12

Added Value of the Neuropsychological Evaluation 185
12
Added Value of the Neuropsychological Evaluation for Diagnosis and Research of Atypical Parkinsonian
Disorders
Bruno Dubois and Bernard Pillon
INTRODUCTION
Diseases with movement disorders may be difficult to diagnose, both at the onset when motor symptoms are mild and not sufficiently specific (e.g., difficulty in manipulating objects), or at the end stage when distinctive motor signs are diluted into a severe and polymorphous clinical picture
(e.g., gait disorder with postural instability and cognitive decline in aged patients). Erroneous diagnoses are frequent (1,2) , even in the most common idiopathic Parkinson’s disease (PD) (3) . Some of these errors may be avoided if the cognitive dysfunctions that often accompany these diseases are included in the diagnostic criteria.
Subtle but specific cognitive deficits can frequently be detected in patients with a variety of diseases accompanied by movement disorders. We used to say “except for essential tremor” but some cognitive changes have recently been reported even in this case (4) . This is explained by the fact that the neuronal pathways connecting the basal ganglia to the cortex project not only to regions involved in the control of movements (motor, premotor, supplementary motor areas) but also to cortical areas contributing to cognitive functions (prefrontal cortex) and to emotional-processing behavior (cingulum and orbitofrontal cortex). In each of these diseases, the loss of different specific populations of neurons in the basal ganglia produces not only a characteristic motor syndrome, but also a recognizable pattern of neuropsychological deficits. Why not include these cognitive and behavioral changes in diagnosis decision trees? Indeed, the use of appropriate neuropsychological tests or questionnaires to detect these deficits can contribute to the diagnosis of such diseases (Table 1).
In this review, we will (1) present the different types of deficits that can be usually encountered following lesions of the basal ganglia; (2) characterize the neuropsychological pattern of the main movement disorders: idiopathic PD, multiple system atrophy (MSA), progressive supranuclear palsy
(PSP), corticobasal degeneration (CBD), and dementia with Lewy bodies (DLB); and (3) show that the contribution of neuropsychological deficits to diagnosis varies from one parkinsonian disorder to another.
From: Current Clinical Neurology: Atypical Parkinsonian Disorders
Edited by: I. Litvan © Humana Press Inc., Totowa, NJ
185
186 Dubois and Pillon
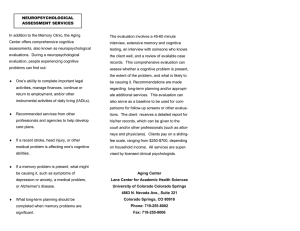
Table 1
Proposed Neuropsychological Battery to Evaluate Cognitive and Behavioral Deficits in Parkinsonian Disorders
Domain of Investigation Proposed Tool
Global cognitive efficiency
Global executive syndrome
Set elaboration and monitoring
Set maintenance
Set shifting
Inhibition of interferences
Motor programming
Mattis Dementia Rating Scale (5)
Frontal Assessment Battery (6)
Wisconsin Card Sorting Test (7)
Lexical fluency (8)
Trail Making Test (9)
Stroop Test (10)
Graphic and motor series (11)
Resistance to environmental dependency Imitation, prehension, utilization (12)
Strategic components of memory California Verbal Learning Test (13)
Opposition between free and cued recall Grober and Buschke Test (14)
Linguistic functions Boston Diagnostic Aphasia Examination (15)
Gestures
Emotional behavior
Apraxia examination (16)
Neuropsychiatric Inventory (17)
WHAT ARE THE COGNITIVE AND BEHAVIORAL CHANGES CURRENTLY
ENCOUNTERED IN PARKINSONIAN DISORDERS?
The neuropsychological picture of patients may vary from subtle behavioral abnormalities to florid dementia with delusions and hallucinations. The nature and severity of cognitive disorders, the type of impaired memory processes, the presence or absence of instrumental deficits, the precocity of the dysexecutive syndrome, and the frequency of behavioral disorders depend on the underlying neuronal lesions.
Dementia
According to DSM-IV ( Diagnostic and Statistical Manual of Mental Disorders , 4th ed.) criteria
(18) , dementia is defined by the development of multiple cognitive deficits, severe enough to interfere with social activity or personal relationships and representing a decline from a previously higher level of functioning. The term dementia needs to be used with caution in diseases in which motor impairment, mood, and behavioral disorders may be part of the clinical picture. In these patients the loss of intellectual capacities can, however, be evaluated by psychometric criteria, using global scales, such as the Mattis Dementia Rating Scale (5) , which is more appropriate than the Mini Mental State
Exam for predominantly subcortical degenerative diseases, given the inclusion of tests evaluating attention and executive functions. Such tools provide cutoff scores that permit a psychometric distinction between demented and nondemented patients. Dementia is usually not observed in PD with early onset (19) or in the early stages of PD (20) or MSA (21,22) . Dementia may occur in patients with late-onset PD (23) , PSP (24,25) , or CBD (26) . It is a major feature of DLB, although there may be fluctuations of intellectual functioning from one day to another (27) .
Memory
Learning disorders in neurodegenerative diseases may be assessed by tools, such as the California
Verbal Learning Test (13) or the Grober and Buschke Test (14) that make it possible to analyze specific memory processes and distinguish between storage and retrieval difficulties. The key for understanding the relationship between memory disorders and degenerative diseases implicates the functional “mediotemporal vs frontal dissociation.” Encoding deficits, loss of information after a delay, low effect of cuing on recall, high number of extralist intrusions, and false positives in recog-
Added Value of the Neuropsychological Evaluation 187
nition characterize diseases associated with lesion of hippocampal and perihippocampal areas such as Alzheimer’s disease (AD) (28) . By contrast, predominant retrieval deficits, manifested by the opposition between impaired free recall and correct cued recall and recognition, are present in diseases associated with dysfunction of striatofrontal neuronal circuits such as PSP or PD with dementia
(PDD) (29) . Milder deficient activation of the frontal component of memory processes occurs in PD
(30,31) , MSA (22) , and CBD (32,33) . Little has been published on learning disorders in DLB, but a study with autopsy-confirmed cases show that they are less severe than in AD (34) . Clinical evidence suggests that although cued recall is less efficient in DLB than in PD or PSP, it is better preserved than in AD. A similar contrast between a true loss of information in AD and retrieval deficits in PDD also applies to retrograde amnesia.
Instrumental Activities
Instrumental dysfunction, suggestive of temporoparietal lesions, include aphasia, apraxia, and visuospatial deficits. Aphasia and apraxia may be investigated by clinical batteries, such as the Boston Diagnostic Aphasia Examination (15) or the Heilman and Gonzalez Rothi battery for apraxia
(16) . Visuospatial deficits are less clearly defined and do not allow the differential diagnosis of the different diseases, since various cognitive abilities, such as visuospatial perception, drawing, or constructive aptitude, and conceptual thinking may affect performance (35) . Impairment of instrumental activities is specific to neurodegenerative diseases with a cortical involvement. Aphasia may be observed in DLB (27) , whereas apraxia is more characteristic of CBD (32,36) . In contrast, instrumental functions are mildly disturbed in PSP (37) and PDD (38) and are preserved in PD (39) and MSA (22) .
Executive Functions
Executive functions , namely the mental processes involved in behavioral planning, particularly when the environment requires adaptation to a new situation, are under the control of striatofrontal circuits. These functions may be investigated at the patient’s bedside (6) ( see video) or by a neuropsychological evaluation assessing the main processes mediated by striatofrontal loops such as set elaboration, set maintenance, and set shifting, inhibition of interferences, motor programming, and environmental autonomy (Table 1). These functions are impaired at an early stage of all parkinsonian disorders, but are much less severe in PD and MSA than in the other parkinsonian syndromes (25,40) .
Behavioral Disorders
Delusions and hallucinations, as diagnosed in accordance with the DSM–IV criteria (18) , are common at early stages of DLB (27) . They occur in PD, particularly in demented patients or as a result of treatment with anticholinergic or dopaminergic drugs, but are not characteristic of MSA, PSP, or
CBD (41) . Apathy and disinhibition may also be observed in parkinsonian disorders (42) . Apathy has been defined as a lack of motivation and responsiveness to both positive and negative events in the absence of emotional distress or negative thoughts. It can be distinguished from depression using new scales, such as the Neuropsychiatric Inventory (17) . Apathy is particularly frequent in PSP
(43) and DLB (44) , whereas irritability predominates in CBD (45) and depression in PD (44) ( see
Chapter 11).
WHICH NEUROPSYCHOLOGICAL PATTERN CHARACTERIZES EACH
OF THE MAIN PARKINSONIAN DISORDERS?
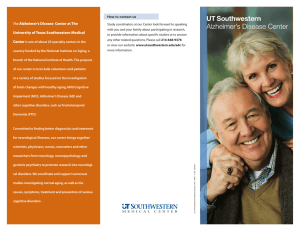
Well-characterized neuropsychological profiles can be drawn from the clustering of the cognitive and behavioral characteristics found in each parkinsonian disorder (Table 2). The absence of marked cognitive or behavioral changes makes more probable the diagnosis of PD or MSA, whereas a severe dysexecutive syndrome suggestive of a striatofrontal dysfunction reinforces the diagnosis of PSP and specific deficits related to a cortical involvement contribute to the diagnosis of CBD or DLB.
188 Dubois and Pillon
Table 2
Neuropsychological Pattern of Each Disease
PD MSA PSP
Dementia
Mattis DRS (144)
Fluctuations
Dysexecutive syndrome
FAB (18)
Envt Dependency
Memory deficits
Free recall (48)
Total recall (48)
Instrumental deficits
Language
Gesture
Psychosis
-
-
-
-
>130
16
±
25
46
-
14
22
46
-
-
-
>130
±
-
11
16
44
-
<130
++
±
±
PDD
<130
+
11
+
12
42
±
±
+
-
-
CBD
<130
11
±
19
42
+
++
DLB
<130
+
11
+
10
34
+
±
++
Mean indicative values adapted from refs. 6 , 22 , 29 , 32 , 52 .
, absent; ±, mild or discussed; +, moderate or present in a proportion of patients;
++, severe and present in a majority of patients.
Parkinson’s Disease
Cognitive changes in the majority of patients with PD are subtle and mainly restricted to attentional and retrieval deficits. It is only by using appropriate neuropsychological tests that these cognitive changes can be detected. They mainly concern (a) the visuospatial domain, observed in visuospatial paradigms that require self-elaboration of the response or forward-planning capacity; (b) memory, that is, working memory and long-term memory, especially in tasks that involve self-organization of the to-be-remembered material, temporal ordering and conditional associative learning, and procedural learning; and (c) executive functions, namely concept formation and problem solving, setmaintenance and set-shifting (for a review, see ref. 46 ).
Mood and behavioral changes are also described in PD. Depression is encountered in about 30% of patients and has been the focus of a large number of studies (47) . It is important to diagnose it because depression induces attention and memory disorders and, if sufficiently severe, impairs cognitive functions especially those of the executive system in relation to a significant decrease in frontal metabolism evidenced on positron emission tomography (PET) scan studies. More recently, attention has been drawn to apathy and its relation to basal ganglia disorders. Apathy is not infrequent in PD and has repercussions on cognitive functions, affect, and behavior (48,49) .
Unlike depression, anxiety symptoms almost always begin after the onset of the motor symptoms and are related to medication-induced on–off fluctuations and wearing-off condition in most of the cases. Drug-induced psychiatric disorders are frequently found in PD and mainly consist of hallucinations and delusions. These disorders are, however, much more frequent in PDD or DLB (44) .
To conclude, the clinical diagnosis of PD relies on the evidence of a parkinsonian syndrome responsive to levodopa in the absence of severe intellectual or memory dysfunction. This is the rule, at least, in the young-onset form of the disease. In the late-onset one, however, a subcorticofrontal dementia may occur after several years of evolution, which may result from the compounding effect of diseaserelated neuronal lesions and age-related neuronal changes (50) . PDD is characterized by a marked dysexecutive syndrome, accompanied by a severe amnesic syndrome with a persistent response to cuing, in the absence of true aphasia, apraxia, or agnosia, and may be difficult to diagnose. DSM–IV criteria of dementia (18) are well suited to AD, but less appropriate for PD because the severe motor
Added Value of the Neuropsychological Evaluation 189
deficits may themselves affect patient’s autonomy. Moreover, an overestimation of the severity of cognitive impairment may result from nonspecific factors (akinesia, hypophonia, depression, anxiety, marked cognitive slowing with delay in responses, uncontrolled dyskinesias) that interfere with the evaluation of cognitive functions.
Multiple System Atrophy
Cognitive changes are mild in the parkinsonian variant of MSA (MSA-P, previously called striatonigral degeneration), at least in the early stage of the disease, before patients reach a severe akinetic state with dysarthria, which may affect the cognitive evaluation. The few studies of cognition in MSA, including the MSA-P variant, display few differences from the neuropsychological pattern of PD: some more severe deficits in the Stroop test (51) or in verbal fluency (52) . In our experience, neuropsychological testing does not help to distinguish between the two disorders. In contrast, when faced to an axial parkinsonian syndrome poorly responsive to levodopa, the absence of a severe subcorticofrontal syndrome strongly favors the diagnosis of MSA-P and decreases the probability for PSP (22,53) .
Psychiatric disorders have been poorly studied in MSA-P. Depression, anxiety, and emotional lability have been described, but not psychosis (54) .
Progressive Supranuclear Palsy
Cognitive and behavioral changes are consistent even in the early stages of the disease. Cognitive slowing and inertia occur in the first year in 52% of cases. As the disease progresses, these changes progressively worsen. From 24 patients who underwent two or more neuropsychological evaluations over time, 38% showed a global impairment at their first examination, and 70% 15 mo later. The changes may become severe enough to warrant the diagnosis of dementia, but the deficits still conform to the pattern of subcorticofrontal dementia. The dysexecutive syndrome of PSP is much more severe than that observed in any other subcortical disorders, and the memory deficit is dramatically improved in conditions that facilitate retrieval processing such as cueing and recognition.
Cognitive slowing appears evident in patients with PSP, who answer questions and solve even the simplest problems with delay. It is a genuine slowing of central-processing time unrelated to motor or affective disorders, as demonstrated experimentally using reaction time tasks (55) and event-related brain potentials (56) .
Cognitive slowing may contribute to decreased lexical fluency that is more severely impaired in patients with PSP than in patients with PD or AD, although naming is more affected in the latter (25) .
The deficit is observed in different types of fluency, including semantic fluency, where patients have to list animal names or objects that can be found in a supermarket, phonemic fluency, where patients are required to produce words beginning with a given letter, and design fluency, where patients must produce abstract designs (57) .
A tendency to perseverate may also account for some of the deficits, particularly in tasks involving concept formation and shifting ability. In the Wisconsin Card Sorting Test, PSP patients complete a smaller number of categories than patients with PD or MSA-P. This lack of flexibility affects both categorical and motor sequencing, as shown by the poor performance of patients with PSP in the
Trail Making Test and in the motor series of Luria. Patients with PSP also experience difficulty in conceptualization and problem-solving ability, which may account for their poor performance in similarities, interpretation of proverbs, comprehension of abstract concepts, arithmetic and lineage problems, tower tasks, and picture arrangement.
This severe dysexecutive syndrome contributes to the memory deficits and instrumental disorders observed in PSP. Short-term memory was found to be impaired using the Brown–Peterson paradigm, a working memory task in which the patients were more sensitive than controls to interference. Longterm memory is also disturbed in PSP, as shown by immediate and delayed recall of the subtests of
190 Dubois and Pillon
the Wechsler Memory Scale, the Rey Auditory Verbal Learning Test, and the California Verbal
Learning Test. However, when encoding is controlled by using semantic category cues and when recall is performed with the same cues, as in the Grober and Buschke procedure, recall performance of the patients dramatically improves, confirming that there is no genuine amnesia in the disease (29) .
Various speech disorders have been described in PSP. A severe reduction of spontaneous speech resembling dynamic aphasia is usually observed (58) , but abnormal loquacity has also been reported.
Word-finding difficulty may occur, but it is generally less severe than in AD patients. Semantic or syntactic comprehension disorders are absent or mild. Dynamic apraxia may be found (32) . Bilateral apraxic errors for transitive and intransitive movements have been reported, but they are much less severe than in CBD (59) . Visual and auditory perception may be disturbed, but there is no evidence of object agnosia or alexia. Therefore, instrumental disorders of patients with PSP, when present, are rather considered to be a consequence of impaired executive and perceptual-motor functions or attentional disorders.
Besides cognitive impairment, patients with PSP exhibit behavioral disorders. They show severe difficulty in self-guided behavior and are abnormally dependent on stimuli from the environment.
They involuntarily grasp all the objects presented in front of them; they imitate the examiner’s gestures passively and use objects in the absence of any explicit verbal orders (25) . Such uncontrolled behaviors are never observed in normal control subjects in the absence of explicit demands and are considered to result from a lack of the inhibitory control normally exerted by the frontal lobes (12) .
PSP patients also have difficulty in inhibiting an automatic motor program once it is initiated. This can easily be evaluated with the “signe de l’applaudissement” [“clapping sign”] (60) : when asked to clap their hands three times consecutively, as quickly as possible, these patients have a tendency to clap more (four or five times), sometimes initiating an automatic program of clapping that they are unable to stop, as if they had difficulty in programming voluntary acts that compete with overlearned motor skills. This sign seems to be specific to striatal dysfunction occurring in PSP (61) . Changes in mood, emotion, and personality have also been described: most frequently bluntness of affective expression and lack of concern about personal behavior or the behavior of others, but sometimes obsessive disorders or disinhibition with bulimia, inappropriate sexual behavior, or aggressiveness.
These changes are difficult to investigate, given the lack of insight and the transient nature of the emotions expressed. The testimony of caregivers is therefore required. Administering the Neuropsychiatric Inventory (NPI) to patients’ informants showed that patients with PSP exhibited apathy almost as a rule, since it was observed in 91% of the cases (43) . Apathy was more frequent in PSP than in any other parkinsonian syndrome.
Corticobasal Degeneration
The cognitive profile of this disease is distinct from that of PSP, because of the presence of signs suggestive of cortical involvement. Many patients present only limb clumsiness and gesture disorders at the first examination, without any—or with few—cognitive or behavioral symptoms (26) . In contrast, the disease may begin by other signs of cortical involvement, particularly nonfluent progressive aphasia (62) . Finally, a severe frontal cognitive and behavioral syndrome may initiate the disease in some patients (63) .
CBD is typically defined by unilateral rigidity of one arm with apraxic features, accounting for the proposition of the new term “progressive asymmetric rigidity and apraxia syndrome” (64) . Gesture disorders are so characteristic of the disease that the diagnosis can be suspected on the simple analysis of the motor disturbances. They consist, at first, of the patient experiencing difficulty or showing perplexity in the performance of delicate and fine movements of the fingers of one hand. At this stage, patients complain of clumsiness and loss of manual dexterity, reminiscent of “limb apraxia,” variously described as “kinesthetic” in patients with lesions of the parietal cortex, or “kinetic” in
Added Value of the Neuropsychological Evaluation 191
patients with lesions of the premotor cortex. Systematic evaluation shows disorders of dynamic motor execution (impaired bimanual coordination, temporal organization, control, and inhibition) (32) . Asymmetric praxis disorders (difficulty in posture imitation, symbolic gesture execution, and object utilization) are also regularly observed, even at this stage. Ideomotor apraxia is frequent, especially in patients who have initial symptoms in the right limb, in agreement with the hypothesis of a predominant storage of “movement formulae” in the left hemisphere (65) . In addition, central deficits in action knowledge and mechanical problem solving have been linked to parietal lobe pathology (66) .
“Alien limb phenomenon,” in which a limb behaves in an uncooperative or foreign way, has been attributed to lesions affecting the supplementary motor area. Its occurrence, in the absence of a known callosal lesion, would be highly suggestive of the diagnosis of CBD.
Other signs of cortical involvement have been observed in CBD. Linguistic disturbances are found, consisting of word-finding difficulties, decreased lexical fluency, transcortical motor aphasia, or progressive phonetic disintegration (67) . These deficits resembling primary progressive nonfluent aphasia can even be an initial symptom of CBD. Neglect and visuospatial deficits have also been reported.
Constructive apraxia is observed in patients with predominant right-hemisphere lesions, in relation with the well-known influence of this hemisphere on visuospatial function.
Other cognitive changes resemble the subcorticofrontal dysfunction of PSP: a dysexecutive syndrome and a learning deficit that can be alleviated by semantic cuing (32) . The environmental dependency syndrome, thought to be related to a release of the inhibition normally exerted by the frontal lobes on the activity of the parietal lobes (12) , is less frequent, however, in CBD than in PSP, probably because of the parietal lobe dysfunction in this disease. Early subcorticofrontal syndrome in
CBD would predict a shorter survival.
In most of the clinical studies performed on CBD patients, the level of intellectual deterioration was mild or moderate until an advanced stage of the disease. In some cases, however, patients with a severe dysexecutive syndrome associated with memory disorders and impaired instrumental activities may reach the threshold of dementia in which both cortical and subcorticofrontal components play a role. Thus, dementia is not infrequent in CBD and may even be observed from the onset in unusual clinical presentation. In 10 out of 13 cases with pathologically proven CBD, dementia was noticed within 3 yr of onset of symptoms (68) .
Besides frontal lobe–type behavioral alterations, patients with CBD may present neuropsychiatric disorders. In a series of CBD patients, the NPI showed that depression, apathy, irritability, and agitation were the symptoms most commonly exhibited (45) . The depression and irritability of patients with CBD were more frequent and severe than those of patients with PSP, whereas patients with PSP exhibited more apathy.
Dementia With Lewy Bodies
The diagnosis of DLB can be suspected clinically on the basis of the early occurrence of a cognitive decline resembling a chronic confusional state with fluctuating cognitive signs and visual and/or auditive hallucinations in a patient with mild parkinsonism (69) . The rapidly progressive dementia is accompanied by aphasia, dyspraxia, or spatial disorientation, suggestive of temporoparietal dysfunction. The neuropsychological profile differs from that of patients with AD: cognitive deficits are more acute, attentional fluctuations more intense, and psychotic features appear earlier. Moreover, patients with DLB present a more severe dysexecutive impairment but less severe memory deficits than patients with AD (34) . The neuropsychological pattern of DLB can also be distinguished from the subcortical dementia of PD on the basis of the early occurrence of cognitive deficits and psychotic features, and the presence of linguistic and visuospatial disorders (44,70) . It is, however, controversial whether DLB constitutes a disorder different from or overlapping with PDD. By convention,
DLB is only considered when the cognitive changes appear before, with or within 1 yr after the occurrence of parkinsonism and cannot be proposed when they appear several years later (69) . At a
192 Dubois and Pillon
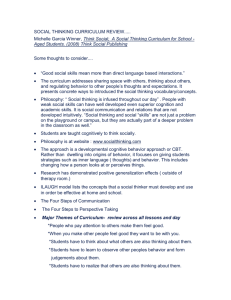
Table 3
Diagnostic Contribution of Motor and Cognitive Deficits
MDP
MSA
PDD
PSP
DLB
CBD
Motor Syndrome
L-dopa React Axial Synd
±
-
+
-
+
±
-
+
+
-
+
+
Severity
+
+
±
±
+
±
Cognitive Changes
Occurrence Cortical Signs early early late early early late
-
-
-
-
+
+
, absent; ±, mild or discussed; +, moderate or present in a proportion of patients; ++, severe and present in a majority of patients.
first glance, the clinical and cognitive profiles of both diseases are rather different with cortical signs only in DLB. The profile of attentional impairments and fluctuating attention (71) and the cognitive pattern at the Mattis Dementia Rating Scale (72) would be, however, rather similar in PDD and DLB, and postmortem examination revealed cortical Lewy bodies in both diseases, suggesting that their differential diagnosis may be more difficult than previously thought (73) .
CONCLUSION
Appropriate tests may help to differentiate among diseases associated with parkinsonism (Table 3).
Schematically, three categories can be distinguished. The first group is defined by mild cognitive deficits. It includes PD and MSA, which have a similar subcorticofrontal pattern of impairment. In the second group (PSP), striatofrontal dysfunction is so severe that it leads to dramatic planning, monitoring, and recall deficits, evolving toward dementia. The third group of diseases (CBD and DLB) is characterized by signs of cortical involvement with asymmetric instrumental disorders in CBD (praxic and linguistic deficits) and more severe dementia with hallucinations in DLB. The inclusion of PDD in the second or the third category is an object of debate and further studies are required.
The neuropsychological profiles described herein are valid when applied to a group of patients with a particular disease. To assess individuals is more difficult. The distribution of the subcortical lesions and the severity of the resulting denervation can vary. The association of cortical lesions with those of the basal ganglia can produce composite pictures. Age at onset and disease duration can alter the neuropsychological picture at different points in time. Nevertheless, appropriate neuropsychological testing is a useful technique for investigating the neuronal pathways affected in these diseases, and can contribute, not only to the diagnosis, but also to our understanding of the underlying pathology. A better clinical knowledge of these diseases will allow the progressive selection and elaboration of shorter and more discriminant tools. Longitudinal studies with pathological confirmation are necessary to attain this aim ( see below).
RESEARCH TO BE DONE TO AMELIORATE
THE NEUROPSYCHOLOGICAL EVALUATION
OF ATYPICAL PARKINSONIAN DISORDERS
Three directions:
• Elaboration of diagnostic criteria for subcorticofrontal dementia.
• Validation of new neuropsychological tools more sensitive to the specific aspects of each disease.
• Longitudinal evaluation of each disease with the same tools to better evaluate their sensitivity and specificity and postmortem anatomo-pathological correlation when possible.
Added Value of the Neuropsychological Evaluation 193
REFERENCES
1. Litvan I, Agid Y, Calne D, et al. Clinical research criteria for the diagnosis of progressive supranuclear palsy (Steele–
Richardson–Olszewski syndrome): Report of the NINDS-SPSP International Workshop. Neurology 1996;47:1–9.
2. Litvan I, Agid Y, Goetz C, et al. Accuracy of clinical diagnosis of corticobasal degeneration. Neurology 1997;48:119–125.
3. Hughes AJ, Daniel SE, Kilford L, Lees AJ. The accuracy of clinical diagnosis of idiopathic Parkinson’s disease: a clinicopathological study. J Neurol Neurosurg Psychiatry 1992;55:181–184.
4. Troster AI, Woods SP, Fields JA, et al. Neuropsychological deficits in essential tremor: an expression of cerebellothalamo-cortical pathophysiology? Eur J Neurol 2002;9:143–151.
5. Mattis S. Dementia Rating Scale. Odessa, FL: Psychological Assessment Resources Inc., 1988.
6. Dubois B, Slachevsky A, Litvan I, Pillon B. The FAB: a Frontal Assessment Battery at bedside. Neurology
2000;55:1621–1626.
7. Nelson HE. A modified Card Sorting Test sensitive to frontal lobe defect. Cortex 1976;12:313–324.
8. Benton AL. Differential behavioral effects in frontal lobe disease. Neuropsychologia 1968;6:53–60.
9. Reitan RM. Validity of the Trail Making Test as an indication of organic brain damage. Percept Mot Skills 1958;8:271–276.
10. Golden CJ. Stroop Color and Word Test. Chicago: Stoelting Company, 1978.
11. Luria AR. Higher Cortical Functions in Man. New York, NY: Basic Books, 1966.
12. Lhermitte F, Pillon B, Serdaru M. Human autonomy and the frontal lobes, I: imitation and utilization behaviors: a neuropsychological study of 75 patients. Ann Neurol 1986;19:326–334.
13. Delis DC, Kramer JH, Kaplan E, Ober BA. California Verbal Learning Test: Research Edition. New York: Psychological Corporation, 1987.
14. Grober E, Buschke H. Genuine memory deficits in dementia. Dev Neuropsychol 1987;3:13–36.
15. Goodglass H, Kaplan E. The Assessment of Aphasia and Related Disorders. Philadelphia: Lea & Febiger, 1976.
16. Heilman KM, Gonzalez Rothi LJ. Apraxia. In: Heilman KM, Valenstein E, eds. Clinical Neuropsychology, 2nd ed.
Oxford: Oxford University Press, 1985:131–150.
17. Cummings JL, Mega M, Gray K, Rosenberg-Thompson S, Carusi DA, Gornbein J. The Neuropsychiatric Inventory: comprehensive assessment of psychopathology in dementia. Neurology 1994;44:2308–2314.
18. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed. Washington, DC:
American Psychiatric Association, 1994.
19. Quinn N, Critchley P, Marsden CD. Young onset Parkinson’s disease. Mov Disord 1987; 2:73–91.
20. Cooper JA, Sagar HJ, Jordan N, Harvey NS, Sullivan EV. Cognitive impairment in early untreated Parkinson’s disease and its relationship to motor disability. Brain 1991;114:2095–2122.
21. Robbins TW, James M, Lange KW, Owen AM, Quinn NA, Marsden CD. Cognitive performance in Multiple System
Atrophy. Brain 1992;115:271–291.
22. Pillon B, Gouider-Khouja N, Deweer B, et al. Neuropsychological pattern of striatonigral degeneration: comparison with Parkinson’s disease and progressive supranuclear palsy. J Neurol Neurosurg Psychiatry 1995;58:174–179.
23. Zetusky WJ, Jankovic J, Pirozzolo FJ. The heterogeneity of Parkinson’s disease: clinical and prognostic implications.
Neurology 1985;35:522–526.
24. Maher ER, Lees AJ. The clinical features and natural history of the Steele–Richardson–Olszewski syndrome (progressive supranuclear palsy). Neurology 1986;36:1005–1008.
25. Pillon B, Dubois B, Ploska A, Agid Y. Severity and specificity of cognitive impairment in Alzheimer’s, Huntington’s, and Parkinson’s diseases and progressive supranuclear palsy. Neurology 1991;41:634–643.
26. Wenning GK, Litvan I, Jankovic J, et al. Natural history and survival of 14 patients with corticobasal degeneration confirmed at postmortem examination. J Neurol Neurosurg Psychiatry 1998;64:184–189.
27. Byrne EJ, Lennox G, Lowe J, Godwin-Austen RB. Diffuse Lewy body disease: clinical features in 15 cases. J Neurol
Neurosurg Psychiatry 1989;52:709–717.
28. Tounsi H, Deweer B, Ergis AM, et al. Sensitivity to semantic cuing: An index of episodic memory dysfunction in early
Alzheimer’s disease. Alzheimer disease and associated disorders 1999;13:38–46.
29. Pillon B, Deweer B, Michon A, Malpand C, Agid Y, Dubois B. Are explicit memory disorders of progressive supranuclear palsy related to damage to striatofrontal circuits? Comparison with Alzheimer’s, Parkinson’s, and Huntington’s diseases. Neurology 1994;44:1254–1270.
30. Taylor AE, Saint-Cyr JA, Lang AE. Memory and learning in early Parkinson’s disease: evidence for a “frontal lobe syndrome.” Brain Cogn 1990;13:211–232.
31. Buytenhuijs EJ, Berger JC, van Spaendonck KP, Horstink MW, Borm GF, Cools AR. Memory and learning strategies in patients with Parkinson’s disease. Neuropsychologia 1994;32:335–342.
32. Pillon B, Blin J, Vidailhet M, et al. The neuropsychological pattern of corticobasal degeneration. Comparison with progressive supranuclear palsy and Alzheimer’s disease. Neurology 1995; 45:1477–1483.
33. Massman PJ, Kreiter KT, Jankovic J, Doody RS. Neuropsychological functioning in cortical-basal ganglionic degeneration: differenciation from Alzheimer’s disease. Neurology 1996;46:720–726.
194 Dubois and Pillon
34. Connor DJ, Salmon DP, Sandy TJ, Galasko D, Hansen LA, Thal L. Cognitive profiles of autopsy-confirmed Lewy body variant vs pure Alzheimer’s disease. Arch Neurol 1998; 55:994–1000.
35. Brown RG, Marsden CD. “Subcortical dementia”: the neuropsychological evidence. Neurosci 1988;25:363–387.
36. Leiguarda R, Merello M, Nouzeilles MI, Balej J, Rivero A, Nagues M. Limb-kinetic apraxia in corticobasal degeneration: clinical and kinematic features. Mov Disord 2003;18:49–59.
37. Maher ER, Smith EM, Lees AJ. Cognitive deficits in the Steele–Richardson–Olszewski syndrome (progressive supranuclear palsy). J Neurol Neurosurg Psychiatry 1985;48:1234–1239.
38. Ross GW, Mahler ME, Cummings JL. The dementia syndromes of Parkinson’s disease: cortical and subcortical features. In: Huber SJ, Cummings JL, eds. Parkinson’s Disease: Neurobehavioral Aspects. Oxford: Oxford University
Press,1992:132–148.
39. Taylor AE, Saint-Cyr JA, Lang AE. Frontal lobe dysfunction in Parkinson’s disease. Brain 1986;109:845–883.
40. Owen AM, Robbins TW. Comparative neuropsychology of Parkinsonian syndromes. In: Wolters EC, Scheltens P, eds.
Mental Dysfunction in Parkinson’s Disease. Proceedings of the European Congress on Mental Dysfunction in
Parkinson’s Disease held in Amsterdam on 20–23 October 1993. Amsterdam: Vrije Universiteit, 1993:221–241.
41. Cummings JL. Psychosis in basal ganglia disorders. In: E Wolters E, Scheltens P, eds. Mental Dysfunction in
Parkinson’s Disease. Proceedings of the European Congress on Mental Dysfunction in Parkinson’s Disease held in
Amsterdam on 20–23 October 1993. Amsterdam: Vrije Universiteit, 1993:257–268.
42. Litvan I, Paulsen JS, Mega MS, Cummings JL. Neuropsychiatric assessment of patients with hyperkinetic and hypokinetic movement disorders. Arch Neurol 1998;55:1313–1319
43. Litvan I, Mega MS, Cummings JL, Fairbanks L. Neuropsychiatric aspects of progressive supranuclear palsy. Neurology 1996;47:1184–1189.
44. Aarsland D, Ballard G, Larsen JP, McKeith I. A comparative study of psychiatric symptoms in dementia with diffuse
Lewy body disease and Parkinson’s disease with and without dementia. Int J Geriatr Psychiatry 2001;16:528–536.
45. Cummings JL, Litvan I. Neuropsychiatric aspects of corticobasal degeneration. In: Litvan I, Goetz CG, Lang AE, eds. Corticobasal Degeneration. Advances in Neurology, vol. 82. Philadelphia: Lippincott, Williams & Wilkins,
2000:147–152.
46. Pillon B, Boller F, Levy R, Dubois B. Cognitive deficits and dementia in Parkinson’s disease. In: Boller F, Grafman J
(eds.). Handbook of Neuropsychology, vol 6. Aging and Dementia. Amsterdam: Elsevier, 2001:311–371.
47. Slaughter JR, Slaughter KA, Nichols D, Holmes SE, Martens MP. Prevalence, clinical manifestations, etiology, and treatment of depression in Parkinson’s disease. J Neuropsychiatry Clin Neurosci 2001;13:187–196.
48. Pluck GC, Brown RG. Apathy in Parkinson’s disease. J Neurol Neurosurg Psychiatry 2002;73:636–642.
49. Czernecki V, Pillon B, Houeto JL, Pachon JB, Levy R, Dubois B. Motivation, reward, and Parkinson’s disease: influence of dopatherapy. Neuropsychologia 2002;40:2257–2267.
50. Katzen HL, Levin BE, Llabre ML. Age of disease onset influences cognition in Parkinson’s disease. J Int Neuropsychol
Soc 1998;4:285–290.
51. Meco G, Gasparini M, Doricchi F. Attentional functions in multiple system atrophy and Parkinson’s disease. J Neurol
Neurosurg Psychiatry 1996;60:393–398.
52. Soliveri P, Monza D, Paridi D, et al. Neuropsychological follow-up in patients with Parkinson’s disease, striatonigral degeneration-type multisystem atrophy, and progressive supranuclear palsy. J Neurol Neurosurg Psychiatry
2000;69:313–318.
53. Brown RG, Pillon B, Uttner I, and Members of the Neuropsychology Working Group and NNIPPS Consortium, France,
Germany, UK. Cognitive function in patients with progressive supranuclear palsy and multiple system atrophy. The
Movement Disorder Society, 7th International Congress of Parkinson’s disease and Movement Disorders, November
2002. Book of Abstracts, 2002, P706.
54. Ghika J. Mood and behavior in disorders of the basal ganglia. In: Bogousslavsky J, Cummings JL, eds. Behavior and
Mood Disorders in Focal Brain Lesions. Cambridge: Cambridge University Press, 2000:122–200.
55. Dubois B, Pillon B, Legault F, Ajid Y, Lhermitte F. Slowing of cognitive processing in progressive supranuclear palsy.
A comparison with Parkinson’s disease. Arch Neurol 1988;45:1194–1199.
56. Johnson R. Event-related brain potentials. In: Litvan I, Agid Y, eds. Progressive Supranuclear Palsy. Oxford: Oxford
University Press, 1992:122–154.
57. Grafman J, Litvan I, Stark M. Neuropsychological features of progressive supranuclear palsy. Brain Cogn 1995;28:311–320.
58. Esmonde T, Giles E, Xuereb J, Hodges J. Progressive supranuclear palsy presenting with dynamic aphasia. J Neurol
Neurosurg Psychiatry 1996;60:403–410.
59. Pharr V, Uttl B, Stark M, Litvan I, Fantie B, Grafman J. Comparison of apraxia in corticobasal degeneration and progressive supranuclear palsy. Neurology 2001;56:957–963.
60. Dubois B, Défontaines B, Deweer B, Malapani C, Pillon B. Cognitive and behavioral changes in patients with focal lesions of the basal ganglia. In: Weiner WJ, Lang AE, eds. Behavioral Neurology of Movement Disorders. Advances in
Neurology, vol. 65. New York: Raven, 1995: 29–41.
Added Value of the Neuropsychological Evaluation 195
61. Slachevsky A, Pillon B, Beato R, et al. The “Signe de l’Applaudissement” in PSP. American Academy of Neurology
54th Annual Meeting, Denver, April 13–20, 2002. Neurology 2002;58(Suppl 3):P06.139.
62. Kertez A, Martinez-Lage P, Davidson W, Munoz DJ. The corticobasal degeneration syndrome overlaps progressive aphasia and frontotemporal dementia. Neurology 2000;55:1368–1375.
63. Bergeron C, Davis A, Lang AE. Corticobasal ganglionic degeneration and progressive supranuclear palsy presenting with cognitive decline. Brain Pathology 1998;8:355–365.
64. Lang AE, Maragonore D, Marsden CD, et al. Movement Disorder Society Symposium on cortico-basal ganglionic degeneration (CBGD) and its relationship to other asymmetrical cortical degeneration syndromes. Mov Disord
1996;11:346–357.
65. Leiguarda R, Lees AJ, Merello M, Starkstein S, Marsden CD. The nature of apraxia in corticobasal degeneration. J Neurol
Neurosurg Psychiatry 1994;57:455–459.
66. Spatt J, Bak T, Bozeat S, Patterson K, Hodges JR. Apraxia, mechanical problem solving and semantic knowledge: contributions to object usage in corticobasal degeneration. J Neurol 2002;249:601–608.
67. Frattali CM, Grafman J, Patronas N, Makhlouf MS, Litvan I. Language disturbances in corticobasal degeneration.
Neurology 2000;54:990–992.
68. Grimes DA, Lang AE, Bergeron C. Dementia is the most common presentation of corticobasal ganglionic degeneration. Neurology 1999;53:1969–1974.
69. Barber R, Panikkar A, McKeith IG. Dementia with Lewy bodies: diagnosis and management. Int J Geriatr Psychiatry
2001;16(Suppl 1):12–18.
70. Gnanalingham K, Byrne E, Thornton A, Samabrook MA, Bannister P. Motor and cognitive function in Lewy body dementia: comparison with Alzheimer’s and Parkinson’s disease. J Neurol Neurosurg Psychiatry 1997;62:243–252.
71. Ballard CG, Aarsland D, McKeith I, et al. Fluctuations in attention: PD dementia vs DLB with parkinsonism. Neurology 2002;59:1714–1720.
72. Aarsland D, Litvan I, Salmon D, Galasko D, Wentzel-larsen T, Larsen JP. Performance on the dementia rating scale in
Parkinson’s disease with dementia and dementia with Lewy bodies: comparison with progressive supranuclear palsy and Alzheimer’s disease. J Neurol Neurosurg Psychiatry 2003;74:1215–1220.
73. Apaydin H, Ahlskog JE, Parisi JE, Boeve BF, Dickson DW. Parkinson disease neuropathology: later-developing dementia and loss of the levodopa response. Arch Neurol 2002;59:102–112.