Oxygen Transport and
Asphyxia
AnS 536
Spring 2016
Goals
To transport oxygen from maternal blood across the placenta to
fetal blood, and after birth from the lungs to the blood stream
To move oxygen from blood to tissues to allow aerobic
metabolism (efficient production of ATP)
To move carbon dioxide in the reverse direction
Erythrocytes
After maturation from stem cells in bone marrow,
erythrocytes have a circulating life of ~120d
Highly specialized cells:
Cytoplasm contains ~35% solution of hemoglobin, but
is devoid of subcellular organelles
Cannot synthesize nucleic acids or proteins, limited lipid
metabolism
Carbohydrate metabolism devoted to maintaining
functional pumps on cell membrane
Erythrocytes
After cell death, hemoglobin degraded and iron
recycled to bone marrow
As they pass through capillaries, cells deform into
ellipsoidal, hemispheric, or teardrop shapes
Cell fragility increased during newborn period
Increased risk and incidence of hemolytic diseases
Transport of Gases in Blood
PO2 not only determines the dissolved oxygen
content of blood, but also affects the amount of
oxygen in reversible chemical combination with
hemoglobin
Chemical and physiological actions of gases
depend on the partial pressures they exert in the
gas phase and in solution in various body fluids
Hemoglobin
The binding of one molecule of O2 to Fe2+ increases the affinity of
the other sites for oxygen binding (4 total)
Carbon dioxide binds to the globulin portions of the molecule rather
than to the iron molecules
Accounts for about 10% of CO2 transport
The sigmoidal shape of the oxygen dissociation curve is physiologically
important
Permits blood to deliver much more oxygen to tissues than a hyperbolic
curve
Hemoglobin
Video Break
OXYGEN BINDING VIDEO:
http://www.dnatube.com/video/274/Hemoglobin-Oxygen-Binding
OXYGEN TRANSPORT VIDEO:
http://www.youtube.com/watch?feature=player_detailpage&v=WXOBJE
XxNEo
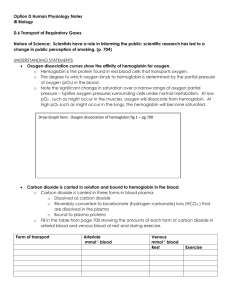
O2-Hb Dissociation Curve
Illustrates a relationship between the partial pressure of
oxygen (PO2) and percent saturated hemoglobin (Hb)
Hemoglobin
Increasing pH in RBC will increase the affinity of
Hb for oxygen (in the lungs)
When Hb binds to oxygen, it undergoes a
conformational change that releases H ions from
globin chains, decreasing pH in the cell
In capillaries H+ generated by carbonic anhydrase
activity in RBC decreases pH and facilitates oxygen
delivery to tissues as well (high CO2
concentrations)
Oxygen Loading and Unloading
Bohr and Haldane Effects
Bohr Effect
Describes the influence of CO2 and pH on the release of O2
↓ in pH (↑ in acidity) due to CO2 and hydrogen ions can combine reversibly with Hb
at the sites other than the O2 binding sites (allosteric binding)
Results in a structural change of Hb, reducing its affinity for O2
Haldane Effect
Displacement of O2 from Hb increases affinity for CO2 and hydrogen ions
Bohr and Haldane Effects
Work together facilitating O2 liberation and the uptake of
CO2 and hydrogen ions at the tissue level
A Bohr or Haldane shift reduces Hb affinity for O2
Important in placental O2 transport
pH is highest in veins where O2 is picked up (umbilical and
placental arterioles)
pH is lowest at arteries after CO2 and hydrogen ions have
been picked up
Changes in pH and CO2 on both maternal and fetal side of
placenta regulate the rate of O2 transfer to a great extent
Bohr and Haldane Effects
Fetal pH is lower (more acidic) than maternal pH
Fetal acidosis is metabolic and not related to the high PCO2
Primarily due to placentally produced lactate and pyruvate
The effect of low pH on O2 delivery to tissues is often
overlooked, but may be important in maintaining O2 delivery to
tissues at an appropriate rate
2,3-Bisphosphoglycerate
(2,3-BPG)
Binds with greater affinity to Maternal deoxyhemoglobin
Once it binds to first binding site, it allosterically affects other sites
in hemoglobin to effectively increase the rate of release of oxygen at
tissue level
Right-shift of curve
Fetal Hemoglobin (HbF)
HbF has a higher affinity for O2
than HbA
Two alpha-gamma dimers rather
than two alpha-beta dimers
Creates a LEFT shift in the
dissociation curve much like the
effect of
↑ pH, ↓ temperature,
or ↓ 2,3 BPG
↑ affinity for O2 by Hb in the fetal blood
enhances O2 transport across the
placenta
After birth HbF declines as neonates
begin to manufacture new erythrocytes
and HbA
HbF binds 2,3-BPG poorly
Hemoglobin Transitions
Fetal Hemoglobin
Fetal Hemoglobin
Cytochrome P450
O2 is MUCH more soluble in lipids (like membranes)
than in water (as in plasma or cytoplasm)
Cytochrome P450 enhances transport processes due
to its high affinity for O2 and accumulates along the
endoplasmic reticulum (ER) of placental cells
Many different varieties
Most involve drug metabolism
All incorporate oxygen into metabolic processes
Tissues can up- or down-regulate the levels of this
molecule to enhance O2 transport into cell
Cytochrome P450
ER forms channels from the cell membrane to the mitochondria allowing
O2 to move more freely throughout or across the cell
Alignment of P450 along the ER channels creates a high affinity, O2
soluble freeway for O2 to travel
P450 enhances transplacental O2 transport
Studies have shown blocking P450 will decrease transplacental O2 flux by
over 75%
Fetal Gas Exchange
CO2 diffuses across placenta primarily in molecular form - not as
bicarbonate ion
Fetal PCO2 is higher than maternal
Fetal oxygen consumption is equivalent to adult values
Placenta is designed to protect the fetus from inadequate or
excessive oxygen availability
Fetal Gas Exchange Cont…
Fetal mechanisms for protection against oxygen radicals are
poorly developed prior to birth
Increased oxygen in fetal blood may have more adverse effects
than beneficial effects
Induction of superoxide dismutase is due to increased exposure to
oxygen postnatally
Questions?
 0
0