Learning Objectives New Technology Reimbursement
advertisement

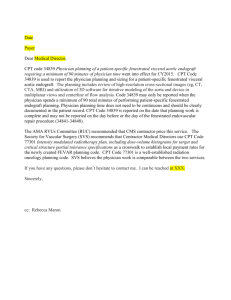
Learning Objectives New Technology Reimbursement • Understand the process for CPT applications Najeeb Mohideen, MD Co Chair Health Policy Committee ASTRO • Introduction to how new codes are valued Department of Radiation Oncology, Northwest Community Hospital, Arlington Heights, IL • Supervision requirements for RO procedures. AAPM Annual Meeting, Houston, TX July 27-31,2008 Projections of National Health Expenditures and Their Share of Gross Domestic Product, 2006-2017 National Health Expenditures and Their Share of Gross Domestic Product, 1960-2006 $2,500 $4,500 Dollars in Billions $1,500 $1,000 714.0 $500 253.4 27.5 74.9 1960 1970 $0 1980 1990 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 NHE as a Share of GDP 5.2% 7.2% 9.1% 12.3% 13.7% 13.6% 13.6% 13.7% 13.8% 14.5% 15.3% 15.8% 15.9% 15.9% 16.0% Source: Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group, at http://www.cms.hhs.gov/NationalHealthExpendData/ (see Historical; NHE summary including share of GDP, CY 1960-2006; file nhegdp06.zip). $4,000 $3,500 $3,000 Dollars in Billions 2,105.5 1,973.3 1,852.3 1,732.4 1,603.4 1,469.6 1,353.6 1,265.6 1,190.5 1,125.3 1,068.8 $2,000 $2,500 2,245.6 2,105.5 2,394.3 2,555.1 2,725.8 2,905.1 3,097.8 3,305.0 3,523.6 3,757.0 4,277.1 4,007.8 $2,000 $1,500 $1,000 $500 $0 NHE as a % of GDP: 2006* 16.0 2007 16.3 2008 16.6 2009 2010 2011 2012 16.9 17.1 17.4 17.7 2013 18.0 2014 18.4 2015 18.8 2016 2017 19.1 *2006 are actual data from the 2006 National Health Expenditure Accounts; 2007-2017 are projected data from the 2006 National Health Expenditure Accounts. Source: Centers for Medicare and Medicaid Services, Office of the Actuary, National Health Statistics Group, at http://www.cms.hhs.gov/NationalHealthExpendData/03_NationalHealthAccountsProjected.asp#TopOfPage (see Projected; NHE Historical and projections, 1965-2017, file nhe65-17.zip) and http://www.cms.hhs.gov/NationalHealthExpendData/ (see Historical; NHE summary including share of GDP, CY 1960-2006; file nhegdp06.zip). 19.5 Reasons for Rising Healthcare Costs • Demographics – aging population, rising obesity • Increased use of Investigations and Imaging – PET scans, MRI scans, Molecular testing • Expensive Drugs • New Technological Capabilities – SBRT, IGRT • Increased utilization of expensive procedures – eg IMRT 2006 HCPCS CPT Code 2003 OPPS+PartBTotal *includes beneficiary payments Rank 77413 77418 ~$380 million ~$318 million 1 2 77414 77427 77334 77295 77336 77290 ~$292 million ~$226 million 3 4 5 6 7 8 77300 77263 9 10 The Medical Technology Market OPPS+PartBTotal *includes beneficiarypayments 77418 ~ $820 million 1 Total Market : Over $ 200 Billion annually 77413 ~$260 million 2 Diagnostic Radiology: 25 Billion 77427 ~$225 million 3 77414 ~$210 million 4 Cardiovascular: 17 Billion 77334 5 77295 6 77336 7 77290 8 77300 9 77301 10 Orthopedics : 16 Billion Radiotherapy and Radiosurgery : 2.5 Billion New Technology Reimbursement • Most new devices launched without dedicated codes, coverage, or payment • Most new devices launched with little or no published data • It takes time, data, and a significant effort to garner new codes, influence coverage policies/ technology assessments, and drive appropriate payment Pathways For New Technology Codes ASTRO Priorities: Health Policy Committee • CPT Panel Process Vendors – Category I and III codes Hospitals Physicians Specialty Organizations ASTRO • • Payers • Research Department – NIH, NCI, Emerging Technology Committee – Paul Wallner, DO & Andre Konski, MD Health Policy Committee • RVS Update Committee (RUC) – Recommendations for Physician Work and PE • CMS – National Payment Rates – Local Coverage Determinations – HCPCS Coding • Medicare Fee Schedule – CPT Codes – owned, updated, maintained by the AMA • Hospital Outpatient Prospective System: New Technology In Medicare Physician Fee Schedule – G Codes – CMS controlled - for procedures applicable to physician and hospital payment systems – C Codes – CMS controlled - for pass through drugs and devices - applicable to OPPS only The MFS Reimbursement Process • Current Procedural Terminology codes (CPT) eg 77427 • Codes are valued on a scale relative to each other • Payments are determined by resource costs needed to provide them The Process For New Codes: ASTRO Code Development and Valuation Subcommittee SBRT Treatment Management SBRT Treatment Delivery “Typical patient” vignettes Complete description of the procedure, Supporting US peerreviewed literature CPT Editorial Panel CATEGORY 1 OR CATEGORY III THE RUC PROCESS CPT PANEL APPROVES CAT I CODES SURVEY PHYSICIANS Physician Work ASTRO REVIEWS NEW CODES PRACTICE EXPENSE Direct Inputs Components of RBRVS • Physician Work (does not include support staff) 53% – Time – Intensity • Technical skill and physical effort • Mental effort and judgment • Stress associated with patient risk • Direct Practice Expense 44% • Non Physician Clinical Labor • Equipment • Supplies • Professional Liability Insurance 3% Components of RBRVS • RO reimbursement is heavily weighted in technical reimbursement. • Pre IMRT: 50 - 60% technical charge • Post IMRT: 60 -80% technical charge Practice Expense Clinical Labor, Supplies and Equipment (CLSE) Clinical Labor Staff 2008 “Top 4” Clinical Labor Staff 2008 Staff Code • 44 Staff Types Description Rate 'Medical Physicist L152A 1.523 'Medical Dosimetrist/Medical Physicist L107A • Price per minute ranges from 0.23 to 1.523 1.075 'RN/OCN L056A 0.79 'Medical Dosimetrist L063A 0.63 Radiation Oncology Codes: Physics Time • 77301 Intensity modulated radiotherapy plan, including dose-volume histograms for target and critical structure partial tolerance specifications • 77418 Intensity modulated treatment delivery, single or multiple fields/arcs, via narrow spatially and temporally modulated beams, binary, dynamic MLC, per treatment session Radiation Oncology Codes: Physics Time Radiation Oncology Codes: Physics Time • 77371 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete • 77301 Intensity modulated radiotherapy plan, including dose-volume histograms for target and critical structure partial tolerance specifications – Medical Dosimetrist/Medical Physicist = 45 Minutes – Medical Physicist = 280 Minutes • 77418 Intensity modulated treatment delivery, single or multiple fields/arcs, via narrow spatially and temporally modulated beams, binary, dynamic MLC, per treatment session – Medical Physics Time = 0 Minutes Radiation Oncology Codes: Physics Time • 77371 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; multi-source Cobalt 60 based – Medical Physics Time = 115 minutes • 77372 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; linear accelerator based – Medical Physics Time = 60 minutes • 77373 Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions – Medical Physics Time = 75 minutes course of treatment of cranial lesion(s) consisting of 1 session; multi-source Cobalt 60 based • 77372 Radiation treatment delivery, stereotactic radiosurgery (SRS), complete course of treatment of cranial lesion(s) consisting of 1 session; linear accelerator based • 77373 Stereotactic body radiation therapy, treatment delivery, per fraction to 1 or more lesions, including image guidance, entire course not to exceed 5 fractions Physics work for CPT 77373 SBRT Delivery: • Setup DRR reference positions (20 min) • Establish Respiratory Cycle (RC) for patient (5 min) • Correlate RC with Target (Fiducial) position (5 min) • Compare with ref DRR's and consult with physician (5 min) • Treatment (30 min) • Re-establish RC/Target position if correlation lost (5 min) • Compare with DRR's, consult with physician (5 min) THE RUC PROCESS CPT PANEL APPROVES CAT I CODES SURVEY PHYSICIANS Physician Work The RBRVS equation ASTRO REVIEWS NEW CODES PRACTICE EXPENSE Direct Inputs RECOMMEND WORK VALUES (RVW) RUC MEETING ASTRO RVS COMMITTEE MEDICARE PAYMENT SCHEDULE CMS New CPT Code • CPT code assigned • Work RVUs recommended by AMA/RUC • Practice expense RVUs recommended by PEAC/RUC • New code and payment published in November Federal Register • Implemented following January • Total process takes two years Hospital Outpatient Prospective Payment System (HOPPS) OPPS: Unit of Payment • A separate payment is made for each Ambulatory Payment Classification (APC) NEW TECHNOLOGY PAYMENTS Specialty Organizations Vendors CMS NEW TECHNOLOGY APC G Codes : G 0339, G 0340 C Codes : Code for Electronic Brachytherapy No Professional Component reimbursement Can be used in a Hospital based setting only CODES FOR IGRT in 2004 Examples in Radiation Oncology: – Ultrasound : CPT 76950 – Stereoscopic X-ray – Computerized Tomography – Stereotactic Body Radiotherapy: – Other Modalities • Respiratory Gating, 4D RT • Tracking Systems (electromagnetic, optical) • Fiducial Markers CODES FOR IGRT in 2008 – – – – – Ultrasound : CPT 76950 Stereoscopic X-ray : CPT 77421 Computerized Tomography : CPT 77014 Stereotactic Body Radiotherapy: 77435 Other Modalities • Respiratory Gating, 4D RT • Tracking Systems • Fiducial Markers: 55876 for prostate CMS Supervision Rules Medicare Supervision Rules Image Guided Radiation Therapy (IGRT) • General Supervision - means the procedure is furnished under the physician’s overall direction and control, but the physician’s presence is not required during the performance of the procedure. Under general supervision, the training of the nonphysician personnel who actually performs the diagnostic procedure and the maintenance of the necessary equipment and supplies are the continuing responsibility of the physician. • Direct Supervision - in the office setting means the physician must be present in the office suite and immediately available to furnish assistance and direction throughout the performance of the procedure. It does not mean that the physician must be present in the room when the procedure is performed. ( Most Radiation Oncology Procedures) • Personal Supervision - means a physician must be in attendance in the room during the performance of the procedure. (CPT 77421) • All the IGRT codes are considered diagnostic tests subject to the physician supervision requirements in the Code of Federal Regulations at 42CFR §410.32(b)(3). • 77% increase in Medicare Procedures for RO IGRT Codes (76370,76950 and 77421) from 2003 to 2006 Increased Scrutiny on New Technology Codes Code will be reviewed in 2 years Monitor Utilization Rates Cost effectiveness/ Comparative effectiveness Does this improve outcome? Long Term outcomes Impact on work Quality What’s on the Horizon? • • • • • What’s on the Horizon? Big changes for Practice Expense Increased scrutiny on High Volume codes Equipment Utilization Rates Case Rates & Bundling/Pairing of Services An aggressive 5 YEAR Review Summary • Appropriate Payment for New Technology – Supporting clinical data – Adequate Codes – Appropriate Valuation – Appropriate Coverage • New Technology will need to show Comparative efficiency to alternatives • Increased Scrutiny of high utilization RO Codes MOVING FORWARD: All codes (current and future) are vulnerable even with the smallest change