C-SPINE T-SHEET
advertisement

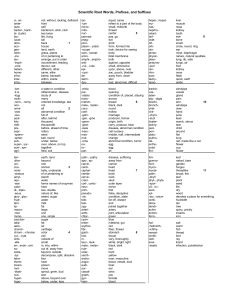
C-SPINE T-SHEET CC: Neck Pain R Upper Extremity Pain R HPI: Onset: Mechanism of injury: Location: Radiation: Yes Pain at Rest: Yes Exacerbating factors: Relieving factors: L L No No ROS: Fever Chills Weakness Night Pain PMHx: Meds: Allergies: Chronic medical conditions: Immunizations Current: Both Both Where: Where: Numbness Paresthesias Weight Loss Amount_________ Yes No Soc Hx: Occupation and/or Activities: Smoking status: Current Past Never IV Drug Use: Yes No PE: Vital Signs: BP: P: Wt: BMI: RR: General Appearance: Skin: Vascular: Neuro: ROM: Soft Tissue: (Palpation) Redness Yes Warmth Yes Ecchymosis Yes Deformity Yes Ulcers Yes Distal Hair pattern: No Location: No Location: No Location: No Location: No Location: Normal Decreased Right Capillary Refill: Radial Pulse: Left Nl Abnormal Nl Abnormal Spurling’s Maneuver: Nl Abnormal Nl Absent Brachioradialis Reflex (C5): Bicep Reflex (C6): Nl Absent Tricep Reflex (C7): Nl Absent Hoffman Test: Nl Abnormal Babinski Reflex: Nl Abnormal Position Sense: Nl Abnormal Nl Abnormal Nl Abnormal Nl Abnormal Nl Absent Nl Absent Nl Absent Rotation: Nl Painful Flexion: Nl Painful Extension: Nl Painful Tenderness: Yes No Location: Vertebral Tenderness: Yes No Cervical Lymphadenopathy: Yes No Location: Location: Nl Abnormal Nl Abnormal Nl Abnormal Nl Painful Nl Painful Nl Painful TREAT APPROPRIATELY TREAT WITH CLOSE FOLLOW-UP Cervical Myelopathy ............................................. 721.1 Degenerative Disc Disease .................................... 722.4 Mechanical Pain/Benign Neck Pain ...................... 723.1 Mild Radicular Symptoms .................................... 723.4 Whiplash Associated Disorder .............................. 847.0 Severe pain Narcotics prescribed (< 1 week f/u) CALL CONSULTANT THAT DAY CONSULT OR REFER Fracture X-ray negative, but tender bony prominence or neurologic signs Meningitis Suspect myelopathy Other positive X-ray findings History of C-spine surgery with recurrent symptoms Plan: Xray / imaging Laboratory eval NSAIDs Acetaminophen Other PRICE Protocol Physical Therapy Disposition: Treatment initiated: Follow-up __________ weeks Treatment / work up initiated: Follow-up ≤ 1 week __________ days Immediate call to Dr. Consultation initiated with Dr. Referral to Dr.