 2000;40:2077–2081. 52. Seemungal B, Faldon M, Revesz T, Lees A, Zee D, Bronstein A. Influence of target size on vertical gaze palsy in a pathologically proven case of progressive supranuclear palsy. Mov Disord 2003;18:818–822. 53. Bhidayasiri R, Riley DE, Somers JT, Lerner AJ, Buttner-Ennever JA, Leigh RJ. Pathophysiology of slow vertical saccades in progressive supranuclear palsy. Neurology 2001;57(11):2070–2077. 54. Mastaglia FL, Grainger KMR. Internuclear ophthalmoplegia in progressive supranuclear palsy. J Neurol Sci 1975;25:303–308. 55. Kitthaweesin K, Riley DE, Leigh RJ. Vergence disorders in progressive supranuclear palsy. Ann N Y Acad Sci 2002;956:504–507. 56. Jenkyn LR, Walsh DB, Walsh BT, Culver CM, Reeves AG. The nuchocephalic reflex. J Neurosurg Psychiatry 1975;38:561–566. 57. Kuniyoshi S, Riley DE, Zee DS, Reich SG, Whitney C, Leigh RJ. Distinguishing progressive supranuclear palsy from other forms of Parkinson’s disease: evaluation of new signs. Ann N Y Acad Sci 2002;956:484–486. 58. Bhidayasiri R, Riley DE, Somers JT, Lerner AJ, Buttner-Ennever JA, Leigh RJ. Pathophysiology of slow vertical saccades in progressive supranuclear palsy. Neurology 2001;57(11):2070–2077. 59. Garbutt S, Harwood M, Kumar A, Han Y, Leigh R. Evaluating small eye movements in patients with saccadic palsies. Ann NY Acad Soc 2003;1004:337–346. Role of Ocular Motor Assessment 251 60. Bhidayasiri R, Plant GT, Leigh RJ. A hypothetical scheme for the brainstem control of vertical gaze. Neurology 2000;54(10):1985–1993. 61. Bhidayasiri R, Riley DE, Somers JT, Lerner AJ, Buttner-Ennever JA, Leigh RJ. Pathophysiology of slow vertical saccades in progressive supranuclear palsy. Neurology 2001;57(11):2070–2077. 62. Pierrot-Deseilligny C, Rivaud S, Fournier E, Agid Y. Lateral visually-guided saccades in progressive supranuclear palsy. Brain 1989;112:471–487. 63. Goffinet AM, DeVolder AG, Gillian C, Rectem D, Bol A, Michel C et al. Positron tomography demonstrates frontal lobe hypometabolism in progressive supranuclear palsy. Ann Neurol 1989;25:131–139. 64. Kitthaweesin K, Riley DE, Leigh RJ. Vergence disorders in progressive supranuclear palsy. Ann N Y Acad Sci 2002;956:504–507. 65. Moses HI, Zee DS. Multi-infarct PSP. Neurology 1987;37:1819. 66. Bhidayasiri R, Plant GT, Leigh RJ. A hypothetical scheme for the brainstem control of vertical gaze. Neurology 2000;54(10):1985–1993. 67. Averbuch-Heller L, Paulson G, Daroff R, Leigh R. Whipple’s disease mimicking progressive supranuclear palsy: the diagnostic value of eye movement recording. J Neurol Neurosurg Psychiatry 1999;66:532–535. 68. Knox DL, Green WR, Troncosa JC, Yardley JH, Hsu J, Zee DS. Cerebral ocular Whipple’s disease: a 62 year-old odyssey from death to diagnosis. Neurology 1995;45:617–-625. 69. Schwartz MA, Selhorst JB, Ochs AL, Beck RW, Campbell WW, Harris JK, et al. Oculomasticatory myorhythmia: a unique movement disorder occurring in Whipple’s disease. Ann Neurol 1986;20:677–683. 70. Lowsky R, Archer GL, Fyles G, Minden M, Curtis J, Messner H, et al. Diagnosis of Whipple’s disease by molecular analysis of peripheral blood. N Engl J Med 1994;331:1343–1346. 71. Fleming JL, Wiesner RH, Shorter RG. Whipple’s disease: clinical, biochemical, and histopathological features and assessment of treatment in 29 patients. Mayo Clin Proc 1988;63:539–551. 72. Riley DE, Fogt N, Leigh RJ. The syndrome of “pure akinesia” and its relationship to progressive supranuclear palsy. Neurology 1994;44:1025–1029. 73. Vidailhet M, Rivaud-Pechoux S. Eye movement disorders in corticobasal degeneration. Adv Neurol 2000;82:161–167. 74. Riley DE, Lang AE, Lewis A, Resch L, Ashby P, Hornykiewicz O et al. Cortical-basal ganglionic degeneration. Neurology 1990;40:1203–1212. 75. Gibb WRG, Luthert PJ, Marsden CD. Corticobasal degeneration. Brain 1989;112:1171–1192. 76. Bhidayasiri R, Riley DE, Somers JT, Lerner AJ, Buttner-Ennever JA, Leigh RJ. Pathophysiology of slow vertical saccades in progressive supranuclear palsy. Neurology 2001;57(11):2070–2077. 77. Bertholon P, Bronstein A, Davies R, Rudge P, Thilo K. Positional down beating nystagmus in 50 patients: cerebellar disorders and possible anterior semicircular canalithiasis. J Neurol Neurosurg Psychiatry 2002;72:366–372. 78. Brett F, Henson C, Staunton H. Familial diffuse Lewy body disease, eye movement abnormalities, and distribution of pathology. Arch Neurol 2003;59:464–467. 79. de Bruin VM, Lees AJ, Daniel SE. Diffuse Lewy body disease presenting with supranuclear gaze palsy, parkinsonism, and dementia: a case report. Mov Disord 1992;7:355–358. 80. Saver JL, Liu GT, Charness ME. Idiopathic striopallidodentate calcification with prominent supranuclear abnormality of eye movement. J Neuro-ophthalmology 1994;14:29–33. 81. Wszolek ZK, Pfeiffer RF, Bhatt MH, Schelper RL, Cordes M, Snow BJ, et al. Rapidly progressive autosomal dominant parkinsonism and dementia with pallido-ponto-nigral degeneration. Ann Neurol 1992;32:312–320. 82. Lepore FE, Steele JC, Cox TA, Tillson G, Calne DB, Duvoisin RC, et al. Supranuclear disturbances of ocular motility in Lytico-Bodig. Neurology 1988;38:1849–1853. 83. Averbuch-Heller L, Helmchen C, Horn AKE, Leigh RJ, Büttner-Ennever JA. Slow vertical saccades in motor neuron disease: correlation of structure and function. Ann Neurol 1998;44:641–648. 84. Caparros-Lefebvre D, Sergeant N, Lees A, Camuzat A, Daniel S, Lannuzel A, et al. Guadeloupean parkinsonism: a cluster of progressive supranuclear palsy-like tauopathy. Brain 2002;125:801–811. 85. Grant MP, Cohen M, Petersen RB, Halmagyi GM, McDougall A, Tusa RJ, et al. Abnormal eye movements in Creutzfeldt–Jakob disease. Ann Neurology 1993;34:192–197. 86. Helmchen C, Büttner U. Centripetal nystagmus in a case of Creutzfeldt–Jakob disease. Neuro-ophthalmology 1995;15:187–192. 87. Leigh RJ, Foley JM, Remler BF, Civil RH. Oculogyric crisis: a syndrome of thought disorder and ocular deviation. Ann Neurol 1987;22:13–17. 88. Lees A, Kim Y, Lyoo C. Oculogyric crisis as an initial manifestation of Wilson’s disease. Neurology 1999;52:1714–1715. 89. Swoboda K, Hyland K, Goldstein D, Kuban K, Arnold L, Holmes C, et al. Clinical and therapeutic observations in aromatic L-amino decarboxylase deficiency. Neurology 1999;53:1205–1211. 90. Liu GT, Carrazana EJ, Macklis JD, Mikati MA. Delayed oculogyric crises associated with striatocapsular infarction. J Clin Neuro-ophthalmol 1991;11:198–201. 252 Leigh and Zee 91. Frankel M, Cummings JL. Neuro-ophthalmic abnormalities in Tourette’s syndrome. Functional and anatomical implications. Neurology 1984;34:359–361. 92. FitzGerald PM, Jankovic J, Glaze DG, Schultz R, Percy AK. Extrapyramidal involvement in Rett’s syndrome. Neurology 1990;40:293–295. 93. Hoyt CS, Mousel DK. Transient supranuclear disturbances of gaze in healthy neonates. Am J Ophthalmol 1980;89: 708–713. 94. FitzGerald PM, Jankovic J. Tardive oculogyric crisis. Neurology 1989;39:1434–1437. 95. Sachdev P. Tardive and chronically recurrent oculogyric crises. Mov Disord 1993;8:93–97. 96. Kim JS, Kim HK, Im JH, Lee MC. Oculogryic crisis and abnormal magnetic resonance imaging signals in bilateral lentiform nuclei. Mov Disord 1996;11:756–758. 97. Collewijn H, Went LN, Tamminga EP, Vegter-Van der Vlis M. Oculomotor defects in patients with Huntington’s disease and their offspring. J Neurol Sci 1988;86:307–320. 98. Lasker AG, Zee DS. Ocular motor abnormalities in Huntington’s disease. Vision Res 1997;37:3639-3645. 99. Lasker AG, Zee DS, Hain TC, Folstein SE, Singer HS. Saccades in Huntington’s disease: initiation defects and distractability. Neurology 1987;37:364–370. 100. Leigh RJ, Newman SA, Folstein SE, Lasker AG, Jensen BA. Abnormal ocular motor control in Huntington’s disease. Neurology 1983;33:1268–1275. 101. Zangemeister WH, Mueller-Jensen A. The coordination of gaze movements in Huntington’s disease. Neuro-ophthalmology 1985;5:193–206. 102. Rubin AJ, King WM, Reinbold KA, Shoulson I. Quantitative longitudinal assessment of saccades in Huntington’s disease. J Clin Neuro-opthalmol 1993;13:59–66. 103. Kirkwood SC, Siemers E, Bond C, Conneally PM, Christian JC, Foroud T. Confirmation of subtle motor changes among presymptomatic carriers of the Huntington disease gene. Arch Neurol 2000;57(7):1040–1044. 104. Rothlind JC, Brandt J, Zee D, Codori AM, Folstein S. Verbal memory and oculomotor control are unimpaired in asymptomatic adults with the genetic marker for Huntington’s disease. Arch Neurol 1993;50:799–802. 105. Reveley MA, Dursun SM, Andrews H. Improvement of abnormal saccadic eye movements in Huntington’s disease by sulpiride: a case study. Journal of Psychopharmacology 1994;8:262–265. 106. Lasker AG, Zee DS, Hain TC, Folstein SE, Singer HS. Saccades in Huntington’s disease: initiation defects and distractibility. Neurology 1987;37:364–370. 107. Hikosaka O, Takikawa Y, Kawagoe R. Role of the basal ganglia in the control of purposive saccadic eye movements. Physiol Rev 2000;80(3):953–978. 108. Oyanagi K, Takeda S, Takahashi H, Ohama E, Ikuta F. A quantitative investigation of the substantia nigra in Huntington’s disease. Ann Neurol 1989;26:13–19. 109. Koeppen AH. The nucleus pontis centralis caudalis in Huntington’s disease. J Neurol Sci 1989;91:129–141. 110. Leigh RJ, Parhad IM, Clark AW, Buettner-Ennever JA, Folstein SE. Brainstem findings in Huntington’s disease. J Neurol Sci 1985;71:247–256. 111. Rinne JO, Daniel SE, Scaravilli F, Pires M, Harding AE, Marsden CD. The neuropathological features of neuroacanthocytosis. Mov Disord 1994;9:297–304. 112. Burke JR, Wingfield MS, Lewis KE, Roses AD, Lee JE, Hulette C, et al. The haw river syndrome: dentatorubropallidoluysian atrophy (DRPLA) in an African-American family. Nat Genet 1994;7:521–524. 113. Lennox G, Jones R. Gaze distractibility in Wilson’s disease. Ann Neurol 1989;25:415–417. 114. Kirkham TH, Kamin DF. Slow saccadic eye movements in Wilson’s disease. J Neurol Neurosurg Psychiatry 1974;37:191–194. 115. Keane JR. Lid-opening apraxia in Wilson’s disease. J Clin Neuro-ophthalmol 1988;8:31–33. 116. Lewis RF. Ocular motor apraxia and ataxia-telangiectasia. Arch Neurol 2001;58(8):1312. 117. Lewis RF, Crawford TO. Ocular motor abnormalities in ataxia telangiectasia. Neurology 1998;50(Suppl). 118. Lewis RF, Crawford TO. Slow target-directed eye movements in ataxia-telangiectasia. Invest Ophthalmol Vis Sci 2002;43(3):686–691. 119. Stell R, Bronstein AM, Plant GT, Harding AE. Ataxia telangiectasia: a reappraisal of the ocular motor features and their value in the diagnosis of atypical cases. Mov Disord 1989;4:320–329. 120. Rottach KG, von Maydell RD, Das VE, Zivotofsky AZ, DiScenna AO, Gordon JL, et al. Evidence for independent feedback control of horizontal and vertical saccades from Niemann–Pick type C disease. Vision Res 1997;37:3627–3638. 121. Garbutt S, Harris CM. Abnormal vertical optokinetic nystagmus in infants and children. Br J Ophthalmol 2000;84(5):451–455. 122. Higgins JJ, Patterson MC, Dambrosia JM, Pikus AT, Pentchev PG, Sato S, et al. A clinical staging classification for type C Niemann–Pick disease. Neurology 1992;42:2286–2290. 123. Stein RW, Kase CS, Hier DB, Caplan LR, Mohr JP. Caudate hemorrhage. Neurology 1984;34:1549–1554. 124. Vermersch AI, RM M, Rivaud S, Vidailhet M, Gaymard B, Agid Y, et al. Saccade disturbances after bilateral lentiform nucleus lesions in humans. J Neurol Neurosurg Psychiatry 1996;60:179–184. Role of Ocular Motor Assessment 253 125. Lekwuwa GU, Barnes GR. Cerebral control of eye movements. II. Timing of anticipatory eye movements, predictive pursuit and phase errors in focal cerebral lesions. Brain 1996;119:491–505. 126. Dursun SM, Burke JG, Reveley MA. Antisaccade eye movement abnormalities in Tourette syndrome: evidence for cortico-striatal network dysfunction? J Psychopharmacol 2000;14(1):37–39. 127. LeVasseur AL, Flanagan JR, Riopelle RJ, Munoz DP. Control of volitional and reflexive saccades in Tourette’s syndrome. Brain 2001;124(Pt 10):2045–2058. 128. Mostofsky SH, Lasker AG, Singer HS, Denckla MB, Zee DS. Oculomotor abnormalities in boys with Tourette syndrome with and without ADHD. J Am Acad Child Adolesc Psychiatry 2001;40(12):1464–1472. 129. Munoz DP, Le Vasseur AL, Flanagan JR. Control of volitional and reflexive saccades in Tourette’s syndrome. Prog Brain Res 2002;140:467–481. 130. Narita AS, Shawkat FS, Lask B, Taylor DS, Harris CM. Eye movement abnormalities in a case of Tourette syndrome. Dev Med Child Neurol 1997;39:270–273. 131. Straube A, Mennicken J-B, Riedel M, Eggert T, Müller N. Saccades in Gilles de la Tourette’s syndrome. Movement Disorders 1997;12:536–546. 132. Binyon S, Prendergast M. Eye-movement tics in children. Dev Med Child Neurol 1991;33:343–355. 133. Shawkat FS, Harris CM, Jacobs M, Taylor D, Brett EM. Eye movement tics. Brit J Ophthalmol 1992;76:697–699. 134. Jinnah HA, Lewis RF, Visser JE, Eddey GE, Barabas G, Harris JC. Ocular motor dysfunction in Lesch–Nyhan disease. Pediatr Neurol 2001;24(3):200–204. 135. Demer JL, Holds JB, Hovis LA. Ocular movements in essential blepharospasm. Am J Ophthalmol 1990;110:674–682. 136. Aramideh M, Bour LJ, Koelman JHTM, Speelman JD, Ongerboer de Visser BW. Abnormal eye movements in blepharospasm and involuntary levator palpebrae inhibition. Brain 1994;117:1457–1474. 137. Bollen E, Van Exel E, van der Velde EA, Buytels P, Bastiaanse J, van Dijk JG. Saccadic eye movements in idiopathic blepharospasm. Movement Disorders 1996;11:678–682. 138. Averbuch-Heller L, Rottach KG, Zivotofsky AZ, Suarez JI, Pettee AD, Remler BF et al. Torsional eye movements in patients with skew deviation and spasmodic torticollis: responses to static and dynamic head roll. Neurology 1997;48:506–514. 139. Stell R, Bronstein AM, Marsden CD. Vestibulo-ocular abnormalites in spasmodic torticollis before and after botulinum toxin injections. J Neurol Neurosurg Psychiatry 1989;52:57–62. 140. Anastasopoulos D, Nasios G, Psilas K, Mergner T, Maurer C, Lücking C-H. What is straight ahead to a patient with torticollis? Brain 1998;121:91–101. 141. Thaker GK, Nguyen JA, Tamminga CA. Increased saccadic distractibility in tardive dyskinesia: functional evidence for subcortical GABA dysfunction. Biol Psychiatry 1989;25:49–59. 142. Cardosa F, Eduardo C, Silva AP, Mota CCC. Chorea in fifty consecutive patients with rheumatic fever. Mov Disord 1997;12:701–703. 143. Helmchen C, Hagenow A, Miesner J, Sprenger A, Rambold H, Wenzelburger R et al. Eye movement abnormalities in essential tremor may indicate cerebellar dysfunction. Brain 2003;126:1319–1392.