Falk Labo Insect Sting Allergy Action Plan
advertisement

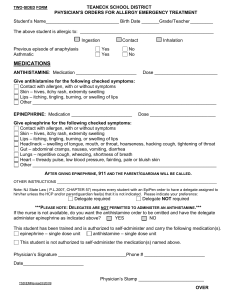
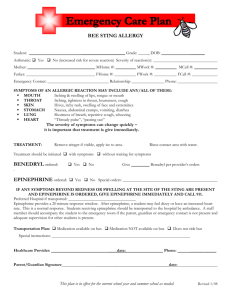
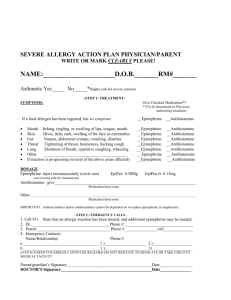
Falk Laboratory School Place Student’s Insect Sting Allergy Action Plan Name: ____________________________________________D.O.B.: ___ /___ /____ Allergy to: ____________________________________________________________ Asthma: Picture Here (THIS SECTION TO BE DEDERMINTED BY PHYSICIAN AUTHORIZING TREATMENT) Symptoms Give Checked Medication • If a bee sting has occurred, but no symptoms □ Epinephrine □ Antihistamine • Site of sting Swelling, redness, itching □ Epinephrine □ Antihistamine • Skin Itching, tingling, or swelling of lips, tongue, mouth □ Epinephrine □ Antihistamine • Stomach Nausea, abdominal cramps, vomiting, diarrhea □ Epinephrine □ Antihistamine • Throat† Tightening of throat, hoarseness, hacking cough □ Epinephrine □ Antihistamine • Lung† Shortness of breath, repetitive coughing, wheezing □ Epinephrine □ Antihistamine • Heart† Thready pulse, low blood pressure, fainting, pale, blueness □ Epinephrine □ Antihistamine • Mouth If a bee sting has occurred, but no symptoms • If reaction is progressing (several of the above areas affected), give □ Epinephrine □ Antihistamine □ Epinephrine □ Antihistamine The severity of symptoms can quickly change. †Potentially life-threatening. Medications/Doses Epinephrine (brand and dose): _______________________________________________________________ Antihistamine (brand and dose): ______________________________________________________________ Other (e.g., inhaler-bronchodilator if asthmatic): __________________________________________________ Monitoring Stay with student; alert healthcare professionals and parent. Tell rescue squad epinephrine was given; request an ambulance with epinephrine. Note time when epinephrine was administered. A second dose of epinephrine can be given 5 minutes or more after the first if symptoms persist or recur. For a severe reaction, consider keeping student lying on back with legs raised. Treat student even if parents cannot be reached. See back/attached for auto-injection technique. Emergency Contacts: Call the parent or guardian to notify them of the incident. 1. Name & Relationship_____________________________________________ Phone ___________________ 2. Name & Relationship_____________________________________________ Phone____________________ I agree to the above plan, and agree that school health personnel and my child’s physician or staff may discuss this plan if there are questions. Parent/Guardian Signature ____________________________________________________Date___________________ Doctor’s Signature _______________________________________Phone________________ Date ________________ This form MUST be signed by a licensed health care provider Print Falk Laboratory School FOR NURSE’S OFFICE USE Staff and faculty received Epinephrine Injection Training on _____/______/______ By _____________________________________________________ Notes: ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ How to use Auvi?Q® 1. Pull Auvi?Q® from the outer case 2. Pull off Red safety guard 3. Place black end against the middle of the outer thigh (through clothing, if necessary), then press firmly and hold in place for 5 seconds. Each device is a single-use injection. Seek medical attention immediately