Original Article
Twelve-Month Prospective Study of Oxygen Saturation
Measurements among Term and Preterm Infants
Michael W. Beresford, PhD
Heather Parry, RGN, RSCN
Nigel J Shaw, MD
BACKGROUND:
Optimising home oxygen delivery in infants has important logistical and
safety implications. This can be aided by having a suitable reference
range of normal values for arterial oxygen saturation using pulse
oximetry (SpO2).
OBJECTIVES:
To describe oxygenation profiles in healthy preterm and term infants in
relation to gestational and postnatal age, to extend reference values to
guide home oxygen therapy.
STUDY DESIGN:
Prospective monitoring of SpO2 for 4 hours at 3 monthly intervals of 34
term, and 53 preterm healthy infants, took place over a 12-month period
using an Ohmeda Biox 3700e pulse oximeter and data logger.
RESULTS:
Group mean and 5th percentiles were used to construct cumulative
frequency curves at each time interval, representing the normal reference
range of SpO2 profiles for term and preterm infants over time.
CONCLUSIONS:
These data may be used to test the benefits in the home or hospital of
having a reference range of normal values for cumulative SpO2.
Journal of Perinatology (2005) 25, 30–32. doi:10.1038/sj.jp.7211206
Published online 14 October 2004
INTRODUCTION
Pulse oximetry (SpO2) has become the mainstay of assessment
of oxygenation in preterm infants who have prolonged oxygen
dependency. In the absence of randomized-controlled trials
Liverpool Women’s Hospital, Liverpool, UK.
Address correspondence and reprint requests to Ben Shaw, Neonatal Unit, Liverpool Women’s
Hospital, Liverpool L8 7SS, UK.
comparing the safety and efficacy of different SpO2 levels,
a pragmatic approach is to aim for normal SpO2 levels.
Using a convenient system that can analyse the infant’s
oxygenation profile and compare it to a reference range for SpO2,
we have previously reported such a reference range in a group of
33 infants born between 30 and 34 weeks gestation in the
immediate postnatal period.1 It is possible that this reference range
could change, as the infant gets older. However, there are no
longitudinal studies of SpO2 in infants and children from birth to
investigate this possibility.
The aims of this study were to describe oxygenation profiles in
healthy preterm and term infants in relation to gestational and
postnatal age and therefore to extend reference values to guide
home oxygen therapy.
METHODS
Infants were recruited to the study between July 1998 and July 1999
at Liverpool Women’s Hospital, UK, after local regional ethics
committee approval had been granted. Infants who had received no
mechanical ventilation or supplemental oxygen therapy were
recruited after parental consent had been obtained. Infants with
known congenital anomalies or cardio-respiratory disorders were
excluded. Gestational age was determined from maternal dates
and/or early antenatal ultrasound examination. All infants were
studied for a continuous period of 4 hours following a feed, while
asleep, or during a period of quiet wakefulness. Infants studied
were grouped into the following gestational age bands: term infants
Z37 weeks; preterm infants: <37 weeks.
Initial monitoring took place in term infants at least 48 hours
postdelivery and after 1 week for the preterm infants. Subsequent
monitoring took place in the infant’s home at approximately 3, 6,
9 and 12 months postdelivery.
The monitoring of SpO2 took place using a standard Ohmeda
Biox 3700e pulse oximeter using an averaging interval of 3
seconds. A data-logging device and dedicated software, developed at
the Department of Clinical Engineering, University of Liverpool,
was used to record the data. Initial measurements took place on
the neonatal unit or postnatal wards before discharge. Parents
agreed to be contacted following discharge at the appropriate time
intervals. At a convenient time, a dedicated research nurse (HP)
visited the family, and instructed the parents in operating and
recording oxygen saturations. Parents recorded four hours of data
while the infant slept, generally at night time. Measurements on
Journal of Perinatology 2005; 25:30–32
r 2005 Nature Publishing Group All rights reserved. 0743-8346/05 $30
30
www.nature.com/jp
Prospective Study of Oxygen Saturation Profiles in Infants
SpO2: Post-delivery
100.0
Cumulative oxygen saturation (%)
infants who were thought, in the opinion of the nurse, to have an
acute respiratory illness were postponed until the child had
clinically improved.
Analyses of raw data were performed blind to the infant’s
gestational or postnatal age. Using the group mean and lower 5th
percentile, a cumulative frequency curve was constructed for each
of the five recorded time intervals over the first year postdelivery.
Descriptive statistics and graphs were generated using Microsoft
Excel statistical software.
Beresford et al.
Term mean
Preterm mean
Reference mean
Term Lower
Preterm Lower
Reference Lower
75.0
50.0
25.0
85
87
89
91
93
95
97
99
SpO2 (%)
SpO2: 6 months post-delivery
Cumulative oxygen saturation (%)
A total of 87 infants were recruited to the study and had baseline
measurements performed. Median (range) gestational age for the
term infants (n ¼ 34) was 40 weeks (37 to 41) and for the preterm
infants (n ¼ 53) was 33 weeks (29 to 36). In all, 19 term infants
and 23 preterm infants were male. Median (interquartile, IQR) age
for the initial recording of term and preterm infants was 2 days (2
to 3) and 8 days (8–10), respectively. Median (IQR) age for each
of the subsequent recordings for all infants postdelivery was: 14
weeks (13–16); 27 weeks (26 to 28); 40 weeks (39 to 42); and 52
weeks (51 to 53).
During the course of the study, 11 (13%) parents asked for their
infant to be withdrawn from further follow-up. In addition, 46
(53%) of families, at some point over the next 12 months failed to
respond to an initial attempt to contact them and a subsequent
reminder. These families were deemed to have withdrawn
themselves from the study from that time point onwards. The
numbers of infants and median (range) gestational age of infants
on whom follow-up data were obtained at 6 and 12 months for the
term and preterm groups, respectively, was as follows. At 6 months,
term group (n ¼ 15): 39 weeks (37 to 41); preterm group
(n ¼ 32): 33 weeks (30 to 36). At 12 months, term group
(n ¼ 11): 39 weeks (37 to 41); preterm group (n ¼ 19): 33 weeks
(31 to 35).
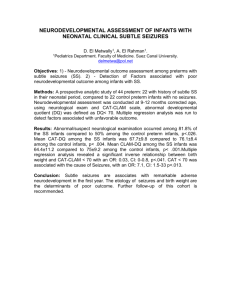
Figures 1 to 3 show the cumulative frequency for SpO2 for term
and preterm infants (along with the existing reference range)
postdelivery, and at 6 and 12 months, respectively (curves for 3 and
9 months not shown). The mean and lower 5th centile are shown
for each group, and similar data are shown of the reference data.1
Figure 1. Mean and lower 5th centile for the cumulative frequency for
SpO2 for term and preterm infants (along with the existing reference
range) postdelivery.
100.0
Term mean
Term Lower
Preterm mean
Preterm Lower
Reference Lower
Reference mean
75.0
50.0
25.0
85
87
89
91
93
95
97
99
SpO2 (%)
Figure 2. Mean and lower 5th centile for the cumulative frequency for
SpO2 for term and preterm infants (along with the existing reference
range) 6 months postdelivery.
SpO2: 12 months post-delivery
Cumulative oxygen saturation (%)
RESULTS
100.0
Term mean
Term Lower
Preterm mean
Preterm Lower
Reference mean
Reference Lower
75.0
50.0
25.0
85
87
89
91
93
95
97
99
SpO2 (%)
CONCLUSIONS
In this study, we have prospectively followed a healthy term and
preterm population of infants over a 12-month period and observed
their SpO2. We have extended our reference range for increasing
postnatal age using a data-logging device and dedicated software
that is relatively simple and practical for routine use at home and
in the nursery.
Journal of Perinatology 2005; 25:30–32
Figure 3. Mean and lower 5th centile for the cumulative frequency for
SpO2 for term and preterm infants (along with the existing reference
range) 12 months postdelivery.
Published data of SpO2 reference ranges in term and preterm
infants over time have been limited, having: included preterm
infants with significant neonatal respiratory disease;2 performed
follow-up measurements within a laboratory setting;3 studied
31
Beresford et al.
infants only on a single occasion over the first 9 months
postdelivery4 or during childhood;5,6 measured SpO2 levels only
during apnoeas or bradycardias;7 or only performed repeat
measures over the first four postnatal weeks.8
Mean cumulative SpO2 frequency for term and preterm infants
were very similar over the initial 6-month follow-up, and
corresponded to our existing reference range.1 They diverged
somewhat at 9 months and a year, where study numbers are
reduced. Of note, the 5th centiles are markedly variable between
groups, and compared to the existing reference range, particularly
after the initial 3-month follow-up. The reasons for variation
between curves may include: a fall in sample numbers over time;
increasing movement artefact not detected with increasing
postnatal age; difference in clinical characteristics between groups
and with the original cohort; or some real differences between
groups over time. Other factors that may contribute to variation in
profiles include: idiopathic pulmonary hypertension; on-going
alveolar development in preterm infants producing aberration in
an otherwise healthy population; circadian rhythm; and sleep
stage. In this pragmatic study, we think it appropriate to use these
postnatal reference ranges for preterm infants in optimising home
oxygen parameters rather than simply a postdelivery cohort, as it
will allow for the possibility of differences due to artefact or
otherwise.
The cumulative frequency curve of oxygen saturations
represents the range of SpO2 profiles in normal term and preterm
infants. Such curves are helpful in guiding supplemental oxygen
treatment as they provide a more visual, user-friendly display of the
normal range than a single figure a mean (SD) SpO2 does.1 For
example, by monitoring oxygen saturations over time in room air
of an infant in whom it is thought that supplemental oxygen may
be required, an individual SpO2 profile can be constructed. This
can be superimposed on the term or preterm reference curve for
the appropriate postnatal age, and any deviation from the normal
SpO2 profile be assessed. Equally, a child on home oxygen could be
monitored for ongoing requirement by comparing their SpO2
profile in room air to the appropriate reference curve. A shift to the
left (with a greater proportion of time spent at SpO2 levels below
the normal values) would indicate an ongoing oxygen
requirement. Repeating the process in oxygen could confirm that
the infants are receiving sufficient oxygen to ensure their oxygen
saturation profile is within the normal range for healthy,
gestational, age-matched infants.
This study has underlined the difficulty of following up a cohort
longitudinally, with 22/34 (65%) of term infants and 25/53 (47%)
of preterm infants dropping out over a 12-month period. It was
thought withdrawal from the study was lower in the preterm group
because the infant had initially been in hospital longer and had
been more familiar with oxygen saturation monitoring as an in-
32
Prospective Study of Oxygen Saturation Profiles in Infants
patient, while the term infants were discharged much sooner, and
had had less contact with staff.
Monitoring infants while undisturbed reflected our clinical
practice of over-night saturation monitoring in children on home
oxygen. Recording SpO2 levels during activities such as feeding and
handling may have increased inaccuracies related to movement
artefact. It is acknowledged that with the advent of newer
technology, motion tolerant low perfusion capable oximeters might
have been able to produce more reproducible results. Restricting
the duration of recording to 4 hours permitted a reasonable period
of study, while maintaining the practicality of the methodology,
and reducing the potential for added movement artefact.9 The
effects of prodromal illness on measurements were not excluded, as
only those infants with actual symptoms had their date of
monitoring postponed. Having defined our criteria for detecting
major movement artefact, we cannot be certain of having excluded
minor artefacts resulting in transient desaturation. The most likely
effect of not detecting these events would have been to lower
marginally the overall mean SpO2.
In summary, we have constructed normal reference ranges for
cumulative SpO2 for healthy term and preterm infants over a 12month period. These data could be used to test the benefits in the
home or hospital of having a reference range of normal values for
cumulative SpO2.
References
1. Ng A, Subhedar N, Primhak RA, Shaw NJ. Arterial oxygen saturation profiles
in healthy preterm infants. Arch Dis Child Fetal Neonatal Ed 1998;79:
F64–F66.
2. Poets CF, Stebbens VA, Alexander JR, Arrowsmith WA, Salfield SAW, Southall
DP. Arterial oxygenation in preterm infants at discharge from the hospital
and six weeks later. J Pediatr 1992;120:447–54.
3. Hoppenbrouwers T, Hodgman JE, Arakawa K, Durand M, Cabal LA.
Transcutaneous oxygen and carbon dioxide during the first half year of life
in preterm and normal term infants. Pediatr Res 1992;31:73–9.
4. Horemuzova E, Katz-Salamon M, Milerad J. Breathing patterns, oxygen and
carbon dioxide levels in sleeping healthy infants during the first nine
months after birth. Acta Paediatr 2000;89:1284–9.
5. Owen G, Canter R. Analysis of pulse oximetry data in normal sleeping
children. Clin Otolaryngol 1997;22:13–22.
6. Owen GO, Canter RJ, Robinson A. Overnight pulse oximetry in snoring and
non-snoring children. Clin Otolaryngol 1995;20:402–6.
7. Hunt CE, Hufford DR, Bourguignon C, Oess MA. Home documented
monitoring of cardiorespiratory pattern and oxygen saturation in healthy
infants. Pediatr Res 1996;39:216–22.
8. Poets CF, Stebbens VA, Lang JA, O’Brien LM, Boon AW, Southall DP. Arterial
oxygen saturation in healthy term infants. Eur J Pediatr 1996;155:219–23.
9. Smith TC, Proops DW, Pearman K, Hutton P. Hypoxia in sleeping children:
overnight studies can be reduced to 4 hours without loss of clinical
significance. Clin Otolaryngol 1992;17:243–5.
Journal of Perinatology 2005; 25:30–32