Original Article
Mifepristone: Effect on Plasma Corticotropin-Releasing Hormone,
Adrenocorticotropic Hormone, and Cortisol in Term Pregnancy
James D. Byrne, MD
Deborah A. Wing, MD
Mhoyra Fraser, PhD
Michael J. Fassett, MD
T. Murphy Goodwin, MD
John R.G. Challis, PhD, Dsc
OBJECTIVE:
To compare the effects of in vivo mifepristone with placebo on plasma
corticotropin-releasing hormone (CRH), adrenocorticotropic hormone
(ACTH), and cortisol levels concentrations in term human pregnancies.
STUDY DESIGN:
In all, 24 women participating in a randomized controlled trial of
mifepristone for preinduction cervical ripening were enrolled in this
ancillary study. Participants with uncomplicated singleton pregnancies
beyond 41 weeks gestation and undilated, uneffaced cervices were
randomized to either placebo or mifepristone 200 mg orally and observed
for 24 hours prior to receiving either intravaginal misoprostol and/or
intravenous oxytocin. Blood samples were obtained before medication
administration, 3 and 6 hours later, and then every 6 hours until delivery.
Plasma hormone levels were measured by radioimmunoassay.
RESULTS:
Basal levels of CRH, ACTH, and cortisol were similar in the placebo
(n ¼ 13) and mifepristone groups (n ¼ 11). Compared to placebo
treatment, exposure to mifepristone resulted in significant elevation of
plasma cortisol within 18 hours. Plasma CRH and ACTH were unaffected.
Progression of labor was associated with significant increases in cortisol
in both groups, while CRH and ACTH levels were not altered. Compared to
basal levels within each group, plasma cortisol at delivery was
Division of Maternal Fetal Medicine, (J.D.B., D.A.W., M.J.F., T.M.G.), Department of Obstetrics
and Gynecology, University of Southern California Keck School of Medicine, Los Angeles, CA, USA;
Liggins Institute for Medical Research (M.F.), Faculty of Medicine and Health Science, University
of Auckland, Auckland, New Zealand; and Departments of Physiology and Obstetrics and
Gynaecology (J.R.G.C.), University of Toronto, MRC Group In Fetal and Neonatal Health and
Development, Toronto, Ontario, Canada.
This work was supported by the Department of Obstetrics and Gynecology, University of Southern
California School of Medicine and by MRC (CIHR) Canada Group Grant in Fetal and Neonatal
Health and Development.
Address correspondence and reprint requests to James D. Byrne, MD, Department of Obstetrics
and Gynecology, Santa Clara Valley Medical Center, 751 South Bascom Avenue, San Jose, CA
95128, USA.
significantly elevated within both the mifepristone (156.8±17.7 vs
332.6±48.5 ng/ml, p ¼ 0.008) and the placebo (166.6±34.3 vs
342.4±46.4 ng/ml, p ¼ 0.003) groups. However, plasma CRH, ACTH, and
cortisol levels at delivery did not differ between the groups.
CONCLUSION:
Mifepristone exposure and induced labor were associated with significant
increases in plasma cortisol without alterations of systemic CRH or ACTH
levels.
Journal of Perinatology (2004) 24, 416–420. doi:10.1038/sj.jp.7211127
Published online 20 May 2004
INTRODUCTION
Despite intensive basic and clinical research, the factors regulating
the duration of pregnancy and the onset of labor are poorly
understood. Labor is initiated by a complex confluence of endocrine
and paracrine mechanisms.1–3 In many mammals, parturition is
preceded by elevation of fetal cortisol, which increases the
expression of placental 17-a-hydroxylase/17,20-lyase. This results
in progesterone withdrawal and enhanced estrogen output.1,3
Multiple parturition pathways are then activated that increase
prostaglandins, oxytocin sensitivity, and calcium channels before
culminating in labor. In contrast, humans lack placental 17-ahydroxylase/17,20-lyase activity. Therefore, systemic progesterone
withdrawal does not occur prior to human labor despite an
equivalent involvement of these same parturition pathways.3
Alternate models suggest that a functional withdrawal of local
progesterone may occur at the placenta, thus initiating labor
through the pathways mentioned above without altering
circulating progesterone.3,4 In vitro research using term human
placentas suggests that the increased cortisol levels associated with
impending labor competitively block the inhibitory action of
progesterone in regulating trophoblastic corticotropin-releasing
hormone (CRH) messenger RNA, resulting in increased CRH
levels.4 Karalis noted a similar elevation in CRH following
mifepristone exposure, which was attributed to antagonism of the
progesterone/glucocorticoid receptor. Karalis’s theory of functional
progesterone withdrawal correlates with extensive in vitro evidence
that placental CRH expression is inhibited by progesterone and
stimulated by glucocorticoids.3,5–8 This has led to the speculation
that a positive feedback loop involving cortisol and CRH may be
involved in labor.
Journal of Perinatology 2004; 24:416–420
r 2004 Nature Publishing Group All rights reserved. 0743-8346/04 $30
416
www.nature.com/jp
Mifepristone in Term Pregnancy
The report by Karalis provides an in vitro experimental model of
human labor in which exposure to mifepristone results in local
placental CRH elevation in a manner similar to what may
naturally occur following competitive inhibition of progesterone by
cortisol. Our objective was to assess this model in vivo by observing
systemic plasma CRH, adrenocorticotropic hormone (ACTH), and
cortisol levels after mifepristone exposure.
MATERIALS AND METHODS
This was an ancillary study to a randomized placebo-controlled
trial evaluating mifepristone for preinduction cervical ripening.9
The study was performed at the University of Southern California
School of Medicine.
Women who met the criteria for entry and exclusion were
invited to participate. Entry criteria were singleton gestation,
cephalic presentation, intact membranes, gestational age more
than 41 weeks by good dates, and reassuring fetal heart rate
patterns. Exclusion criteria were Bishop score greater than 6, more
than nine uterine contractions per hour, parity of six or more,
prior uterine surgery, contraindications to prostaglandins, or
evidence of complications such as infection, hypertension,
intrauterine growth restriction, macrosomia, and vaginal bleeding.
The primary study of preinduction cervical ripening was double
masked and these methods have been reported previously.9 Briefly,
subjects received a single dose of either mifepristone 200 mg or
placebo (ascorbic acid) by mouth. Following administration of the
medication, subjects were observed with continuous external
electronic fetal monitoring for 24 hours. At the end of this
observation period, women were re-evaluated and labor induction
was continued with misoprostol or oxytocin according to the study
protocol.9
Maternal venous blood was obtained prior to study medication
administration (time 0 hours), at 3 hours, at 6 hours, and then
every 6 hours until the final collection at delivery. The women were
randomly chosen among eligible study candidates for participation
in this adjunct. Blood was drawn into chilled heparinized tubes
and immediately centrifuged at 2000 g revolutions/minute for
12 minutes at 41C. Plasma was separated into equal aliquots and
stored at 701C until batched extraction and assay.
The primary outcome measures were plasma hormones CRH,
ACTH, and cortisol. Plasma CRH was measured by
radioimmunoassay (RIA) as described by Marinoni et al.8 The
lower limit of detection of the assay was 4.3 pmol/l and the intraand interassay coefficients of variation were 6.5 and 12%,
respectively. ACTH was measured with a commercial RIA kit
(Incstar, Stillwater, MI) with an interassay coefficient of variation
of 10.6%. Cortisol was measured by RIA as reported previously.8
The interassay coefficient of variation was 11%.
Sample size of was determined on the basis of data
demonstrating a two-fold increase in CRH values following
Journal of Perinatology 2004; 24:416–420
Byrne et al.
mifepristone exposure in vitro.4 We hypothesized that the in vivo
response would be less robust, and estimated that a minimum
sample of nine women in each group would be adequate to detect
an 80% differences in the mean plasma CRH level with a type I
error of 0.05 and a type II error of 0.2. The test was one
sided as prior in vivo and in vitro reports have never demonstrated
a decrease in CRH values after exposure to mifepristone.
Hormone results are expressed as mean±SEM. Owing to high
individual variation, maternal plasma CRH values were also
evaluated as the mean percent change from basal levels. Statistical
analysis was performed with SPSS for Windows version 6.1.4 (SPSS
Inc., Chicago, IL). Comparisons between normally distributed
variables were performed with unpaired t-tests. As hormone levels
were not normally distributed, comparisons between groups were
performed using Mann–Whitney U-tests and within-group
comparisons were made with Wilcoxon’s matched-pairs tests.
Tests were two sided with p<0.05 statistically significant. An
Investigational New Drug Application was filed with the
Food and Drug Administration under the preinduction
cervical ripening study. The institutional review board approved
both studies. Written informed consent was obtained for each
protocol.
RESULTS
In all, 24 women were enrolled: 13 received placebo and 11
received mifepristone. The two groups were similar with respect to
maternal age, parity, gestational age, and birth weight (Table 1).
The two groups were also similar with regard to intrapartum events
such as misoprostol use and oxytocin administration, as well as
route of delivery (Table 1). At enrollment, the mean baseline CRH
level for all subjects was 3.8±0.3 ng/ml, mean ACTH was
30.1±4.7 pg/ml, and mean cortisol was 142.8±9.6 ng/ml. Baseline
levels were similar in both the placebo and mifepristone groups for
CRH (3.6±0.4 vs 4.0±0.5 ng/ml, p ¼ 0.67), ACTH (33.4±7.0 vs
26.1±6.1 pg/ml, p ¼ 0.32), and cortisol (133.5±10.9 vs
152.8±16.1 ng/ml, p ¼ 0.37).
All women receiving mifepristone delivered within 42 hours of
receiving the medication. Consequently, longitudinal comparisons
between groups were limited to the first 36 hours after drug
administration.
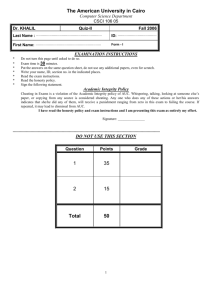
Plasma CRH levels were not altered by mifepristone exposure or
by labor. Compared to placebo, mifepristone exposure was not
associated with alterations in plasma CRH levels when analyzed as
either the mean value (Figure 1) or as the percentage change from
basal levels (not presented). No significant CRH alterations from
baseline levels occurred within the mifepristone group. Within the
placebo group, match-paired CRH levels did not change from basal
levels except for an isolated point at 18 hours. Progression of labor
and delivery were not associated with significant alterations in
plasma CRH levels.
417
Byrne et al.
Mifepristone in Term Pregnancy
Table 1 Maternal Characteristics
Age (years)
Parity
Gestational age (weeks)
Misoprostol use
Oxytocin use
Mean time from enrollment to active labor (minutes)
Mean time from enrollment to delivery
Route of delivery
Vaginal
Instrumented vaginal
Cesarean
Birth weight (g)
Placebo (n ¼ 13)
Mifepristone (n ¼ 11)
P-value
24.4±1.6
1 (0–3)
41.3±0.1
11/13 (84.6%)
6/13 (46.2%)
2026.2±238.2
2620.6±283.0
29.3±1.9
1 (0–5)
41.2±0.1
9/11 (81.8%)
4/11 (36.4%)
2179.5±211.4
2473.4±216.2
0.07a
0.24b
0.40a
0.85c
0.63c
0.51d
0.69d
7
4
2
3665±167
10
1
0
3780±130
0.12c
0.60a
Data presented as mean±SE the mean, median (range or n(5)).
a
Unpaired t-test.
b
Mann–Whitney U-test.
c 2
w test.
d
Based on log-transformed data.
Placebo
Mifepristone
40
CRH ( ng/mL)
ACTH (pg/mL)
50
30
20
6.0
5.5
10
*
5.0
4.5
4.0
3.5
3.0
0
3
6
12
18
Time (hr)
24
30
36
Figure 1. Longitudinal changes in plasma ACTH (top) and CRH
(bottom). Asterisk, Placebo group CRH level compared to baseline
p<0.05, Wilcoxon’s matched-pairs test. Points represent mean; error
bars represent SEM.
Plasma ACTH levels were not significantly altered by
mifepristone exposure, progression of labor, or delivery (Figure 1).
Plasma cortisol was significantly elevated following mifepristone
exposure. Compared to placebo-treated women, plasma cortisol
levels were significantly higher in the mifepristone-treated women
beginning 18 hours after administration (Figure 2). Within the
mifepristone group, matched-paired comparisons to basal levels
revealed that cortisol began to rise 12 hours after administration of
the medication. This increase was statistically significant at 18
hours and beyond. A similar trend was noted within the placebo
group, but this did not achieve statistical significance during the
first 36 hours of sampling.
418
In order to assess hormonal alterations associated with
labor, data were evaluated using delivery as a common
point of reference. Progression of labor was associated with
significant increases in plasma cortisol in both groups.
Mifepristone exposure was associated with higher levels of cortisol
during labor were compared to placebo (Figure 3). This difference
was statistically significant 24 hours (239.0±36.3 vs
153.5±17.7 ng/ml, p ¼ 0.04) and 6 hours (237.5±28.4 vs
171.5±25.72 ng/ml, p ¼ 0.04) prior to delivery. With-in-group
matched-paired comparisons to basal levels revealed that plasma
cortisol was significantly elevated at the time of delivery in both the
mifepristone group (156.8±17.7 vs 332.6±48.5 ng/ml, p ¼ 0.008)
and the placebo group (166.6±34.3 vs 342.4±46.4 ng/ml,
p ¼ 0.003).
Comparison between the mifepristone and placebo groups at
delivery noted similar plasma hormone levels for CRH (3.4±0.7 vs
4.3±0.7 ng/ml, p ¼ 0.36), ACTH (26.4±5.9 vs 30.9±5.6 pg/ml,
p ¼ 0.50), and cortisol (332.6±48.5 vs 342.4±46.4 ng/ml,
p ¼ 0.55).
SIGNIFICANCE
Our data with regard to plasma CRH, ACTH, and cortisol in late
pregnancy contributes to knowledge of endocrinology in pregnancy.
This research focus is currently receiving significant investment
due to wide clinical implications for maternal and fetal medicine.
These include elucidation of potential etiologies and management
options for diverse conditions, including preterm labor, intrauterine
growth restriction, maternal stress responses and depression, and
postnatal disease.3,10–12
Journal of Perinatology 2004; 24:416–420
Mifepristone in Term Pregnancy
Byrne et al.
350
*#
Placebo
Mifepristone
Cortisol (ng/mL)
275
*#
*#
*#
200
125
50
0
3
12
6
18
24
30
36
Time (hr)
Figure 2. Longitudinal changes in plasma cortisol. Pound sign,
placebo vs mifepristone p<0.05 by Mann–Whitney U-test. Asterisk,
mifepristone group cortisol level compared to baseline, p<0.05 by
Wilcoxon’s matched-pairs test. Points represent mean; error bars
represent SEM.
500
Placebo
Mifepristone
Cortisol (ng/mL)
400
300
200
*
100
#
*#
**
*
*
**
**
**
**
**
0
-42
-36
-30
-24
-18
-12
-6
-3
0
Time to Delivery (hr)
Figure 3. Changes in plasma cortisol in relation to delivery. Pound
sign, placebo vs mifepristone, p<0.05 by Mann–Whitney U-test.
Cortisol levels compared to delivery noted for Placebo group (double
asterisk) and mifepristone group (asterisk) with p<0.05 by Wilcoxon’s
matched-pairs test. Points represent mean; error bars represent SEM.
We noted baseline CRH levels at gestational age Z41 weeks
that were elevated compared to values reported for term
pregnancies, consistent with observations that placenta CRH
expression increases with advancing gestational age.13–15 CRH
levels varied widely between our subjects, a finding consistent with
other studies.5,14,16,17 Individual variation in plasma CRH levels in
pregnancy is not due to diurnal influences.15,18
Our study did not show elevations in systemic plasma CRH
following in vivo mifepristone and may indicate that the CRH
alterations observed by Karalis et al. in vitro occur only at a local
level. Neither plasma CRH nor ACTH was altered by mifepristone
exposure or by progression of labor. Our data corroborates studies
Journal of Perinatology 2004; 24:416–420
by Cooper et al.,19,20 who observed that human placental CRH and
ACTH immunostaining were not altered by oral mifepristone
administration in the first trimester or by term labor. Despite
progressive increases in CRH that peak prior to spontaneous labor,
our collective data support the hypothesis that labor itself can
progress without further increases in systemic CRH levels.13,14 Our
findings correlate with those of Florio et al.,17 who found no
increases in CRH levels in women in spontaneous labor. The same
conclusion is supported for ACTH, refuting reports that levels
increase with labor.21,22
Plasma cortisol increased significantly both with mifepristone
exposure and with labor. We acknowledge that these latter results
may be confounded by the subsequent administration of
misoprostol, and in approximately half of the subjects, oxytocin.
We were unable to analyze the influence of these two agents on
plasma cortisol levels independently, as there was only one subject
in the study who received neither oxytocin nor misoprostol. We
suggest that the rise in cortisol may be due to alterations in
placental cortisol metabolism, rather than to alterations in the
maternal hypothalamic-pituitary-adrenal (HPA) axis induced by
either mifepristone exposure or the ‘‘stress’’ of labor. It remains
possible that there are changes in the concentrations of ACTH in
maternal circulation during the course of labor that we cannot
detect using current methodology. In addition, mifepristone
exposure may have produced further subtle variations in ACTH that
have biological effect, but were undetectable with the sampling and
assay techniques we have used. This not withstanding, the lack of
evidence for alterations in CRH and/or ACTH concentrations
strongly suggests that the maternal HPA axis was not involved in
the cortisol elevations we observed. In nonpregnant subjects,
mifepristone acts within hours of administration to inhibit directly
the negative feedback of cortisol on the HPA axis. This results in
increased ACTH followed by increased systemic cortisol.23,24 A
similar HPA axis response to ‘‘stress’’ has been suggested to explain
the rise in plasma cortisol that accompanies the progression of
labor.21 This too would be expected to result in ACTH elevation.
However, despite elevations in plasma cortisol, we did not observe a
sequence of an HPA cascade involving CRH or ACTH. Thus, the rise
in cortisol observed is probably not due to direct action on the
maternal HPA axis.
We acknowledge the limitations of our study, including a small
sample size and the possibility of beta-error. Since there are no
previous studies of in vivo plasma CRH alteration following
mifepristone exposure in term human pregnancy, our ability to
calculate statistical power was limited to projections based on in
vitro evidence. This in vitro data documented a two-fold increase in
CRH following mifepristone. Even though we projected a less robust
response, our data failed to demonstrate the 80% differences in the
mean plasma CRH levels used in our power calculation. Owing to
multiple factors, access to mifepristone for in vivo research
involving human pregnancies remains highly restricted and subject
419
Byrne et al.
to regulatory control. These limitations to access prevented us from
pursing a study redesign and expansion of sample size following
the analysis of our data. Lastly, our choice of placebo was based on
cost and availability. Our reviews of the literature found little
evidence that ascorbic acid administration would significantly
affect plasma levels of the hormones in question. In fact, both oral
and intravenous ascorbic acid administration have been associated
with cortisol reduction in the circulation.25,26
Our findings support observations that, when compared to
nonpregnant women and early pregnancy, the maternal HPA axis
response to elevated CRH and ACTH appears to be blunted in late
pregnancy.21,23,24 This supports concern that data obtained from
endocrine studies of nonpregnant subjects and in early pregnancy
cannot be universally applied to women pregnant at term.
Additional studies with larger numbers of subjects are warranted to
clarify the systemic and local factors influencing the
fetal–maternal unit and the initiation of term human parturition.
References
1. Nathanielsz PW. A time to be born: implications of animal studies in
maternal–fetal medicine. Birth 1994;21:163–9.
2. Challis JR, Lye SJ, Gibb W, Whittle W, Patel F. Alfaidy. Understanding
preterm labor. Ann NY Acad Sci 2001;943:225–34.
3. Challis J, Sloboda D, Matthews S, et al. Fetal hypothalamic-pituitary adrenal
(HPA) development and activation as a determinant of the timing of birth,
and of postnatal disease. Endocr Res 2000;26(4):489–504.
4. Karalis KP, Goodwin G, Majzoub JA. Cortisol blockade of progesterone: a
possible molecular mechanism involved in the initiation of human labor.
Nat Med 1996;2:556–60.
5. Jones SA, Brooks AN, Challis JRG. Steroids modulate corticotropin-releasing
factor production in human fetal membranes and placenta. J Clin
Endocrinol Metab 1989;68:825–30.
6. Jones SA, Challis JRG. Steroid, corticotropin-releasing hormone, ACTH, and
prostaglandin interactions in the amnion and placenta of early pregnancy
in man. J Endocrinol 1990;125:153–9.
7. Karalis KP, Majzoub JA. Regulation of corticotropin-releasing hormone by
steroids. Ann NY Acad Sci 1995;771:551–5.
8. Marinoni E, Korebrits C, Di Iorio R, Cosmi EV, Challis JRG. Effect of
betamethasone in vivo on placental corticotropin-releasing hormone in
human pregnancy. Am J Obstet Gynecol 1998;178:770–8.
9. Wing DA, Fassett MJ, Mishell Jr DR. Mifepristone for preinduction cervical
ripening beyond 41 weeks’ gestation: a randomized controlled trial. Obstet
Gynecol 2000;96:543–8.
10. Florio P, Severi FM, Ciarmela P, et al. Placental stress factors and
maternal–fetal adaptive response: the corticotropin-releasing factor family.
Endocrine 2002;19(1):91–102.
420
Mifepristone in Term Pregnancy
11. Kofman O. The role of prenatal stress in the etiology of developmental
behavioural disorders. Neurosci Biobehav Rev 2002;26(4):457–70.
12. McCoy SJ. Endocrine factors and postpartum depression. A selected review.
J Reprod Med 2003;48(6):402–8.
13. McLean M, Thompson D, Zhang HP, Brinsmead M, Smith R. Corticotropinreleasing hormone and b-endorphin in labour. Euro J Endocrinol 1994;
131:167–2.
14. Warren WB, Patrick SL, Goland RS. Elevated maternal plasma corticotropinreleasing hormone levels in pregnancies complicated by preterm labor. Am J
Obstet Gynecol 1992;166:1198–207.
15. Petraglia F, Genazzani AD, Aguzzoli L, et al. Pulsatile fluctuations of
plasma-gonadotropin-releasing hormone and corticotropin-releasing factor
levels in healthy pregnant women. Acta Obstet Gynecol Scan 1994;73:
284–9.
16. McLean M, Bisits A, Davies J, Woods R, Lowry P, Smith R. A placental clock
controlling the length of human pregnancy. Nat Med 1995;1:460–3.
17. Florio P, Cobellis L, Woodman J, Severi FM, Linton EA, Petraglia F. Levels of
maternal plasma corticotrophin-releasing factor and urocortin during labor.
J Soc Gynecol Invest 2002;9:233–7.
18. Magiakou MA, Mastorakos G, Rabin D, et al. The maternal hypothalamicpituitary–adrenal axis in the third trimester of human pregnancy. Clin
Endocrinol 1996;44:419–28.
19. Cooper EA, Brooks AN, Miller MR, Greer IA. Corticotrophin-releasing factor
immunostaining is present in placenta and fetal membranes from the first
trimester onwards and is not affected by labor or administration of
mifepristone. Clin Endocrinol 1994;41:677–83.
20. Copper ES, Greer IA, Brooks AN. Placental proopiomelanocortin gene
expression, adrenocorticotropin tissue concentrations, and immunostaining
increase throughout gestation and are unaffected by prostaglandins,
antiprogestins, or labor. J Clin Endocrinol Metab 1996;81:4462–9.
21. Carr BR, Parker CR, Madden JD, MacDonald PC, Porter JC. Maternal plasma
adrenocorticotropin and cortisol relationships throughout human pregnancy. Am J Obstet Gynecol 1981;139:416–21.
22. Ochedalski T, Zylinska K, Laudanski T, Lachowicz A. Corticotrophinreleasing hormone and ACTH levels in maternal and fetal blood during
spontaneous and oxytocin-induced labour. Eur J Endocrinol 2001;144:
117–21.
23. Spitz IM, Bardin CW. Clinical pharmacology of RU486 F an antiprogestin
and antiglucocorticoid. Contraception 1993;48:403–44.
24. Wang JD, Shi WL, Zhang GQ, Bai XM. Tissue and serum levels of steroid
hormones and RU486 after administration of mifepristone. Contraception
1994;49:245–53.
25. Liakakos D, Doulas NL, Ikkos D, Anoussakis C, Vlachos P, Jouramani G.
Inhibitory effect of ascorbic acid (vitamin C) on cortisol secretion following
adrenal stimulation in children. Clin Chim Acta 1975;65:251–5.
26. Kodama M, Kodama T, Murakami M, Kodama M. Vitamin C infusion
treatment enhances cortisol production of the adrenal via the pituitary
ACTH route. In vivo 1994;8:1079–85.
Journal of Perinatology 2004; 24:416–420