Original Article Is the New Definition of Bronchopulmonary Dysplasia More Useful?

Original Article
Is the New Definition of Bronchopulmonary Dysplasia More
Useful?
Rakesh Sahni, MD
Amer Ammari, MD
Mandhir S. Suri, MD
Vladana Milisavljevic, MD
Kiyoko Ohira-Kist, MA
Jen T. Wung, MD
Richard A. Polin, MD
70.8% weighed <751 g at birth. Associated comorbidities correlated significantly with grades of underlying pulmonary disease. Also, significantly longer hospital stay, discharge at a higher PMA and lower growth velocity was observed with increasing grades of BPD.
CONCLUSIONS:
The new system for grading the severity of BPD offers a better description of underlying pulmonary disease and correlates with the infant’s maturity, growth and overall severity of illness. Whether it will have a role in predicting long-term outcome remains to be determined.
Journal of Perinatology (2005) 25, 41–46. doi:10.1038/sj.jp.7211210
Published online 11 November 2004
OBJECTIVE:
To determine the incidence of bronchopulmonary dysplasia (BPD) in low birth weight (LBW) infants <1251 g managed with early bubble nasal continuous positive airway pressure (NCPAP) and a gentle ventilation strategy using the newly proposed definition for BPD and the previous definitions.
METHODS:
Needs for supplemental oxygen and positive pressure (positive pressure ventilation or NCPAP) during initial hospitalization were evaluated in 266 inborn LBW infants (birth weight <1251 g). The data were categorized in three weight groups, <751, 751 to 1000 and 1001 to 1250 g and the incidence of BPD was computed in survivors based on oxygen need at 28 days, 36 weeks postmenstrual age (PMA) and the new severity of BPD criteria, that is, mild BPD : need for supplemental oxygen
Z
28 days, but not at 36 weeks PMA; moderate BPD : need for supplemental oxygen
Z 28 days and <30% at 36 weeks PMA and severe BPD : need for supplemental oxygen
Z
28 days, and >30% at 36 weeks PMA and/or positive pressure at 36 weeks PMA. Further, BPD-associated comorbidities and short-term outcome data during hospitalization were compared among the groups, defined by severity of BPD.
RESULTS:
Among LBW infants <1251 g, the incidences of BPD at 28 days and
36 weeks PMA were 21.1 and 7.4% respectively. Using the newly defined criteria, the incidences of mild, moderate and severe BPD were 13.5, 4.8
and 2.6%, respectively. In total, 64.6% of these infants had mild BPD and
Department of Pediatrics, College of Physicians and Surgeons, Columbia University, New York,
NY, USA.
Address correspondence and reprint requests to Rakesh Sahni, MD, Department of Pediatrics,
College of Physicians and Surgeons, Columbia University, 630 W. 168th Street, New York, NY
10032, USA.
Journal of Perinatology 2005; 25:41–46 r 2005 Nature Publishing Group All rights reserved. 0743-8346/05 $30 www.nature.com/jp
INTRODUCTION
The definition of bronchopulmonary dysplasia (BPD), first described by Northway Jr et al. in 1967
1 has changed over the past three decades. Antenatal glucocorticoid therapy, postnatal surfactant therapy and gentler ventilation techniques have minimized severe lung injury in more mature and larger infants.
BPD is now infrequent in infants with gestational age exceeding
30 weeks or birth weight more than 1200 g.
2
With the change in clinical presentation of BPD, the original description now applies only to a minority of patients.
Various definitions of BPD have been used in the literature.
In the past, the most commonly used was that of the 1979 BPD workshop, which defined BPD as 28 days of oxygen therapy with radiographic changes.
3
Oxygen requirement at 36 weeks postmenstrual age (PMA) was suggested as a better predictor of long-term respiratory outcomes and is presently most widely used.
4
However, these definitions have the limitation that the varied use of supplemental oxygen and positive pressure among different centers is not taken into account. Given the importance of consistent definition of BPD, a more extensive definition was proposed at a recent NIH BPD workshop.
5
This new definition uses oxygen dependency at 36 weeks PMA, total duration of oxygen supplementation, positive pressure requirements and gestational age of the infant to delineate the three degrees of severity, mild, moderate and severe ( mild BPD : need for supplemental oxygen
Z
28 days, but not at 36 weeks PMA; moderate BPD : need for supplemental oxygen
Z
28 days and <30% at 36 weeks PMA and severe BPD : need for supplemental oxygen
Z
28 days, and >30% at 36 weeks PMA and/or positive pressure at 36 weeks PMA).
41
Sahni et al.
New Definition of BPD
Preliminary validation of this definition was performed for infants with gestational ages <32 weeks from the NICHD Neonatal
Network database and Palta’s data.
6
However, its relationship to the previous definitions remains unknown.
The objective of this study was to determine the incidence of
BPD in infants <1251 g, using the newly proposed definition for
BPD and the previous definitions. Further, BPD-associated comorbidities during hospitalization and prior to discharge and short-term outcome data related to duration of hospitalization, growth and PMA at discharge were compared among the various groups, defined by the new severity of BPD definition.
METHODS
We performed a retrospective analysis on the clinical course data of all inborn low birth weight infants (birth weight <1251 g) admitted to the neonatal intensive care unit at Children’s Hospital of New
York between July 1999 and June 2002. The study was approved by
Institutional Review Board. The mean birth weight and gestational age were 864±231 g (mean±SD) and 26.9±2.4 weeks, respectively.
The variables extracted from the infant’s medical records included birth weight, gestational age, duration of respiratory support modality (positive pressure ventilation (PPV) or nasal continuous airway pressure (NCPAP), duration and amount of supplemental oxygen therapy (specifically during the initial 28 days of life and at
36 weeks of PMA), disposition (discharge to home, transfer to another medical facility or expiration), discharge weight, length of initial hospitalization, PMA at discharge, growth velocity ([discharge weight-birth weight]/length of hospitalization) and associated neonatal comorbidities: airleak syndromes, patent ductus arteriosus
(PDA), PDA needing surgical ligation, necrotizing enterocolitis
(NEC), NEC requiring surgery, retinopathy of prematurity (ROP), severe ROP (requiring photocoagulation), and severe intraventricular hemorrhage (grades III–IV). For infants who were transferred to chronic care or other medical facilities for continued care, similar data were obtained prior to discharge to home.
Respiratory Care Strategy
All spontaneously breathing infants with respiratory distress and an oxygen requirement were placed on NCPAP. Nasal continuous airway pressure was initiated at 5 cmH
2
O within the first ten minutes of life. The fractional inspired oxygen (FiO
2
) was adjusted to maintain arterial oxygen tension between 50 and 70 mmHg or oxygen saturation between 90 and 95%. Infants without spontaneous respiratory efforts and those with spontaneous respiration but showing inadequate ventilation (arterial carbon dioxide tension >65 mmHg and pH <7.2) or inadequate or worsening oxygenation with a FiO
2
Z
0.6 were intubated and ventilated. Administration of exogenous surfactant (Survanta s
) as late rescue was reserved for intubated infants requiring a
FiO
2
>0.60 to maintain adequate arterial oxygen saturation.
42
The ventilatory modes focused on maintenance of adequate oxygenation with minimization of volutrauma. The principles of this approach used low ventilatory settings while preserving spontaneous respiration to maintain PaO
2 between 50 and
70 mmHg or oxygen saturation between 90 and 95%, and PaCO
2 between 40 and 60 mmHg. The ventilator was initially set to provide inspiratory pressures to produce adequate chest excursion and air entry, positive end expiratory pressure (PEEP) of 5 cmH
2 rate at r
40 breaths per minute with inspiratory time of 0.5
O, seconds. If the infant showed excessively labored spontaneous respiration or the PaCO
2 remained above 60 mmHg, highfrequency positive pressure ventilation was used by setting the ventilator rate at 100/min, with inspiratory time of 0.3 seconds and
PEEP of 0 cmH
2
O (to account for the inadvertent PEEP associated with such short expiratory times). If the infant failed above management and/or the PaCO
2 remained elevated (>60 mmHg), the infant was given a trial on high frequency oscillatory ventilation. Following weaning off the ventilatory support, supplemental oxygen was provided to maintain oxygen saturations between 90 and 95%, as needed.
The need for supplemental oxygen, positive pressure (positive pressure ventilation or NCPAP), short-term associated comorbidities during hospitalization and prior to discharge and short-term outcome data related to duration of hospitalization, PMA at discharge and growth velocity were evaluated. The data were categorized in three weight groups, <751, 751 to 1000 and 1001 to
1250 g and the incidence of BPD was computed based on oxygen need at 28 days, 36 weeks PMA and the newly proposed BPD criteria among the survivors at different time points. Further, the categorical data on the above-described BPD-associated comorbidities were compared among infants with different grades of BPD, using w
2 analyses. Owing to small number of infants with moderate and severe BPD, the data on comorbidities in these two groups were combined for analyses. Short-term continuous outcome data related to duration of hospitalization, PMA at discharge and growth velocity were compared among the infants with different grades of BPD using one-way ANOVA.
RESULTS
There were 266 LBW infants with birth weight <1251 g who were admitted with intention to treat during the 3-year study period. Of these, 237 (89.1%) and 230 (86.5%) were alive at 28 days of life and 36 weeks PMA, respectively. Five infants died after 36 weeks
PMA and the remaining 225 (84.5%) infants were discharged home. Of these 225 infants, 21 were transferred (11 to chronic care and 10 to maternal referral facilities) prior to discharge home.
Pertinent infant data and discharge characteristics were extracted from those institutions for all of these 21 infants. There were 136
(51.1%) female infants in the study population; 43 (21.4%) were
Journal of Perinatology 2005; 25:41–46
New Definition of BPD Sahni et al.
black, 60 (28.1%) were Caucasian and 127 (47.7%) were Hispanic.
Antenatal steroids were administered to 192 (72.2%) mothers and exogenous surfactant given to 56 (21.0%) infants. Only seven
(2.6%) infants received postnatal steroids.
Among our study infants (mean gestational age ¼ 27.4±2.4
weeks) the incidences of BPD at 28 days and 36 weeks PMA were
21.1% ( n ¼ 237) and 7.4% ( n ¼ 230), respectively. Using the new definition of BPD, the incidences of mild, moderate and severe
BPD, were 13.5, 4.8 and 2.6%, respectively ( n ¼ 230) (see Table 1).
In the infants with BPD by newly defined criteria, 64.6% had mild
BPD and 70.8% weighed <751 g at birth.
As shown in Table 2, the BPD-associated comorbidities correlated significantly with grades of pulmonary disease with higher incidence of airleak syndromes ( w
2 ¼ 9.4, p <0.01), PDA
( w
2
¼ 29.1, p <0.0001), PDA needing surgical ligation ( w
2 p <0.0005), NEC ( w
2 ¼ 9.6, p <0.01), overall ROP ( w
2 ¼
¼ 15.2,
36.5, p <0.0001), severe ROP ( w
2
¼ 13.5, p <0.001), and severe intraventricular hemorrhage ( w
2
¼ 11.4, p <0.005) among infants with moderate and severe BPD as compared to infants with no
BPD.
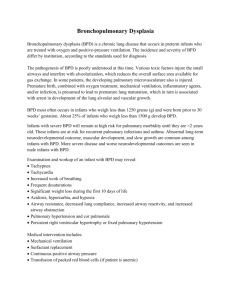
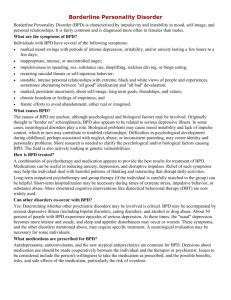
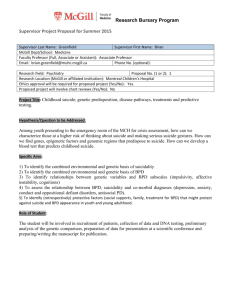
Among infants who were discharged home ( n ¼ 225), infants with severe BPD as compared those with no BPD, had a significantly longer hospital stay (313.0±38.2 vs 56.4±25.9 days, p <0.00001), were discharged at a higher PMA (69.2±7.5 vs
34.9±5.3 weeks, p <0.00001), and had lower growth velocity
(12.9±0.03 vs 18.7±5.2, p <0.002), as shown in Figures 1–3.
DISCUSSION
Despite technologic advances, increased use of exogenous surfactant and antenatal steroids, improved ventilatory strategies
Figure 1.
Length of stay (days) during initial hospitalization by severity of BPD for infants discharged home ( n ¼ 225).
Table 1 Incidence of BPD Using Different Definitions
Birth weight (g) n ( N ) Gestational age
(weeks)*
Oxygen at 28 days (%) ( N )
Oxygen at 36 weeks PMA (%)
( n )
<751
751–1000
1001–1250
<1251
67 (72)
72 (73)
91 (92)
230 (237)
25.4±1.9
27.0±1.8
28.9±1.8
27.3±2.3
50.0 (36)
17.8 (13)
1.1 (1)
21.1 (50)
22.4 (15)
1.4 (1)
1.1 (1)
7.4 (17)
N and n refer to infants alive at 28 days of life and at 36 weeks PMA, respectively. PMA ¼ postmenstrual age.
*Mean±SD.
Mild BPD (%)
( n )
28.3 (19)
16.6 (12)
0 (0)
13.5 (31)
Moderate BPD
(%) ( n )
Severe BPD (%)
( n )
13.4 (9)
1.4 (1)
1.1 (1)
4.8 (11)
8.9 (6)
0 (0)
0 (0)
2.6 (6)
Table 2 Incidence of Comorbidities Associated with Different Grades of Newly Defined BPD
Comorbidities No BPD ( n ¼ 182)
% ( n )
Mild BPD ( n ¼ 31)
% ( n )
Air leak syndromes
PDA overall
PDA requiring surgical ligation
NEC overall
NEC requiring surgery
ROP overall
ROP requiring treatment
Intraventricular hemorrhage (Grades III–IV)
2.7 (5)
37.9 (69)
21.7 (15)
5.5 (10)
50.0 (5)
22.0 (40)
7.5 (3)
2.2 (4)
9.7 (3)
77.4 (24)
33.3 (8)
16.1 (5)
20.0 (1)
61.3 (19)
21.1 (4)
9.7 (3)
Journal of Perinatology 2005; 25:41–46
Moderate+severe BPD ( n ¼ 17)
% ( n )
17.6 (3)
88.2 (15)
73.3 (11)
23.5 (4)
75.0 (3)
76.5 (13)
53.8 (7)
17.6 (3)
P
<0.01
<0.0001
<0.0005
<0.01
0.25
<0.0001
<0.001
<0.005
43
Sahni et al.
New Definition of BPD
Figure 2.
Postmenstrual age at discharge (weeks) from hospital by severity of BPD for infants discharged home ( n ¼ 225).
Figure 3.
Growth velocity (g/day) during initial hospitalization by severity of BPD for infants discharged home ( n ¼ 225).
and better nursing care practices, BPD continues to be a major health problem for the increasing number of extremely premature infants who survive. The incidence of BPD reported in the literature varies widely.
7
The lack of uniformity in the diagnostic criteria of
BPD may be responsible for much of the variation in the incidence of BPD. Unlike other disease definitions, which reflect the underlying pathophysiology, the different diagnostic criteria for
BPD have largely been based on a single clinical criterion, the need for prolonged oxygen therapy, which serves as a marker for chronic lung injury. The importance of having consistent criteria for the diagnosis of BPD may have a little impact on clinical practice; however, it is of critical importance when BPD is used as an end point in clinical research trials and may also have relevance for comparison of outcomes across multiple interventional and observational studies.
In the 1970s, Bancalari et al.
8 proposed criteria to define BPD as oxygen dependency during the first month of life accompanied by
44 clinical and radiographic findings. Over the subsequent years as the clinical presentation of BPD has evolved, these criteria, which characterized the classic presentation of severe BPD originally described by Northway Jr et al.
1 are now outdated. In most infants with BPD today (i.e. "new BPD"), the condition follows a less severe course of respiratory distress syndrome and these infants generally have intervals with no supplemental oxygen needs during the first weeks of life. There is a wide variation in the incidence of
BPD in the same group of extremely LBW infants if the calculations are based on need for oxygen every day during the first 28 days of life vs requirement for oxygen on day 28 (5.9 vs
57.2%) as a significant number of these infants (94%) spend at least a day or more without oxygen dependency during the first month of life.
9
Although oxygen requirement on day 28 appears to be a accurate marker of BPD, it still has serious limitations as some infants may need only a few days of supplemental oxygen around day 28 and may not have chronic lung disease.
Additionally, it is possible that some infants may not require supplemental oxygen on that particular day of life, but may later develop severe lung injury.
In 1988, Shennan et al.
4 proposed that the definition of BPD be modified to include requirements for oxygen at 36 weeks PMA along with a total oxygen duration of
Z
28 days. These new criteria identified a group of infants with more severe lung disease, especially those born at lower gestational ages. Subsequently, the
36-week BPD definition was shown to predict long-term respiratory outcome better than the oxygen dependency during the first month of life.
8,10 –11
However, there are still some issues with this definition particularly related to gestational age that are inherent in defining BPD as oxygen requirement at 36 weeks PMA. An extremely preterm infant will, by definition, require a much longer duration of supplemental oxygen therapy than a more mature preterm infant to reach 36-week PMA criteria for BPD. The duration of oxygen therapy may correct for lower gestational age in extremely preterm infants, but not for more mature preterm infants. Additionally, the limitation of using oxygen needs at
36 weeks PMA to define BPD is affected by the inaccuracies in estimating true durations of gestation at lower gestational ages.
Several investigators have attempted to establish the predictive value of different diagnostic criteria for BPD in relation to longterm pulmonary or neurologic outcome. Not surprisingly, most of these studies have shown a clear relationship between severe BPD and poor respiratory outcome.
6,8,10 –15
Using the NICHD Neonatal
Network database for all infants with birth weights under 1 kg and gestational ages under 32 weeks, Ehrenkranz showed that oxygen administration for the first 28 days resulted in the highest sensitivity, specificity, and positive and negative predictive values for oxygen administration at 36 weeks; while oxygen administration at 36 weeks PMA had the highest values for sensitivity, specificity, and the percent of infants correctly classified in respect to predicting oxygen need at discharge.
Journal of Perinatology 2005; 25:41–46
New Definition of BPD Sahni et al.
Rehospitalizations for respiratory causes, and the use of pulmonary medications after discharge, were predicted similarly by the 28-day and the 36-week oxygen requirements.
5
The relationship between
BPD and other outcomes is more difficult to establish, however, because it is confounded by a number of co-morbidities that are associated with extreme prematurity.
Our data indicate that in infants <1251 g, even with a low incidence of BPD and conservative respiratory care strategies including liberal use of NCPAP, the new definition seems to better classify infants with BPD based on the underlying pulmonary disease without affecting the overall incidence of BPD. The inclusion of positive pressure support (positive pressure ventilation or NCPAP) at 36 weeks PMA in the diagnostic criteria of severe BPD did not show a significant number of infants in that category. In fact, majority of our infants had mild BPD and most of these were extremely small (<750 g and <26 weeks gestation). One has to be cautious regarding the need for positive pressure support in defining severe BPD as positive pressure ventilation and NCPAP may not be similar. We believe that the new definition may offer an advantage over the previous definitions when comparisons in outcomes are made across institutions with different respiratory care practices. As expected, our data demonstrate the tendency for higher occurrence of associated comorbidities with more severe grades of BPD. The new criteria also predicted the duration of hospitalization, PMA at discharge and growth velocity during hospitalization based on severity of BPD. Although the new definition offers a better description of underlying pulmonary disease and accounts for severity of associated illness and maturity at discharge, its role in predicting long-term outcome also remains to be determined. These new diagnostic criteria need to be validated in infants >32 weeks.
Several important limitations remain for all the diagnostic criteria for BPD (including the newly proposed definition) since they are based on persistence of oxygen dependency. These include variations in oxygen requirement as a result of use of different respiratory support modalities (PPV or NCPAP), the differences in altitude and the use of drugs that may influence gas exchange, such as respiratory stimulants, diuretics and corticosteroids.
Another major problem is the variation in the level of oxygenation considered acceptable by different clinicians.
16
All definitions assume that criteria for oxygen administration are uniform, which is not the case. This clearly has a major influence on the total duration of oxygen therapy and, thus, on the classification of BPD.
Moreover, recent data suggest that targeting higher oxygen saturations (95 to 98%) in extremely preterm infants who are dependent on supplemental oxygen is associated with higher rates of need for supplemental oxygen at 36 weeks of PMA and a significantly higher frequency of home-based oxygen therapy. Also, this high or more physiological oxygen-saturation range does not confer any significant benefit with respect to growth and development at 12 months corrected age.
17
To minimize the
Journal of Perinatology 2005; 25:41–46 variations introduced by different practices of oxygen use, Walsh et al. have recently described a physiological concept of defining
BPD. This stepwise timed oxygen reduction test uses challenges with lower inspired oxygen concentration in infants receiving supplemental oxygen ( r 0.3 at 36±1-week PMA) and has been shown to be safe, feasible, reliable and valid for defining BPD.
18
Hopefully, ongoing efforts like these to standardize criteria for oxygen supplementation will further reduce the variability in defining BPD.
Acknowledgements
We thank our colleague Karl Schulze for his helpful suggestions.
References
1.
Northway Jr WH, Rosan RC, Porter DY. Pulmonary disease following respirator therapy of hyaline-membrane disease: bronchopulmonary dysplasia. N Engl J Med 1967;276:357–68.
2.
Bancalari E, Gonzalez A. Clinical course and lung function abnormalities during development of neonatal chronic lung disease. In: Bland RD,
Coalson JJ, editors Chronic Lung Disease in Early Infancy. New York: Marcel
Dekker; 2000 p. 41–64.
3.
National Institutes of Health. Report of Workshop on Bronchopulmonary
Dysplasia; NIH Publication No. 80-1660. Washington, DC: National
Institutes of Health; 1979.
4.
Shennan AT, Dunn MS, Ohlsson A, Lennox K, Hoskins EM. Abnormal pulmonary outcomes in premature infants: prediction from oxygen requirement in the neonatal period. Pediatrics 1988;82:527 –32.
5.
Jobe AH, Bancalari E. Bronchopulmonary dysplasia. NICHD–NHLBI–ORD
Workshop. Am J Respir Crit Care Med 2001;163:1723–9.
6.
Palta M, Sadek-Badawi M, Evans M, Weinstein MR, McGuinnes G.
Functional assessment of a multicenter very low-birth-weight cohort at age
5 years: Newborn Lung Project. Arch Pediatr Adolesc Med 2000;154:23 –30.
7.
Lemons JA, Bauer CR, Oh W, Korones SB, Papile LA, Stoll BJ. Very low birth weight outcomes of the National Institute of Child Health and Human
Development Neonatal Research Network, January 1995 through December
1996. Pediatrics 2001;107:1–8.
8.
Bancalari E, Abdenour GE, Feller R, Gannon J. Bronchopulmonary dysplasia: clinical presentation. J Pediatr 1979;95:819–23.
9.
Bancalari E, Claure N, Sosenko IR. Bronchopulmonary dysplasia: changes in pathogenesis, epidemiology and definition. Semin Neonatol 2003;8:63–71.
10.
Palta M, Gabbert D, Weinstein MR, Peters ME. Multivariate assessment of traditional risk factors for chronic lung disease in very low birth weight neonates. J Pediatr 1991;119:285–92.
11.
Palta M, Sadek M, Barnet JH, et al. Evaluation of criteria for chronic lung disease in surviving very low birth weight infants. J Pediatr
1998;132:57–63.
12.
Tepper RS, Morgan WJ, Cota K, Taussig LM. Expiratory flow limitation in infants with bronchopulmonary dysplasia. J Pediatr 1986;109:1040–6.
13.
Gerhardt T, Hehre D, Feller R, Reifenberg L, Bancalari E. Serial determination of pulmonary function in infants with chronic lung disease.
J Pediatr 1987;110:448–56.
45
Sahni et al.
New Definition of BPD
14.
Baraldi E, Filippone M, Trevisanuto D, Zanardo V, Zacchello F. Pulmonary function until two years of life in infants with bronchopulmonary dysplasia.
Am J Respir Crit Care Med 1997;155:149–55.
15.
Northway W, Moss R, Carlisle K, et al. Late pulmonary sequelae of bronchopulmonary dysplasia. N Engl J Med 1990;323:1793 –9.
16.
Ellsbury DL, Acarregui MJ, McGuinness GA, Klein JM. Variability in the use of supplemental oxygen for bronchopulmonary dysplasia. J Pediatr
2002;140:247–9.
17.
Askie LM, Henderson-Smart DJ, Irwig L, Simpson JM. Oxygen-saturation targets and outcomes in extremely preterm infants. N Engl J Med
2003;349(10):959 –67.
18.
Walsh MC, Wilson-Costello D, Zadell A, Newman N, Fanaroff A. Safety, reliability, and validity of a physiologic definition of bronchopulmonary dysplasia. J Perinatol 2003;23:451–6.
46 Journal of Perinatology 2005; 25:41–46