Brandeis University - Qualified Status Change Form
advertisement

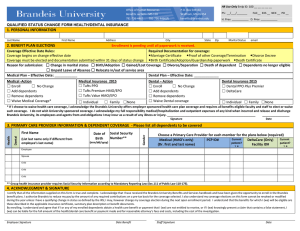
Brandeis University - Qualified Status Change Form 1. PERSONAL INFORMATION 1. Please make sure your address is updated in Brandeis University Self Service (BUSS). The HOME address is what is used and sent to the vendors. 2. If you do not know your current health or dental plan you can log on to BUSS and find it under Benefit Summary in Self Service (https://www.brandeis.edu/buss/). 2. BENEFIT PLAN ELECTIONS 1. Check off the type of Qualifying Event – Please submit Required Documentation with the form 2. Effective date is the event date. 3. Choose a health and/or dental plan and level of coverage. 4. If waiving coverage please sign acknowledgement that employer sponsored coverage was offered and waived. 3. PRIMARY CARE PROVIDER INFORMATION & DEPENDENT COVERAGE 1. Required Documentation for family coverage: Marriage Certificate, Birth Certificate or Adoption/Guardianship paperwork. 2. List ALL individuals to be COVERED under the medical and/or dental plan including your legal spouse, children under age 19, children age 19-26 who do not have coverage as an employee or dependent under his/her spouse’s employer sponsored plan. 3. Social Security Numbers are required for all dependents enrolled under your plan. 4. Primary Care Provider Medical: If you choose the Premium or Value HMO/EPO plan a Primary Care Physician (PCP) is required, it is important that you select one right away. Until we know who your PCP is, your in-network benefits may be limited to emergency services only. To find a PCP, visit tuftshealthplan.com and use the Doctor Search feature selecting the Standard network. On this application, indicate whether you are an established patient of the PCP you have listed. 5. Primary Care Provider Dental: If you choose the DeltaCare dental plan you must choose a DeltaCare Primary Care Dentist (PCD) visit deltadentalma.com, use the find a dentist feature and select a dentist from the DeltaCare network or call DeltaCare member services at 800-327-6277. 4. ACKNOWLEDGEMENT AND SIGNATURE 1. Sign and date form. Please note university email is not encrypted; therefore you should not send this form back over email for your safety and security. You may drop off to our office, fax or send via campus mail. MS 118 Fax: 781-736-4466 Office: Bernstein-Marcus 2nd Flr Office of Human Resources Benefits section – MS 118 781-736-4467 781-736-4466(f) HR Use Only Emlp ID: 100 __ __ __ __ __ P.O. Box 549110 Waltham, MA 02454 benefits@brandeis.edu PS: __/___/_______ FAC__ EXS __ NEX __ PD __ H. Prev. ___________ D. Prev. ___________ QUALIFIED STATUS CHANGE FORM HEALTH/DENTAL INSURANCE 1. PERSONAL INFORMATION Last Name First Name Address City State Zip Marital Status email 2. BENEFIT PLAN ELECTIONS Enrollment is pending until all paperwork is received. Coverage Effective Date Rules: Required Documentation for coverage: Coverage begins on change effective date Marriage Certificate Proof of other Coverage/Termination Divorce Decree Coverage must be elected and documentation submitted within 31 days of status change Birth Certificate/Adoption/Guardianship paperwork Death Certificate Reason for submission: ☐ Change in marital status ☐ Birth/Adoption ☐ Gained/Lost Coverage ☐ Divorce/Separation ☐ Death of dependent ☐ Dependents no longer eligible ☐ Unpaid Leave of Absence ☐ Relocate in/out of service area Medical Plan – Effective Date: ____________ Dental Plan – Effective Date: _____________ Medical -Action ☐ Enroll ☐ No Change ☐ Add dependents ☐ Remove dependents ☐ Waive Medical Coverage* Medical Insurance ☐ Tufts PPO ☐ Tufts Premium HMO/EPO ☐ Tufts Value HMO/EPO ☐ Individual Dental – Action ☐ Enroll ☐ No Change ☐ Add dependents ☐ Remove dependents ☐ Waive Dental coverage ☐ Family ☐None Dental Insurance ☐ Dental PPO Plus Premier ☐ DeltaCare ☐ Individual ☐ Family ☐None * If I choose to waive health care coverage, I acknowledge the Brandeis University offers employer sponsored health care plan coverage and requires all benefits eligible faculty and staff to elect or waive such coverage. I do not wish University sponsored coverage. I acknowledge my full responsibility medical/hospitalization and outpatient expenses of any kind when incurred and release and discharge Brandeis University, its employees and agents from and obligations I may incur as a result of any illness or injury. Dental Health First Name (List last name only if different from employee’s last name) Date of Birth Social Security Number** (mm/dd/yyyy) Gender 3. PRIMARY CARE PROVIDER INFORMATION & DEPENDENT COVERAGE - Please list all dependents to be covered Choose a Primary Care Provider for each member for the plans below (required) Current Current Medical (HMO’s only) PCP ID# DeltaCare (Only) patient? patient? (Dr. first and last name) Facility ID# Y N Y N Employee Spouse Child Child Child ** Group health insurance provider requires Social Security Information according to Mandatory Reporting Law (Sec.111 of Public Law 110-173). 4. ACKNOWLEGMENT & SIGNATURE I certify that all the information supplied on this form is true and complete. I acknowledge that I have received the Brandeis University Benefits and Services handbook and have been given the opportunity to enroll in the Brandeis benefit plans. I authorize Brandeis to reduce my pay by the amount of any required contributions on a pre-tax basis for the coverage selected. I also understand my coverage elections on this form cannot be revoked or modified during the year unless I have a qualifying change in status as defined by the IRS; I may, however change my coverage election during the next open enrollment period. I understand that the benefits for which I (we) will be eligible are those described in the applicable insurance certificate, summary plan description or benefit documents. By enrolling, I understand and agree that if I or any of my enrolled dependents obtain a health care benefit or payment that I (we) are not entitled to receive, or if I (we) knowingly present a claim that contains a false statement, I (we) can be liable for the full amount of the health/dental care benefit or payment made and for reasonable attorney’s fees and costs, including the cost of the investigation. Employee Signature Date Benefit Staff Signature Date