R A : HEUMATOID
advertisement

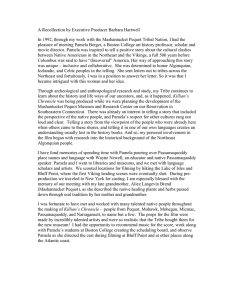
RHEUMATOID ARTHRITIS: OVERVIEW AND NEW INFORMATION Pamela E. Prete MD, FACP, FACR Section Chief, Rheumatology Professor of Medicine, Emeritus THIS CASE 36 female complains of fatigue, has right 3rd mcp And left 2nd PIP joint swelling for 5 months, BUT no am stiffness and minimal response to NSAIDS. PE shows no other joint involvement, no RA nodules. X-rays show no erosions or JSN. Pamela E. Prete MD LABORATORY RESULTS Dr Prete does a full clinical musculoskeletal exam and orders a bunch of tests But the Results are NOT back yet…So Does she have this disease Rheumatoid arthritis ---whatever that is Pamela E. Prete MD Hemoglobin is 12.1 WBC 4500 Platelets 550,000 ( normal ?) ESR 46mm/hour C- reactive protein 12 ( normal < 5) RF is 1:80 RHEUMATOID ARTHRITIS - DEFINITION Pamela E. Prete MD A prototypic chronic systemic auto-inflammatory disease with features of autoimmunity Of undetermined etiology involving primarily the synovial membranes and articular structures With pain, stiffness, and swelling of joints, leading to deformity and ankylosis (fused joints) With significant extra-articular manifestations related to the widespread systemic auto inflammation. RHEUMATOID ARTHRITIS – THE MOST COMMON AUTOINFLAMMATORY/AUTOIMMUNE DISEASE 1% population or 3 per 10,000 3:1 female to male Highest in 3rd and 4th decades Two peaks incidence Morbid/mortal disease Description dates to the 17th century -A New World Disease Pamela E. Prete MD RHEUMATOID ARTHRITIS Affects the peripheral joints in a symmetric pattern. Extra-articular involvement of organs such as the skin, heart, lungs, and eyes can be significant. Constitutional symptoms, including Fatigue, malaise, and morning stiffness Pamela E. Prete MD FIRST AND FOREMOST - INFLAMMATORY ARTHRITIS SYMMETRIC Pamela E. Prete MD MORNING STIFFNESS… Not just AM but after any long period of rest Must elicit correctly Our case patient did not have it,….. Pamela E. Prete MD Needs to be >1 hour - FEET TOO “BUNIONS” WITH COCKUP TOES AND Feet are involved 90% MTP’s ( Although patients get Hallux valgus – the 1st MTP is spared in RA) -- Pamela E. Prete MD WHAT IS MOST CHARACTERISTIC OF RA? - PATHOPHYSIOLOGY OF RA SYNOVITIS Normal Diarthrodial JOINT Pamela E. Prete MD RA SYNOVITIS- PANNUS T lymphocytes, CD 4 helper cells, macrophages Pamela E. Prete MD NORMAL SYNOVIAL LINING Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD SYNOVIAL PANNUS Pamela E. Prete MD SYNOVITIS CAUSES THE EROSIONS AND JUXTA – ARTICULAR OSTEOPENIA Pamela E. Prete MD MUSCULOSKELETAL ULTRASOUNDDETECTS SUBCLINICAL INFLAMMATION Pamela E. Prete MD RHEUMATOID ARTHRITIS – AN AUTOINFLAMMATORY DISEASE WITH AUTOIMMUNE FEATURES- AUTOANTIBODIES ANA positive in 20% Screening test Rheumatoid Factor New RA autoantibody Anti Cyclic Citrullinated Peptide (anti CCP) Pamela E. Prete MD RHEUMATOID FACTOR IS AN 1. 3. 4. 5. 6. A human antibody against Fc portion human Ig Usually IgM directed against IgG (but any combo has been noted) Binds Complement Not diagnostic of RA Does NOT follow disease activity Seen in any disease with polyclonal b cell activation Pamela E. Prete MD 2. AUTOANTIBODY NEW AUTOANTIBODY ANTI CCP What is a citrullinated exchange of the charged arginine for peptide? the non charged citrulline Pamela E. Prete MD 1. Newest autoantibody found in RA patients 2. Highly specific for RA but not sensitive 3. Associated with “shared epitope” 3. RA disease- CVD, more joint destruction WHAT IS THE EVIDENCE FOR GENETIC FACTORS IN RHEUMATOID ARTHRITIS? But only certain alleles of HLA DR4 All RA associated alleles “share” an amino acid sequence, located HLA DRB1 gene In all populations, RA susceptibility is in the “shared epitope” Pamela E. Prete MD 1970’s association with HLA DR4 THE IMMUNE CASCADE IN RA Dendritic T Co-stimulation required TNF alpha Pamela E. Prete MD macrophage TNF IL-1 IL-6 Co-stimulation required B Anti-CCP Rheumatoid factors WHAT DO WE KNOW ABOUT THE ETIOLOGY OF RHEUMATOID ARTHRITIS? Genetic “shared epitope” 67-74 HLA DRB1 Autoreactive Polyclonal B cells Autoantibodies RF and Anti CCP Complement cascade activated Immune complexes are formed Production of certain cell products the activate inflammation and destruction - CYTOKINES Pamela E. Prete MD Interleukin 1 Tumor necrosis factor Interleukin 6 RHEUMATOID ARTHRITIS – SYSTEMIC AUTOIMMUNE / AUTO INFLAMMATORY DISEASE- By causing… 1. Synovitis 2. Serositis 3. Nodules 4. Vasculitis 5. Autoantibodies Pamela E. Prete MD How dose RA affect all these organ systems ? RA SYSTEMIC DISEASE—SICCA SYNDROME –DRY EYE AND MOUTH Major cause of Secondary Sjogren’s disease Defined as sicca with Lymphocytic infiltration of the lacrimal gland Pamela E. Prete MD KERATOCONJUNCTIVITIS SICCA (KCS) DRY EYE WITH THINNING OF THE SCLERA Pamela E. Prete MD SCLEROMALACIA- THINNING OF SCLERA Pamela E. Prete MD Blue choroid coming through thinned sclera Scleromalacia perforans - rare historic note only RHEUMATOID LUNG - MOST SERIOUS VISCERAL ORGAN AFFECTED BY RHEUMATOID ARTHRITIS Rheumatoid nodules Pamela E. Prete MD **LUNG Most common small bilateral pleural effusions Cause of lung fibrosis Pulmonary vasculitis Caplan’s syndrome CAPLAN’S SYNDROME First reported in coal miners with RA RA nodules If solitary must biopsy RA patients have nodules elsewhere Can also result as an abnormal rxn to methotrexate (methotrexate nodulosis) Pamela E. Prete MD SUMMARY OF RHEUMATOID LUNG Pleura ---------------Pleuritis, pleural effusions Air way------------- Cricoarytenoid arthritis, bronchiolitis Parenchyma---------Pneumonitis, BOOP, LIP, nodules, lung fibrosis Pulmonary vessels---- -----------Vasculitis Lymphoid tissue----Lymphoid hyperplasia or lymphoma RA treatment induced Lung --------------------------Methotrexate fibrosis, infection reactivation of TB Pamela E. Prete MD RHEUMATOID ARTHRITIS Rare presentation Rheumatoid factor, present in 93% Subcutaneous nodules were present in 47%. left-sided chest pain most common symptom pericardial friction rub Cardiomegaly,, accompanied by pleural effusion pericardial fluid low sugar concentration elevated lactic dehydrogenase low complement Pamela E. Prete MD PERICARDITIS NEUROLOGIC Entrapment Carpal Wrist Synovitis in RA tunnel C1 C2 subluxation synovial involvement of the ligament over the odontoid Pamela E. Prete MD RHEUMATOID NODULES? Occur over extensor tendons Elbow most common Firm nodule -0.3-1cm Occur with disease activity Can occur anywhere Have a characteristic pathology Pamela E. Prete MD NODULES Pamela E. Prete MD RA NODULE -PATHOGNOMONIC PATHOLOGY Central necrosis Palisading histiocytes Fibrotic capsule ULTRASOUND Hypoechoic homogeneous mass with anechoic center Pamela E. Prete MD RHEUMATOID VASCULITIS - A THING OF THE PAST BECAUSE OF THE TARGETED THERAPIES Digital infarcts Small vessel Vasculitis Result in Lung hemorrhage or GI bleeding Pamela E. Prete MD warning sign of small vessel vasculitis in RA or impending digital gangrene WHAT IS NEW IN RA The pathophysiology and new genetic information has led to specific targeted immunotherapy and the use of the new BIOLOGICS. AND the discovery that Rheumatoid arthritis has multiple subclasses based on the responses to the targeted therapies. BUT WE NEED TO START THERAPY EARLIER AT THE MOLECULAR LEVEL –HOW CAN WE DO THAT? Pamela E. Prete MD AND WHY HAS IT BEEN A GREAT DECADE FOR RHEUMATOID ARTHRITIS? THE “OLD” AMERICAN COLLEGE OF RHEUMATOLOGY (ACR) CRITERIA FOR THE DIAGNOSIS OF RHEUMATOID ARTHRITIS 7 1. 3. 4. 5. 6. 7. Pamela E. Prete MD 2. Morning stiffness Arthritis of 3 or more joint areas, observed by a physician. Arthritis of hand and wrist joints Symmetric arthritis Rheumatoid nodule Serum Rheumatoid Factor Radiographic changes hand and wrist radiographs--erosions or juxta-articular osteopenia NEW ACR EULAR CRITERIA FOR RA 4 DOMAINS 1. Domain: Joint involvement – max 5points 2. Domain: Serology -max 3points 3. Domain: Duration of synovitis- max 1point 4. Domain: Acute phase reactants -max 1point YOU NEED 6 points for a DEFINITE RA DIAGNOSIS Pamela E. Prete MD DOMAIN: JOINT INVOLVEMENT Note: Patients receive the highest point level they fulfill within each domain. For example, a patient with five small joints involved and four large joints involved scores 3 points. Pamela E. Prete MD – 1 medium-large joint (0 points) – 2-10 medium-large joints (1 point) – 1-3 small joints (2 points) – 4-10 small joints (3 points) – More than 10 small joints (5 points) DOMAIN: SEROLOGY -MAX 3POINTS What is CCP? Pamela E. Prete MD -No RF or anti-CCP) (0 points) – One positive at low titer, < 3x normal (2 points) – One positive at high titer, > 3x normal (3 points) DOMAIN: DURATION OF SYNOVITIS- MAX 1POINT < Pamela E. Prete MD 6 weeks (0 points) >6 weeks or longer (1 point) DOMAIN: ACUTE PHASE REACTANTS Neither (CRP) nor (ESR) is abnormal (0 points) –Abnormal CRP or abnormal ESR (1 point) Pamela E. Prete MD SUMMARY OF THE NEW RA CRITERIA Pamela E. Prete MD WORK UP FOR RA INCLUDES Specific history and physical Serologies CBC and Differential, ESR, C Reactive protein, ANA, Rheumatoid factor and Anti CCP On the spot imaging with musculoskeletal ultrasound –newest modality for Rheumatologists Joint tap- Synovial fluid – inflammatory- low glucose Other Imaging X-rays- hands, feet , MRI early erosions, Bone scan Pamela E. Prete MD Fam hx, msk exam, ROS TREATMENT BEFORE THE BIOLOGICS NSAIDs for stiffness Corticosteroids for inflammation and to suppress the autoimmunity Disease Modifying Anti rheumatic Drugs (DMARDs) Pamela E. Prete MD Drug of choice -Methotrexate 7.5-25mg weekly But also Cyclosporine, Azathioprine, cyclophosphamide MONOCLONAL ANTIBODIES AND RA Tumor Necrosis (alpha) Inhibitors 5 FDA approved Rituximab (rituxan) anti CD20 B cells Abatacept anti Costimulation blocking CD80/86 CD28 Anakinra (Kineret) anti IL 1 receptor DOES NOT WORK Tocilizumab (Actemra) anti IL 6 Pamela E. Prete MD Infliximab ( Remicaid ) an infusion Etanercept ( Enbrel) against soluble TNF receptors Adalimunab (Humira) against soluble and membrane bound TNF receptors Certolizumab (Cimza) pegylated Golimumab (Simponi) Pamela E. Prete MD THESE TARGETED THERAPIES HAVE CHANGED THE COURSE OF RA… Pamela E. Prete MD No deformities No synovectomies No splinting No small vessel vasculitis Resolution of nodules Less RA lung Less Mortality from CVD Decreased incidence of Non Hodgkin’s Lymphoma RHEUMATOID ARTHRITIS SUMMARY Eyes, lungs, heart, lymph glands There the unknown antigen trigger Genetic predisposition-- HLA DR4 and “Shared” epitope located on HLA DRB1 Autoantibodies rheumatoid factor and new anti cyclic citrullinated peptides- define subclasses of RA Have pathogenic and prognostic significance Involves the Adaptive and Innate Immune system Pamela E. Prete MD Auto-inflammatory disease ( with autoimmune features) resulting in symmetric joint destruction, systemic disease RHEUMATOID ARTHRITIS SUMMARY Multiple effector cells release cellular products cytokines, in synovial proliferation resulting in joint and multiple organ destruction Immune complexes and complement are active Multiple theories have been proposed to explain the findings Suppression of the auto reactivity improves Rheumatoid arthritis Pamela E. Prete MD RHEUMATOID ARTHRITIS SUMMARY But Targeted therapies have changed the course of Rheumatoid arthritis Information from Targeted therapy suggest T cell or IL 1 suppression not helpful once the disease is apparent Varied responses to the Targeted therapies indicate Rheumatoid arthritis is not one disease and autoimmune processes overlap between autoimmune diseases Pamela E. Prete MD ATTENTION If questions or help with a patient page Dr Prete or email pamela.prete@va.gov Pamela E. Prete MD THANK YOU FOR YOUR KIND Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD Definitions JOINT DISTRIBUTION (0-5) 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 Definition of “JOINT INVOLVEMENT” - Any swollen or tender joint (excluding DIP of hand and feet, 1st MTP, 1st CMC) SEROLOGY (0-3) Negative RF AND negative ACPA 0 Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 ≥6 = definite RA - Additional evidence from MRI / US may be used for confirmation of the clinical findings Pamela E. Prete MD 1 large joint Definitions JOINT DISTRIBUTION (0-5) 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 Definition of “SMALL JOINT” Negative RF AND negative ACPA 0 MCP, PIP, MTP 2-5, thumb IP, wrist Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 SEROLOGY (0-3) SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 ≥6 = definite RA NOT: DIP, 1st CMC, 1st MTP Pamela E. Prete MD 1 large joint Definitions JOINT DISTRIBUTION (0-5) 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA 0 Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 ≥6 = definite RA Definition of “LARGE JOINT” Shoulder, elbow, hip, knee, ankles Pamela E. Prete MD 1 large joint Definitions JOINT DISTRIBUTION (0-5) 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA 0 Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 ≥6 = definite RA Definition of “>10 JOINTS” - At least one small joint - Additional joints include: temporomandibular, sternoclavicular, acromioclavicular, and others (reasonably expected in RA) Pamela E. Prete MD 1 large joint Definitions JOINT DISTRIBUTION (0-5) 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA 0 Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 ≥6 = definite RA Definition of “SEROLOGY” Pamela E. Prete MD 1 large joint Negative: ≤ULN (for the respective lab) Low positive: >ULN but ≤3xULN High positive: >3xULN Definitions JOINT DISTRIBUTION (0-5) 0 2-10 large joints 1 1-3 small joints (large joints not counted) 2 4-10 small joints (large joints not counted) 3 >10 joints (at least one small joint) 5 SEROLOGY (0-3) Negative RF AND negative ACPA 0 Low positive RF OR low positive ACPA 2 High positive RF OR high positive ACPA 3 SYMPTOM DURATION (0-1) <6 weeks 0 ≥6 weeks 1 ACUTE PHASE REACTANTS (0-1) Normal CRP AND normal ESR 0 Abnormal CRP OR abnormal ESR 1 ≥6 = definite RA Definition of “SYMPTOM DURATION” Refers to the patient’s self-report on the maximum duration of signs and symptoms of any joint that is clinically involved at the time of assessment. Pamela E. Prete MD 1 large joint NEW RA CRITERIA Patients are definitively diagnosed with RA if they score 6 or more points according to the following criteria Note: Patients receive the highest point level they fulfill within each domain. For example, a patient with five small joints involved and four large joints involved scores 3 points. Pamela E. Prete MD 1. Domain: Joint involvement – 1 medium-large joint (0 points) – 2-10 medium-large joints (1 point) – 1-3 small joints (2 points) – 4-10 small joints (3 points) – More than 10 small joints (5 points) 2. Domain: Serology – No rheumatoid factor (RF) or anti–citrullinated protein antibody (anti-CCP) (0 points) – One of these two tests is positive at low titer, less than three times the upper limit of normal (2 points) – One test is positive at high titer, more than three times the upper limit of normal (3 points) 3. Domain: Duration of synovitis – Less than 6 weeks (0 points) – 6 weeks or longer (1 point) 4. Domain: Acute phase reactants – Neither C-reactive protein (CRP) nor erythrocyte sedimentation rate (ESR) is abnormal (0 points) – Abnormal CRP or abnormal ESR (1 point) 4 DOMAINS 1.Domain: Joint involvement – max 5points 2. Domain: Serology -max 3points 3. Domain: Duration of synovitis- max 1point 4. Domain: Acute phase reactants -max 1point Pamela E. Prete MD DOMAIN: JOINT INVOLVEMENT Note: Patients receive the highest point level they fulfill within each domain. For example, a patient with five small joints involved and four large joints involved scores 3 points. Pamela E. Prete MD – 1 medium-large joint (0 points) – 2-10 medium-large joints (1 point) – 1-3 small joints (2 points) – 4-10 small joints (3 points) – More than 10 small joints (5 points) DOMAIN: SEROLOGY -MAX 3POINTS (0 points) (2 points) One positive at high titer, > 3x normal (3 points) Pamela E. Prete MD No RF or anti-CCP) One positive at low titer, < 3x normal DOMAIN: DURATION OF SYNOVITIS- MAX1POINT • < 6 weeks • >6 weeks or longer (0 points) (1 point) DOMAIN: ACUTE PHASE REACTANTS Neither (CRP) nor (ESR) is abnormal (0 points) –Abnormal CRP or abnormal ESR (1 point) Pamela E. Prete MD LABORATORY RESULTS Anti CCP 52 units/mL (normal is < 16units/mL) RF mildly increased 1:80 ESR -64 mm/hr Urinalysis Normal Anti DD DNA abs, SSA, SSB, RNP, Smith all negative! Does she have RA? Under the old Criteria NO! Under the NEW –you bet! Pamela E. Prete MD CBC mild anemia Serum iron normal Serum ferritin normal ANA 1:40 3 ACR CRITERIA ARE PRESENT SYMMETRIC, 3 OR MORE JOINTS, AND INVOLVEMENT OF HAND AND WRIST Pamela E. Prete MD RADIOGRAPHIC CHANGES On Hand and Wrist x-rays Juxta-articular osteopenia Frank erosions Not cysts, not osteoarthritis changes Pamela E. Prete MD SYNOVIAL CAVITY >10-50 thousand wbc’s Low glucose Low complement Pamela E. Prete MD Synovial Cavity Normally only a "potential" space with 12ml of highly viscous fluid few cells. In RA, large collections of fluid ("effusions") occur RA synovial fluid is highly inflammatory Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD RA IMMUNE CASCADE Pamela E. Prete MD Pamela E. Prete MD WHY ARE ACPA IMPORTANT IN RA? Pamela E. Prete MD Pamela E. Prete MD RA – AUTO-INFLAMMATORY, WASTING DISEASE IF UNTREATED Pamela E. Prete MD RHEUMATOID ARTHRITIS – JOINT DAMAGE Pamela E. Prete MD REMEMBER THIS CASE… Family history reveals an Aunt with Rheumatoid arthritis Social history reveals she is a 2 pack a day smoker, married with two children No IVD, Medications - Tylenol 4 per day Pamela E. Prete MD You are in Arthritis Clinic and Dr Prete asks you to see a 29 YO female with fatigue and early morning stiffness that lasts all day. She states her hands have swelled and ached for the past 2 months. ETIOLOGY Worldwide, 3 cases per 10,000 population Prevalent in some Native American groups (56%) and much less prevalent in others (e.g., black persons from the Caribbean region). First-degree relatives of individuals with RA are at an increased risk (2- to 3-fold) of the disease. Disease concordance in monozygotic twins is only15-20% Because the worldwide frequency of RA is relatively constant, a ubiquitous infectious agent has been postulated to play an etiologic role. Pamela E. Prete MD ARTHRITIS? Definite swelling MCP’s, PIP’s But was it observed by a Provider >6 weeks? Pamela E. Prete MD So our patient has 1. 3 or more joints 2. Involvement of the hands and wrist 3. Symmetric Fatigue stiffness PIP and MCP involvement … She has an inflammatory arthritis but is it RA? Pamela E. Prete MD WHAT ABOUT OUR PATIENT? Rheumatoid Arthritis? ARE we sure of the diagnosis? Does the diagnosis fulfill ACR criteria? …Does it matter? Pamela E. Prete MD WHAT IS THE DIAGNOSIS?… SO WHAT ABOUT OUR PATIENT ? She had morning stiffness 3 or more joints inflamed at the same time Hand involvement Symmetric arthritis She did not have No Rheumatoid nodules No hand x-ray changes We don’t know about RF… She has 4 of the 7 ACR criteria so it is most likely she has rheumatoid arthritis just on CLINICAL EXAMINATION alone! Pamela E. Prete MD EULAR CRITERIA FOR RA-- NEW Pamela E. Prete MD score 6 or more points according to the following criteria, four domains: Domain: Joint involvement – 1 medium-large joint (0 points) – 2-10 medium-large joints (1 point) – 1-3 small joints (2 points) – 4-10 small joints (3 points) – More than 10 small joints (5 points) Note: Patients receive the highest point level they fulfill within each domain. For example, a patient with five small joints involved and four large joints involved scores 3 points Domain: Serology – Not positive for either rheumatoid factor or anti–citrullinated protein antibody (0 points) – At least one of these two tests are positive at low titer, defined as more than the upper limit of normal but not higher than three times the upper limit of normal (2 points) – At least one test is positive at high titer, defined as more than three times the upper limit of normal (3 points) . Pamela E. Prete MD REMEMBER YOU NEED 6 POINTS Domain: Duration of synovitis – Less than 6 weeks (0 points) – 6 weeks or longer (1 point) Domain: Acute phase reactants – Neither C-reactive protein nor erythrocyte sedimentation rate is abnormal (0 points) – Abnormal CRP or abnormal ESR (1 point) Pamela E. Prete MD Pamela E. Prete MD Unknown but here are the data we know Pamela E. Prete MD WHAT CAUSES RHEUMATOID ARTHRITIS … Pamela E. Prete MD Associated with the shared epitope RA-associated HLADR4 molecules (DR4) can bind and present citrullinated peptides much more efficiently Pamela E. Prete MD the shared epitope of the HLA-DR4/DR1 cluster is present in up to 90% of patients Synovial cell hyperplasia and endothelial cell activation are early events in the pathologic process that progresses to uncontrolled inflammation and consequent cartilage and bone destruction. CD4 T cells, mononuclear phagocytes, fibroblasts, osteoclasts, and neutrophils play major cellular roles in the pathophysiology of RA, while B lymphocytes produce autoantibodies (i.e., rheumatoid factors [RFs]). Abnormal production of numerous cytokines, chemokines, and other inflammatory mediators (e.g., tumor necrosis factor alpha [TNFalpha], interleukin (IL)–1, IL-6, transforming growth factor beta, IL8, fibroblast growth factor, platelet-derived growth factor) has been demonstrated in patients with RA. Ultimately, inflammation and exuberant proliferation of synovium (i.e., pannus) leads to destruction of various tissues, including cartilage, bone, tendons, ligaments, and blood vessels. Although the articular structures are the primary sites involved by RA, other tissues are also affected. Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD RHEUMATOID FACTOR Pamela E. Prete MD 1. 80% of all RA patients 2. High titer (quantity) 3. Found in serum but also Joint, pleural or pericardial fluids 4. By itself-not diagnostic 5. Found in other diseases with polyclonal stimulation of B Cells Aging Hepatitis C Chronic infections Lymphomas Other AI diseases – highest in Sjogren’s DESTRUCTIVE NATURE OF RHEUMATOID ARTHRITIS AND ITS SYSTEMIC FEATURES… We need to know it’s pathophysiology Pamela E. Prete MD TO EXPLAIN THE EROSIVE, PANNUS- JOINT DESTRUCTION Pamela E. Prete MD GENETIC FACTORS IN RHEUMATOID ARTHRITIS In all populations RA susceptibility is conferred by the shared epitope Pamela E. Prete MD Risk of RA is 2-3 if you have a relative with RA Only certain alleles of HLA DR4 confer susceptibility Susceptibility – located at 67-74 amino acids on HLA DRB1 gene All RA associated alleles “share” an amino acid sequence – the shared epitope Pamela E. Prete MD Pamela E. Prete MD Pamela E. Prete MD WHY THE JOINTS? Pamela E. Prete MD Pamela E. Prete MD RHEUMATOID ARTHRITIS - JOINT SYNOVIAL CAVITY EROSIONS JOINT DESTRUCTION Pamela E. Prete MD THE NEW TREATMENT PARADIGM Higher dose steroids for flares or extraarticular disease Occupational therapy Intraarticular steroids Physical therapy Patient education Simple analgesic Pamela E. Prete MD Orthopedic surgery