Document 14239970
advertisement

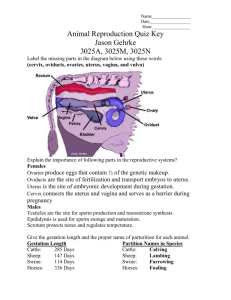
Journal of Medicine and Medical Sciences Vol. 1(3) pp. 083-086 April 2010 Available online http://www.interesjournals.org/JMMS Copyright ©2010 International Research Journals Full length Research Paper Transvaginal ultrasonographic measurement of cervical and uterine size in varying uterine versions/flexions Ambrogio P Londero¹, Serena Bertozzi², Arrigo Fruscalzo³ 1 Clinic of Obstetrics and Gynecology, University Hospital of Udine, Italy SSMM Misericordia 15, 33100 Udine, Italy 2 Clinic of Surgical Semeiotics, University Hospital of Udine, Italy 3 Department of Obstetrics and Gynecology, Gesundheitszentrum Rheine - Mathias-Spital, Rheine, Germany Accepted 02 April, 2010 This study is carried out to assess transvaginal ultrasonographic measurement of uterine and cervical size in varying uterine versions/flexions. We compared 28 transvaginal ultrasonographic measurements of the cervix and uterus on one patient with Allan-Master’s syndrome. Statistical analysis was performed by R (version 2.8.0), considering significant a p<0.05; Anova Oneway, Tukey test, and t-test were used to compare mean values, and Kolmogorov-Smirnov test to state the normality of all considered variables. Uterus was anteverted on 9 occasions, retroverted on 15 and on axis on 4. Mean cervical length and width results significantly greater by the anteverted uterus than by the retroverted one (p<0.05).There is a significant difference of cervical size based on its position and on uterus versions-flexions and we have to take in consideration a possible underestimation of cervical length with retroverted uterus. Keywords: Cervix measurement, retroverted uterus, transvaginal ultrasonography. INTRODUCTION The literature demonstrates that transvaginal ultrasonography is a good method to estimate cervical length, and it is more precise than vaginal visits (Jackson et al., 1992). It may be used to predict the risk of preterm delivery, labour induction failure or caesarean section requirement. Moreover, it may be useful for the surgeon to predict the difficulties of transvaginal or transabdominal histerctomy. While cervical size at mid- or last gestation is a recognized predictive factor for preterm labour (Theron et al., 2008; Smith et al.,2008; Ozdemir et al., 2007), but the literature lacks in studies about the cervical size at initial gestation or in non pregnant women. Furthermore, we did not find in the literature studies about estimation of cervical length in retroverted uterus. Our study then aims to assess transvaginal ultrasonographic measurement of uterine and cervical size in varying uterine versions/flexions. *Corresponding author email: ambrogio.londero@gmail.com; Tel: 0039-0432-559635; Fax: 0039-0432-559641; Cel: 0039347-2335937 MATERIALS AND METHODS We collected data about transvaginal ultrasonographic measurements on the same patient found to be affected by uterus hypermobility. This diagnosis was made by finding the uterous in previous ultrasonographies antevertedflexed in some occasions and retrovertedflexed in some others, and sometimes it was also possible to observe the uterus during the same ultrasound examination varying between the anteverted flexed and the retroverted flexed position. Within two consecutive menstrual cycles, uterus and cervix size were measured every second day (starting from the first day of the first cycle) on a 25-years-old caucasian nullipara nulligravida with uterine hypermotility and regular menstrual cycles lasting 29 days with 5 days of bleeding. All ultrasonographic measurements were performed by the same operator with an Acuson Sequoia 512 Sonographer with a transvaginal probe (EV8C4). Cervical length was measured as the linear distance between the internal, cervical orifice (considered to be the point where endometrium finishes) and the external one, while the whole length of the cervical canal could be observed, thus a symmetric image of the external one can be obtained. Cervical width was measured at the maximal wide point of the cervix along the cervical canal. Uterine length was measured in one segment, in anterior-posterior view from the fundus to the cervix, comprising the whole cervix. In addition, curve lengths were measured as a single linear segment. 084 J. Med. Med. Sci. Figure 1. Two images of the same uterus: one anteverted flexed and one retroverted flexed. Table 1. Uterus measurments by every different uterine position: variance analysis by One-way Anova (values represent mean and standard deviation). Cervical length Cervical width Uterus length Uterus width Anteverted flexed 32.12 (±2.37) 22.48 (±1.6) 75.21 (±2.03) 38.28 (±1.25) On axis 27.2 (±2.12) 25.05 (±4.07) 74 (±1.63) 37.5 (±0.58) Statistical analysis was performed by R (version 2.8.0), considering significant a p<0.05. Oneway Anova, Tukey Honest Significant Differences, and t-test were used to compare mean values, and Kolmogorov-Smirnov test to state the normality of all considered variables. RESULTS Uterus was anteverted flexed on 9 occasions, retroverted flexed on 15, and on axis (not verted nor flexed) on the remaining 4 (Figure 1). Table 1 shows the mean cervical length and its standard deviation by each uterine position. Comparing mean cervical length and width in the different uterine positions, Retroverted flexed 26.76 (±3.8) 25.43 (±3.82) 68.15 (±1.88) 38.4 (±1.88) p <0.05 0.122 <0.05 0.605 they result significantly greater by an anteverted flexed uterus than by a retroverted flexed one (p<0.05), and there is also a significant difference of mean length between an antevertedflexed and an on axis uterus (p<0.05) (Figure 2). Uterus length estimation in anteverted position or on axis position is statistically longer then in retroverted position (p<0.05), while no significant difference has been observed between anteverted uterus and that on axis. Moreover, the uterus width measures show no significant difference between the anteverted position of the uterus, the retroverted one or that on axis. Then, considering that the cervix does not significantly change during cycle and thus in this case we succeed in Londero et al. 085 Figure 2. The mean cervical length with 95% confidence intervals, in the three different positions. excluding all possible variability sources, as the measurements were done on the same cervix by the same gynaecologist and with the same machine, our results suggest a significant difference of the cervical size based on its position and on uterus version-flexion. DISCUSSION Uterine hypermotility is a rare condition, firstly described by Allen and Masters as an intraoperatively diagnosed syndrome characterized by lacerations in the peritoneum and fascia of the broad and cardinal ligaments. These kind of lacerations are described in both multiparous and nulliparous patients, but are mostly associated with pregnancy (Ventolini and Neiger, 2007). We observed a young nullipara nulligravida with uterine hypermotility of casual ultrasonographic diagnose. The literature demonstrates the ultrasonographic measurment of cervix to be an accurate method to estimate the cervical length in the case of anteverted uterus (Jackson et al., 1992), but also admits an underestimation of ultrasonographic measurement in the case of curved cervix (To et al., 2001).With our case, we demostrate the significant difference between the estimation of cervical length in anteverted and retroveted position of the uterus, in the same patient and consequently the same cervix. Although we cannot yet surely say if there is an overestimation of cervical length by means of an anteverted flexed uterus or an under-estimation due to a retroverted flexed one, we can suppose an underestimation of cervical length in retroverted uterus position, because of a more important curvature of the cervix in the most occasions of retroverted uterus. In the literature no static evaluation of cervical length has been able to identify yet the women who have delivered preterm or that will be at risk for preterm delivery (Pardo et al., 2003), and actually we think that a dynamic evaluation of cervix during early pregnancy would be more appropriate in this perspective. In fact, based on previous studies (Londero et al., 2010; Berghella et al., 2003), we suppose that in the first part of pregnancy there is a dynamic evolution of cervix, and in particular that the cervical length progressively increases due to physiologic modifications (Zemlyn, 1981). Therefore, it is important to acknowledge such an evolution in order to critically evaluate cervical length by predicting the risk of preterm delivery in case of a retroverted flexed uterus. The difference observed between the uterus length between the anteverted and the retroverted position may be interpreted in the same way as cervical length in these 086 J. Med. Med. Sci. positions, and we consequently suppose an underestimation also of uterus length in its retroverted position. An important limitation of our study is that we evaluated a single patient, and this it is due to the rarity of the clinical characteristics of the observed patient. On the other hand, this limitation represents also a strength point of our research, because we could exclude every biological variation of cervical length, which may exist between the different individuals. Moreover, we took in consideration every factor which may affect measurement variability, such as uterine position and cycle phase, and we reduced every possible confounding factor such as operator or machine variability. In particular, we choose a single operator and a standard method to measure the cervix, even if we did not test the inter-operator variability of measurements, because the main aim of the study was to test the differences in estimation of cervical length by changing the uterus position. Conclusion In conclusion, we found a significant difference of cervical size based on its position and on uterus version-flexions, which suggests a possible under-estimation of cervical length in case of retroverted uterus. REFERENCES Berghella V, Talucci, M,Desai A (2003). Does transvaginal sonographic measurement of cervical length before 14 weeks predict preterm delivery in high-risk pregnancies? Ultrasound Obstet. Gynecol. 21(2), 140–144. Jackson GM, Ludmir J, Bader TJ (1992).The accuracy of digital examination and ultrasound in the evaluation of cervical length. Obstet. Gynecol. 79(2), 214–218. Londero AP, Bertozzi S, Fruscalzo A, Driul L, Marchesoni D (2010). Ultrasonographic assessment of cervix size and its correlation with female characteristics, pregnancy, bmi, and other anthropometric features. Arch. Gynecol. Obstet.[Epub ahead of print] PMID: 20145939 Ozdemir I, Demirci F, Yucel O, Erkorkmaz U (2007).Ultrasonographic cervical length measurement at 10-14 and 20-24 weeks gestation and the risk of preterm delivery. Eur. J. Obstet. Gynecol. Reprod. Biol. 130(2), 176–179. Pardo J, Yogev Y, Ben-Haroush A, Peled, Y, Kaplan,B, Hod, M (2003).Cervical length evaluation by transvaginal sonography in nongravid women with a history of preterm delivery. Ultrasound Obstet. Gynecol. 21(5), 464–466. Smith GCS, Celik E, To M, Khouri O, Nicolaides KH, Group FMFSTS (2008).Cervical length at mid-pregnancy and the risk of primary cesarean delivery. N Engl. J. Med. 358(13):1346–1353. Theron G, Schabort C, Norman K, Thompson M, Geerts L (2008). Centile charts of cervical length between 18 and 32 weeks of gestation. Int. J. Gynaecol. Obstet. 103(2), 144–148. To MS, Skentou C, Chan C, Zagaliki A, Nicolaides KH (2001). Cervical assessment at the routine 23-week scan: standardizing techniques. Ultrasound Obstet. Gynecol. 17(3):217–219. Ventolini G, Neiger R (2007). Allen-masters syndrome detected at the time of a cesarean delivery: A case report and a review of the literature. J. Gynecol. Surg. 23(3):117-120. Zemlyn S (1981).The length of the uterine cervix and its significance. J. Clin. Ultrasound 9(6):267–269.