Social Cognition, Vol. 24, No. 5, 2006, pp. 641-656
KOEHLER
FACE
PREFERENCES
ET AL.
AND THE MENSTRUAL CYCLE
DO CYCLIC CHANGES IN WOMEN’S
FACE PREFERENCES TARGET CUES TO
LONG–TERM HEALTH?
NICOLE KOEHLER
GILLIAN RHODES
LEIGH W. SIMMONS
The University of Western Australia
LESLIE A. ZEBROWITZ
Brandeis University
A shift to prefer more masculine male faces when conception risk is high may
be an adaptation for finding mates with good disease resistance. We investigated whether preferences for other facial cues to long–term health also increase when conception is likely. We examined preferences for the faces of
men with good health histories and for facial averageness and symmetry, two
putative indicators of health during development. Preferences were tested at
two points in the menstrual cycle that differed maximally in conception risk.
No cyclic changes in preferences were found. We consider implications for
the sexual selection of variation in preferences across the menstrual cycle.
There is currently considerable interest in understanding facial attractiveness from an evolutionary perspective (for reviews, see
Rhodes, 2006; Thornhill & Gangestad, 1999a). Cross–cultural agreement on attractiveness (Langlois, Kalakanis, Rubenstein, Larson,
Hallam, & Smoot, 2000) and emergence of preferences early in development (e.g., Slater, Quinn, Hayes, & Brown, 2000; Slater, Van der
Schulenberg, Brown, Badenoch, Butterworth, Parsons, 1998) suggest
This work was supported by the Australian Research Council. We thank the Institute of
Human Development (IHD) at the University of California, Berkeley for access to the data
archives used in this study.
Please send correspondence to Gillian Rhodes, School of Psychology, University of
Western Australia, 35 Stirling Highway, Crawley, WA 6009, Australia; E–mail:
gill@psy.uwa.edu.au.
641
642
KOEHLER ET AL.
that some of our preferences must reflect our biological rather than
our cultural heritage.
Theorists have proposed that certain facial traits, including
averageness, symmetry, and sexual dimorphism, may be attractive
because they signal aspects of mate quality such as health and intelligence (Gangestad & Thornhill, 1997; Penton–Voak & Perrett,
2000; Rhodes, 2006; Rhodes & Zebrowitz, 2002; Symons, 1979;
Thornhill & Gangestad, 1993, 1999a). Sexual dimorphism is also attractive in faces (Rhodes, 2006). Theoretically, masculinity could
signal immunocompetence (Folstad & Karter, 1992), and it is associated with actual health during development in humans (Rhodes,
Chan, Zebrowitz & Simmons, 2003). Preferences for these traits in
male faces could, therefore, increase reproductive success, either
because preferred mates provide indirect genetic benefits in the
form of heritable resistance to disease, or because they provide direct benefits such as resources, parental care, and reduced risk of
contagion.
Women’s preferences for men’s faces also change over the menstrual cycle. Women with a natural menstrual cycle prefer relatively
more masculine faces when conception is likely (Johnston, Hagel,
Franklin, Fink, & Grammer, 2001; Penton–Voak & Perrett, 2000;
Penton–Voak, Perrett, Castles, Kobayashi, Burt, Murray, 1999). Indeed, there has been some suggestion that a preference for masculine
faces emerges only when conception is likely, although a recent
meta–analytic review suggests that this is not the case (Rhodes,
2006). Given that facial masculinity is an honest signal of health during development in humans (Rhodes et al., 2003), a shift to prefer
more masculine faces when conception is likely could be an adaptation for obtaining genetic benefits for offspring. Similar shifts have
been observed in olfactory preferences for putative cues to mate
quality, with women preferring the scent of men with symmetric
bodies when conception is likely, but not at other phases of the menstrual cycle (Gangestad & Thornhill, 1998; Rikowski & Grammer,
1999; Thornhill & Gangestad, 1999b).
The increase in masculinity preference when conception is likely
led us to ask whether visual preferences for other facial cues to
immunocompetence and long–term health might also increase when
conception is likely. We tested this hypothesis by examining menstrual cycle variation in preferences for the faces of men with good
health histories, and for facial averageness and symmetry, two puta-
FACE PREFERENCES AND THE MENSTRUAL CYCLE
643
tive indicators of health during development (Rhodes, 2006; Rhodes
& Simmons, in press; Rhodes & Zebrowitz, 2002).
We showed female participants pairs of faces that differed either in
their medically assessed health during development, their symmetry, or their averageness. In each case, we asked participants to pick
the more attractive face, once when conception risk was high and
once when it was low. The health pairs displayed the faces of young
men who differed in their health during development, primarily in
the length and severity of infectious conditions. The individuals depicted were born in California in the 1920s and grew up before vaccinations and antibiotics were used, so that differences in health likely
reflect differences in disease resistance (Kalick, Zebrowitz, Langlois,
& Johnson, 1998). Previous research with this sample shows that
these faces contain readable cues to health, with healthier individuals rated as looking healthier than their peers (Kalick et al., 1998). Curiously, however, the healthier individuals were not rated as more
attractive than their peers. In the light of the masculinity results, we
wondered whether a preference for the healthier faces might emerge
at the fertile point of the menstrual cycle. In the averageness and
symmetry pairs, we paired low– and high–average versions of a face,
and low– and perfect–symmetry versions of a face, respectively. In a
previous study, we found no cyclic change in the preference for symmetric faces, assessed using attractiveness ratings (Koehler, Rhodes,
& Simmons, 2002). Here, we used a forced-choice method, which
may be more sensitive than ratings to subtle changes in preferences,
if participants are reluctant to assign different ratings to subtle
differences in perceived attractiveness.
Participants were tested at two phases of the menstrual cycle,
which differed maximally in conception risk: at mid–cycle, when
conception risk is highest, and early in the cycle, when conception
risk is lowest (Wilcox, Dunson, Weinberg, Trussell, & Baird, 2001).
We reasoned that if preference variation across the menstrual cycle is
an adaptation for acquiring genetic benefits, such as heritable resistance to disease, for offspring, then it should be most apparent between these phases (cf. Johnston, Arden, Macrae & Grace, 2003;
Macrae, Alnwick, Milne, & Schloerscheidt, 2002). In addition to testing women with a natural menstrual cycle, we tested pill users who
are not expected to show cyclic changes.
644
KOEHLER ET AL.
METHOD
PARTICIPANTS
Fifty female university students who were not taking any form of
oral/hormonal contraception and 52 pill takers participated in the
present study. All participants were heterosexual (by self–report)
and not currently pregnant or breast-feeding. Women with a natural
cycle all had a regular cycle, with a mean (± SD) self–reported cycle
length of 28.5 (± 1.4, N = 52) days and an actual cycle length of 29.6 (±
2.4, N = 36) days for the cycle containing the mid–cycle test session
(described later). The mean (± SD) age of women with a natural cycle
and pill using women was 22.6 (± 5.6) years (range 17–35), and 19.8 (±
3.2) years (range 17–31), respectively. Women with a natural cycle
were significantly older than pill users, t100 = 3.11, p = .0024,
two–tailed. Fifty participants completed the study for course credit,
and the remaining participants were reimbursed for travel expenses.
STIMULI
There were three stimulus sets (health, averageness, symmetry),
each consisting of 24 pairs of black-and-white front–view images of
young adult, male, Caucasian faces with neutral facial expressions.
Different faces were used in each set. In the health set, the pairs consisted of the faces of two individuals who differed in their medically
assessed health during development (examples cannot be shown
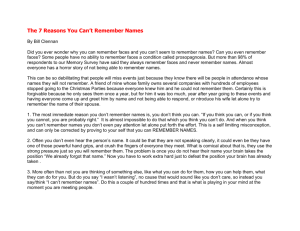
due to confidentiality). In the averageness set, each pair displayed a
low– and high–average version of the same face (Fig. 1a & c), and in
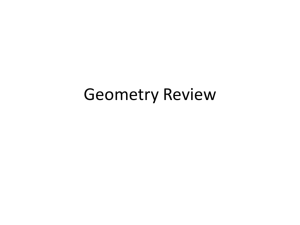
the symmetry set each pair displayed a low– and perfect–symmetry
version of the same face (Fig. 2a & b). All faces were scaled to have an
interpupil distance of 80 pixels and horizontally aligned pupils.
Blemishes and facial jewelry were removed using the stamp tool in
Adobe Photoshop. A black oval mask was placed over each face to
minimize the visibility of nonface information (Fig. 1 & 2). The outside dimensions of the mask were 280 by 420 pixels. All faces were
shown at a resolution of 72 pixels per inch.
Health Set. There were 24 health pairs, each showing two faces, of
individuals who differed in their health during development. Photographs and health scores were obtained from a longitudinal data archive, the Intergenerational Studies (IGS), held at the University of
FACE PREFERENCES AND THE MENSTRUAL CYCLE
645
California Berkeley Institute of Human Development and the
Radcliffe Henry Murray Center, and used previously by Kalick et al.
(1998; see also Rhodes et al., 2003; Rhodes, Zebrowitz, Clark,
Hightower, & McKay, 2001). The photographs depicted the individuals at age 17–18 years. The individuals were born between 1920 and
1929 and would not have been exposed to vaccinations or antibiotics
by ages 17–18 (Kalick et al., 1998). The health scores (1 = unhealthy, 5
= healthy) reflect health during development, primarily the number
and severity of infectious conditions (Kalick et al., 1998). Scores were
assigned by medical professionals based on annual medical examinations from the ages of 3 to 18 years. Faces of the 24 healthiest and 24
unhealthiest males were selected for the present study. The mean (±
SD) health scores of the males in the low and high health groups were
2.8 (± 0.3) and 3.9 (± 0.1), respectively, which differed significantly,
paired t23 = 18.91, p < .0001, two–tailed. The groups did not differ significantly in attractiveness, paired t23 = 0.99, p = 0.33, two–tailed (3.3 ±
0.7, low health; 3.5 ± 0.8, high health), as expected given Kalick et al.
(1998).
Averageness Set. Each averageness pair consisted of a low- and a
high-average version of the same individual’s face (see Fig. 1a & c).
Sixteen of these pairs were taken from Rhodes, Sumich, and Byatt
(1999) and the remaining eight pairs were created using the same
procedure. Gryphon’s Morph software was used to create low- and
high-average faces. A same–sex average face (see Fig. 1d) was used
to create low- and high-average faces. The average male face created
by Rhodes et al. (1999) was used. To create the low- and high-average
versions of each face, 120 landmark points were positioned (by eye)
on internal features of the standardized face (e.g., the corners of the
eyes, nose, and mouth), the outline of the face, and inner hairline. The
same landmark points were placed on corresponding locations on
the average face. Previous studies show high reliability of placing
points on facial landmarks (see Koehler, Simmons, Rhodes, & Peters,
2004; Simmons, Rhodes, Peters, & Koehler, 2004). Each “low-average” face (Fig. 1a) was created by warping its standardized original
face 50% away from the average face (i.e., increasing the distance of
each landmark point from its corresponding position on the average
face by 50%) and remapping all texture information (brightness values) from the standardised original face into corresponding locations in this new configuration. This new configuration is called “low
average” because it has a high deviation from the average. A
a)
b)
50% toward average
c)
d)
FIGURE 1. a) A low-average version, b) the original face, c) a high-average version, and d) the average male face. See text for a detailed explanation
of the morphing procedure. Note only the low- and high-average versions of each individual’s face were used in the experiment.
50% away from average
646
KOEHLER ET AL.
FACE PREFERENCES AND THE MENSTRUAL CYCLE
a)
647
b)
FIGURE 2. A symmetry pair, consisting of a) lowand b) perfect-symmetry versions of the same face.
“high-average” face (Fig. 1c) was created in a similar way except that
the standardized original face was warped toward the average by
50%, so that the standardized original had a low deviation away
from the average. The average face was used only to create the lowand high-average versions of each face and was not shown to participants.
Symmetry Set. The symmetry pairs consisted of a low- and a perfect-symmetry version of each individual’s face for a total of 24 individuals (see Fig. 2). Sixteen of these pairs were taken from Rhodes,
Proffit, Grady, and Sumich (1998), and the remaining pairs were created using the same procedure. Gryphon’s Morph software was
used to create low- and perfect-symmetry versions of each face. To
create a perfectly symmetric face, landmark points were placed on
the original face and its mirror image. A perfectly symmetric face
was created by morphing together the original faces and their mirror
images. A low-symmetry face was created by warping the original
face 50% away from the perfect-symmetry face and then remapping
the original texture information into this new configuration.
648
KOEHLER ET AL.
PROCEDURE
Face pairs from the health, averageness, and symmetry sets (N = 72)
were presented in random order. For each set, the low version appeared on the left side of the screen on half the trials and on the right
side of the screen on the other half. Participants were asked to choose
which face they would prefer as a sexual partner. Each pair remained
visible until the participant responded. SuperLab software controlled presentation of stimuli and recorded responses on a
Macintosh computer.
At recruitment, participants reported the date of onset of their last
menstrual period, average cycle length, use of oral/hormonal contraceptives, and age. Participants were asked to contact the experimenter on the first day of menses to arrange a test session. The best
times to conceive are no more than 72 hours prior to ovulation and no
later than 24 hours after ovulation because most sperm can survive
for 48 hours inside the female’s reproductive tract, with some being
able to survive 72 hours, and the ovum being viable for the first 12–24
hours after ovulation (Hyde & Delamater, 1997; Marieb, 1995). Two
test sessions, one early–cycle (days 1–7, low conception risk) and one
mid–cycle (days 10–15, high conception risk in women with a natural
cycle only), were arranged with each participant. Test sessions were
based on the assumption that ovulation occurs 14 days prior to the
onset of menses in women with a natural cycle (reviewed in Zuspan
& Zuspan, 1979). Day 1 refers to the first day of onset of menses. The
mean ± SD days participants were tested on early– and mid–cycle
were days 3.4 ± 1.0 (range 2–7) and 12.9 ± 1.1 (range 11–15), respectively, for those with a natural cycle, and days 2.9 ± 0.9 (range 1–5)
and 12.8 ± 1.0 (range 10–15), respectively, for pill users. These test
days coincide with the lowest (0.000–0.018) and highest (0.085 –
0.073) probabilities of conception taking place following one act of
unprotected sex in women with a regular menstrual cycle during
days 2–7 and days 11–15, respectively, with the highest probability
being on day 12 (Wilcox et al., 2001).
Half of the participants with a natural cycle and half of the participants on the pill were tested early in their cycle first, whereas the
other halves were tested mid–cycle first to prevent order effects. The
procedure was identical for both test sessions. The brief questions regarding participants’ average cycle length and the date of onset of
their last menstrual period were repeated at each test session to con-
FACE PREFERENCES AND THE MENSTRUAL CYCLE
649
firm that the predicted day of a test session corresponded with the actual day of a participant’s cycle.
RESULTS
The proportion of pairs for which women selected the high-health,
high-average, and perfect-symmetry face, respectively, were our
measures of health preference, averageness preference, and symmetry preference, respectively.
Before examining possible cyclic preference changes, planned
t–tests were performed to determine whether there was a general
preference (for all participants combined) for healthy, average, and
symmetric faces. We tested whether these proportions were significantly greater than 0.50 (random choices) at both early– and
midcycle test sessions. Bonferroni corrections were used to correct
for multiple comparisons (N = 6, critical p = .008). The health preference did not differ significantly from chance during early–cycle test
sessions (M ± SD; 0.483 ± 0.092), t101 = 1.88, p = .07, two–tailed, but was
significantly below chance during mid–cycle test sessions (M ± SD;
0.478 ± 0.098), t101 = 2.27, p = .03, two–tailed. However, the later difference was not robust to Bonferroni correction (N = 6), the effect size
was small (r = .22), and the 95% confidence interval (.459–.497) only
just excluded .50. As expected, the averageness preference was significantly greater than 0.50, for both test sessions, t101 = 65.06, p <
0.001, two–tailed (M ± SD; 0.932 ± 0.067, early–cycle), and t101 = 85.31,
p < .001, two–tailed, (M ± SD; 0.941 ± 0.052, mid–cycle). Also as expected, the symmetry preference was significantly greater than
chance for both test sessions, t101 = 17.30, p < .001, two–tailed, (M ± SD;
0.763 ± 0.153, early–cycle), and t101 = 17.26, p < .001, two–tailed (M ±
SD; 0.769 ± 0.157, mid–cycle). Although high, the averageness preference was significantly below ceiling for both test sessions, t101 = 10.21,
p < .001, one–tailed, (early–cycle), and t101 = 11.37, p < .001, one–tailed,
(mid–cycle).
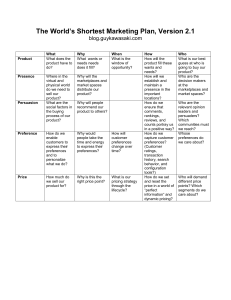
To test for cyclic changes in preferences, we conducted separate
two-way ANOVAs for each type of pair (health, averageness, symmetry), with participant group (natural cycle, pill) as a between-subjects factor and test session (early–cycle, mid–cycle) as a
repeated-measures factor (Fig. 3). (A preliminary analysis with test
order as a factor showed no significant main effects or interactions.)
Age of participant was included as a covariate because the natural
650
KOEHLER ET AL.
cycle and pill groups showed a small but significant difference in
age. There was no significant interaction between group and test session for health pairs, ANOVA: F1, 98 = 0.34, p = .56; averageness pairs,
ANOVA: F1, 98 = 0.10, p = .75; or symmetry pairs, ANOVA: F1, 98 = 0.19,
p = .67. There were no significant main effects. We also conducted
separate one–way ANOVAs for each type of pair (health,
averageness, symmetry) for participants with a natural cycle, with
test session (early–cycle, mid–cycle) as a repeated-measures factor
and age of participant as a covariate. No significant changes in preference were found for health, ANOVA: F1, 49 = 0.003, p = .95;
averageness, ANOVA: F1, 49 = 0.42, p = .52; or symmetry pairs,
ANOVA: F1, 49 = 0.05, p = .83.
DISCUSSION
We found no evidence that preferences for the facial cues to
long–term health examined here emerged or increased when conception was likely. Kalick et al. (1998) found no preference in women
whose conception risk was unknown for the faces of men with better
health histories, even though those faces were perceived to look
healthier. Using faces from the same database, we found no evidence
that a preference for the healthier faces emerged when conception
was likely. Nor did preferences for facial averageness and symmetry,
two other putative cues to long–term health, increase when conception was likely. The failure to find an increase in symmetry preference replicates Koehler et al. (2002). These results suggest that the
increased preference for masculine faces that occurs when conception is likely is not part of a general increase in preferences for cues to
immunocompetence and long–term health.
Two recent studies have reported a cyclic change in preference for
apparent health in faces (Jones, Little, Boothroyd, DeBruine,
Feinberg, Law Smith, 2005; Jones, Perrett, Little, Boothroyd,
Cornwell, Feinberg, 2005). However, this change does not appear to
target genetic benefits for offspring because the preference increases
after ovulation. Rather, as the authors note, it may be an adaptation
for avoiding infection in the early stages of pregnancy, when immune function is depressed, that operates by detecting cues to current ill health in faces. Consistent with this interpretation, the
preference also increases during pregnancy (Jones, Perrett, et al.,
2005).
FACE PREFERENCES AND THE MENSTRUAL CYCLE
651
Mean proportion of high-health/high-average/perfect-symmetry faces chosen
1.0
Early-cycle
Mid-cycle
0.9
0.8
0.7
0.6
0.5
0.4
Natural cycle
Health
Pill
Natural cycle
Pill
Averageness
Natural cycle
Pill
Symmetry
Face Set and Participant Group
FIGURE 3. Mean proportion of high-average, perfect-symmetry and high-health faces
preferred by women with natural cycles (N = 50) and pill users (N = 52) during early- and
mid-cycle test sessions. SE bars are shown.
It is possible that we would have obtained different results with a
different sample of faces or with color images. The advantages of our
health–set sample are that objective health histories were available
and that good health likely reflects disease resistance because these
individuals grew up before vaccinations and antibiotics were used.
Therefore, if a preference for relatively healthy faces emerged when
conception was likely, it would be strong evidence of an adaptation
for obtaining genetic benefits for offspring. A disadvantage of our
sample is that only black-and-white images were available and skin
color is certainly an important cue to health, particularly current
health (Jones, Little, Feinberg, Tiddeman, Penton-Voak, & Perrett,
2004). However, we do not believe this to be a serious limitation because our focus was on preferences for cues to long–term health during development, which affects facial structure (e.g., deviations from
averageness or symmetry) and skin texture (e.g., pock marks, scarring), both of which are visible in black-and-white images. Not surprisingly, we found the usual preferences for facial averageness and
symmetry. Therefore, we think it is unlikely that our failure to find
cyclic variation is due to the use of black-and-white images.
652
KOEHLER ET AL.
Could our failure to find cyclic effects reflect failure to test when
conception is likely? We think not, because we used more stringent
criteria for determining the fertile phase than most previous studies
reporting cyclic effects. All participants had a normal cycle length,
and the fertile phase was restricted to days 11–15, which show the
highest probability of conception taking place following one incident of unprotected sex (Wilcox et al., 2001). The likelihood of conception on these days ranges from 0.073 to 0.094, whereas the lower
bound was much lower in other studies (0.004 in Rikowski &
Grammer, 1999; 0.009 in Gangestad & Thornhill, 1998; Penton–Voak
& Perrett, 2000; Thornhill & Gangestad, 1999b).
Our failure to find cyclic effects is also unlikely to reflect failure to
test when conception was unlikely. Our low conception risk test days
(2–7) have extremely low conception probabilities (0.000–0.018,
Wilcox et al., 2001). Previous studies have generally included all
nonfertile days in their low conception risk groups, thereby including days with conception probabilities as high as 0.073 (Gangestad &
Thornhill, 1998; Penton–Voak & Perrett, 2000; Thornhill &
Gangestad, 1999b) and 0.047 (Rikoski & Grammer, 1999), which are
higher than some of the high conception risk days.
Cyclic changes may be greater in the context of short–term than
long–term partner choices (Jones, Little, et al., 2005; Johnston et al.,
2001; Penton–Voak et al., 1999), although they are certainly not restricted to such contexts (Gangestad & Thornhill, 1998; Johnston et
al., 2001; Penton–Voak et al., 1999; Rikowski & Grammer, 1999;
Thornhill & Gangestad, 1999b). This raises the question of whether
cyclic changes in the preferences examined here would emerge in
the context of short–term mate choice. This is possible, although in
a previous study we found no cyclic effect on symmetry preferences for either short–term or long–term partners (Koehler et al.,
2002). Furthermore, the substantial direct benefits associated with
healthy partners (e.g., reduced risk of infection, greater potential to
provide resources and parental care) raise the question of why preferences for healthy mates would be restricted to short–term contexts. We suggest that restricted preferences may occur only when
there are costs to associating with the preferred individuals, as appears to be the case for masculine males (Penton–Voak et al., 1999;
Perrett, Lee, Penton-Voak, Rowland, Yoshikawa, Burt et al., 1998).
These costs could explain why cyclic changes in preferences for relatively masculine faces are greater for short–term partners and also
FACE PREFERENCES AND THE MENSTRUAL CYCLE
653
why the masculinity preference changes over the menstrual cycle.
More generally, the lack of such costs may explain the absence of
variation in preferences for the cues to long–term health examined
here.
Since our study was conducted, Jones and colleagues have reported that a preference for masculine faces is stronger mid–cycle
(high conception risk) than late–cycle and that masculinity preferences were related to changes in progesterone levels, which occur
mid–late cycle (Jones, Little, et al., 2005). It is possible, therefore, that
cyclic changes in masculinity preferences identified in studies that
classify both early– and late–cycle preferences as low conception risk
(see above) come solely from a mid–late–cycle reduction rather than
an early–mid–cycle increase in the preference. This hypothesis could
be tested directly by comparing early–, mid– and late–cycle masculinity preferences. It is an open question whether the preferences examined here show a similar pattern. Future studies could test
whether preferences for average and symmetric faces decrease after
ovulation. We note, however, that failure to test after ovulation is unlikely to explain the absence of variation in preferences for our
healthier faces because these faces were not preferred at ovulation.1
In summary, we found no evidence for cyclic changes in preferences for the facial cues to long–term health examined here. The
only cyclic change in visual preferences that seems likely to be an
adaptation for obtaining genetic benefits for offspring remains the
increased preference for masculine faces when conception risk is
high. The cyclic change reported recently in preference for apparent health in faces appears to be an adaptation for avoiding contagion rather than for obtaining genetic benefits for offspring (Jones,
Little, et al., 2005; Jones, Perrett, et al., 2005). Taken together, these
findings suggest that visual preferences that can obtain genetic benefits for offspring may increase when conception is likely only if
there are costs to associating with the preferred individuals, as may
be the case for masculine–looking male faces.
1. There was actually a small bias against healthy faces mid-cycle (for all participants
combined), but this did not survive Bonferroni correction. Nor was there any significant
difference in health preference between mid-cycle and early-cycle test sessions. Given that
the health pairs were matched on initial attractiveness, the small bias against healthy faces
in one of the test sessions likely reflects random variation between samples of raters.
654
KOEHLER ET AL.
REFERENCES
Folstad, I., & Karter, A. J. (1992). Parasites, bright males and the
immunocompetence handicap. American Naturalist, 139, 603–622.
Gangestad, S. W., & Thornhill, R. (1997). Human sexual selection and developmental stability. In J. A. Simpson & D. T. Kenrick (Eds.), Evolutionary social
psychology (pp. 169–196). Hillsdale, NJ: Lawrence Erlbaum Associates, Inc.
Gangestad, S. W., & Thornhill, R. (1998). Menstrual cycle variation in women’s
preferences for the scent of symmetry men. Proceedings of the Royal Society
of London: Series B, 265, 927–933.
Hyde, J. S., & Delamater, J. D. (1997). Understanding human sexuality (6th ed.).
Boston, MA: McGraw–Hill.
Johnston, L., Arden, K., Macrae, C. N., & Grace, R. C. (2003). The need for speed:
The menstrual cycle and person construal. Social Cognition, 21, 89–100.
Johnston, V. S., Hagel, R., Franklin, M., Fink, B., & Grammer, K. (2001). Male facial attractiveness: Evidence for hormone–mediated adaptive design. Evolution and Human Behavior, 22, 251–267.
Jones, B. C., Little, A. C., Boothroyd, L., DeBruine, L. M., Feinberg, D. R., Law
Smith, M. J., et al. (2005). Commitment to relationships and preferences for
femininity and apparent health in faces are strongest on days of the menstrual cycle when progesterone level is high. Hormones and Behavior, 48,
283–290.
Jones, B. C., Little, A. C., Feinberg, D. R., Tiddeman, B. P., Penton–Voak, I. S., &
Perrett, D. I. (2004). The relationship between shape symmetry and visible
skin condition in male facial attractiveness. Evolution and Human Behavior,
25, 24–30.
Jones, B. C., Perrett, D. I., Little, A. C., Boothroyd, L., Cornwell, R .E., Feinberg, D.
R. et al. (2005). Menstrual cycle, pregnancy and oral contraceptive use alter
attraction to apparent health in faces. Proceedings of the Royal Society of London, Series B, 272, 347–354.
Kalick, S. M., Zebrowitz, L. A., Langlois, J. H., & Johnson, R. M. (1998). Does human facial attractiveness honestly advertise health? Longitudinal data on
an evolutionary question. Psychological Science, 9, 8–13.
Koehler, N., Rhodes, G., & Simmons, L. W. (2002). Are human female preferences for symmetrical male faces enhanced when conception is likely? Animal Behaviour, 64, 233–238.
Koehler, N., Simmons, L. W., Rhodes, G., & Peters, M. (2004). The relationship
between sexual dimorphism in human faces and fluctuating asymmetry.
Proceedings of the Royal Society of London, Series B (Suppl.), 271, S233–S236.
Langlois, J., Kalakanis, L., Rubenstein, A.J., Larson, A., Hallam, M., & Smoot, M.
(2000). Maxims or myths of beauty? A meta–analytic and theoretical review. Psychological Bulletin, 126, 390–423.
Macrae, C. N., Alnwick, K. A., Milne, A. B., & Schloerscheidt, A. M. (2002). Person perception across the menstrual cycle: Hormonal influences on social–cognitive functioning. Psychological Science, 13, 532–536.
FACE PREFERENCES AND THE MENSTRUAL CYCLE
655
Marieb, E. N. 1995. Human anatomy and physiology (3rd ed.). Redwood City, CA:
The Benjamin/Cummings Publishing Company.
Penton–Voak, I. S., & Perrett, D. I. (2000). Woman preference for male faces
changes cyclically: Further evidence. Evolution and Human Behavior, 21,
39–48.
Penton–Voak, I. S., Perrett, D. I., Castles, D. L., Kobayashi, T., Burt, D. M., Murray
L. K. et al. (1999). Menstrual cycle alters face preference. Nature, 388,
741–742.
Perrett, D. I., Lee, K. J., Penton–Voak, I., Rowland, D., Yoshikawa, S., Burt, D. M.,
et al. (1998). Effects of sexual dimorphism on facial attractiveness. Nature,
394, 884–887.
Rhodes. G. (2006). The evolution of facial attractiveness. Annual Review of Psychology, 57, 199–226.
Rhodes, G., Chan, J., Zebrowitz, L. A., & Simmons, L. W. (2003). Does sexual dimorphism in human faces signal health? Proceedings of the Royal Society of
London, Series B (Suppl.), 270, S93–S95.
Rhodes, G., Proffitt, F., Grady, J. M., & Sumich, A. (1998). Facial symmetry and
the perception of beauty. Psychometric Bulletin and Review, 5, 659–669.
Rhodes, G., & Simmons, L. (in press). Symmetry, attractiveness and sexual selection. In R. Dunbar & L. Barrett (Eds.), The Oxford handbook of evolutionary
psychology. Oxford: Oxford University Press.
Rhodes, G., Sumich, A., & Byatt, G. (1999). Are average facial configurations attractive only because of their symmetry? Psychological Science, 10, 52–58.
Rhodes, G., & Zebrowitz, L. A. (2002). Facial attractiveness: Evolutionary, cognitive,
and social perspectives. Westport, CT: Ablex.
Rhodes, G., Zebrowitz, L. A., Clark, A., Kalick, S. M., Hightower, A., & McKay, R.
(2001). Do facial averageness and symmetry signal health? Evolution & Human Behavior, 22, 31–46.
Rikowski, A., & Grammer, K. (1999). Human body odour, symmetry and attractiveness. Proceedings of the Royal Society of London: Series B, 266, 869–874.
Simmons, L. W., Rhodes, G., Peters, M., & Koehler, N. (2004). Are human preferences for facial symmetry focused on signals of developmental instability?
Behavioral Ecology, 15, 864–871.
Slater, A., Quinn, P.C., Hayes, & Brown, E. (2000). The role of facial orientation in
newborn infants’ preference for attractive faces. Developmental Science, 3,
181–185.
Slater, A., Van der Schulenberg, C., Brown, E., Badenoch, M., Butterworth, G.,
Parsons, S., et al. (1998). Newborn infants prefer attractive faces. Infant Behavior and Development, 21, 345–354.
Symons, D. (1979). The evolution of human sexuality. Oxford: Oxford University
Press.
Thornhill, R., & Gangestad, S. W. (1993). Human facial beauty: Averageness,
symmetry, and parasite resistance. Human Nature, 4, 237–269.
Thornhill, R., & Gangestad, S.W. (1999a). Facial attractiveness. Trends in Cognitive Sciences, 3, 452–460.
656
KOEHLER ET AL.
Thornhill, R., & Gangestad, S. W. (1999b). The scent of symmetry: A human sex
pheromone that signals fitness? Evolution and Human Behavior, 20, 175–201.
Wilcox, A. J., Dunson, D. B., Weinberg, C. R., Trussell, J., & Baird, D. D. (2001).
Likelihood of conception with a single act of intercourse: Providing benchmark rates for assessment of post–coital contraceptives. Contraception, 63,
211–215.
Zuspan, K. J., & Zuspan, F. P. (1979). Basal body temperature. In E. S. E. Hafez
(Ed.), Human ovulation. (pp. 291–298). Amsterdam: Elsevier/North–Holland Biomedical Press.