COST CONCIOUSNESS PROJECT FECAL OCCULT BLOOD TEST (FOBT) – by Kelvin Nguyen
advertisement
 – by Kelvin Nguyen")
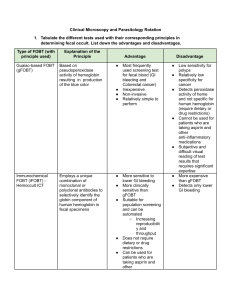
COST CONCIOUSNESS PROJECT FECAL OCCULT BLOOD TEST (FOBT) – APPROPRIATE OR NOT APPROPRIATE? by Kelvin Nguyen 05/10/2013 BACKGROUND • Fecal occult blood test is ordered in outpatient setting for colorectal cancer screening. • The test is ordered in the in-patient setting, many times for reasons not related to colorectal cancer screening. • Currently, fecal occult blood test can be done via 3 types of testing: • Stool guaiac test for fecal occult blood (gFOBT) – detects heme • HemoQuant – can quantify the heme moiety of intact hemoglobin • Fecal DNA test – extract DNA from stool sample and testing for alteration associated with cancer. • Fecal Immunochemical testing (FIT) – specific antibodies detecting globin – more specific for lower GI bleed. UCI has been using gFOBT and recently having FIT test available. BACKGROUND • gFOBT is about 30% sensitive and can go up to 90-92% with serial sampling of 3. • Normal person sheds about 0.5-1.5 ml of blood into stool over 24 hour period. gFOBT can detect as small as 2 ml to 10 ml of blood in the stool per 24hrs . • A good sample for gFOBT is when the patient is 72 hours off medications or foods that can give false positive results such as: NSAIDs and Aspirin, vitamin C, red meat, cantapoupe and other melons, grapefruit, turnips, broccoli, figs, radhish, horseradish, cauliflower, cabbage, cucumber, carrot, potato, pumpkin, zucchini, parsley. AIM • To evalulate whether or not FOBT was ordered appropriately or not • To evaluate cost-effectiveness of FOBT METHODS • Chart review of 10 patients who have been admitted in April with FOBT performed. • Acceptable indications for ordering FOBT AT ADMISSION (the FOBT is Hemmocult) on 1 study: • Symptoms of acute or chronic GI bleeding (e.g., hematemesis, melena) • Physical signs of anemia (e.g., pallor) • Anemia on admission complete blood count • Report of weight loss of at least 4.5 kg within 6 mo • Symptoms of enteric illness (fever, diarrhea) • Change in bowel habits or tenesmus • History of prior GI malignancy • History of colonic abnormalities (e.g., diverticula, arteriovenous malformation) • Other indications: anticoagulation therapy, coagulopathy, history of benign GI lesions 1Gomez JA and Diehl AK. Admission stool guaiac test : Use and Impact on patient management. The American Journal of Medicine 1992; 92: 603-06. PATIENTS • 10 patients age from 26 to 90 • 8 females and 2 males • All were admitted at UCIMC in April 2013 • Primary services include IM (4), family medicine, OB/GYN, General/Trauma surgery, Neurosurgery, CCU RESULTS • All 10/10 cases are deemed inappropriate. All are from Internal Medicine (3/4). 2 were ordered at the time of admission. • 10 cases: the test was ordered without mentioned in the notes. They were ordered during hospitalization. No follow ups were done regardless of results of the test. • 1/10 was ordered at admission with a history of anemia with lower than usual Hgb without recent scopes and rectal exam was negative for blood. • 1/10 was ordered at admission on a patient with hematemesis and melena. RESULTS • 1/10 was done during hospitalization per renal recommendation as work up for elevated BUN which renal consult did not think it was due to kidney injury. • 5/1/10 cases: the test was done because of acute Hgb drop from 11.4 to 10.2 over 24 hours. The patient has a history of anemia. • 1/10 cases: the test was done because of loose stool without blood in the stool reported. Test was positive but nothing was followed (not mentioned in the notes or consulting GI etc.) COST CONCIOUSNESS • The cost of the test to performed is almost $20.00. The patient Is billed almost $60.00. • Imagine how common FOBT is ordered as a reflex for acute Hgb drop, diarrhea, etc. 100 unnecessary tests could easily cost the patients $6000.00 REMINDER • FOBT is recommended for colorectal caner screening. • Because of low sensitivity and specificity of the test, the results are not benefiting in inpatient setting (1 single testing 30% sensitivity with each test for a combination of 3 test, the sensitivity can go up to 92% in a condition of being compliant for 3 days of restricted foods and medications). • The upcoming FIT test is even more specifically designed for colorectal cancer screening as it only picks up lower GI bleed. Therefore, ordering in the inpatient setting is even more inappropriate. CONCLUSION • Be very mindful of ordering FOBT in the inpatient hospital setting. Very soon, there will be only FIT test available! • What is the point of ordering the test without follow-up? There were studies in the past that FOBT was done and the rate of follow up on this test is very low (~30%). THANK YOU