IGRT and SBRT Programs with
advertisement

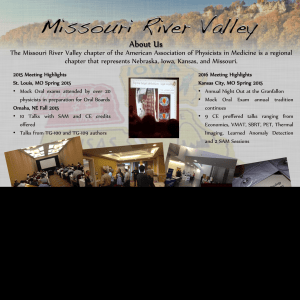
IGRT and SBRT Programs with Siemens Accelerators and ExacTrac Stereoscopic XX-ray System Linear Accelerators with features specifically suitable for SBRT Dimitris Mihailidis Mihailidis,, Ph.D. Charleston Radiation Therapy, Charleston, Charleston, West Virginia * Slide courtesy of Brian Kavanagh / University of Colorado Introduction and Purpose QUESTION: Can Stereoscopic x-Ray IG Technology convert a conventional Siemens (Primus or Oncor) linac into a “precision” IG - SBRT delivery machine ? Description of the Systems Implement Image Guidance (IG) on a Siemens Linac (Primus or Oncor). Necessary components to include for IG upgrade. Compatibility of components to provide an IG solution. Transition to an SBRT program. Siemens PRIMUS with ExacTrac System Infrared camera BrainLab ExacTrac System: Two X-ray tubes. Two amorphous silicon detectors (20x20 cm2). Infrared Polaris system. Touch screen and arm. 512x512 Matrix X-Ray phantom. ISO phantom. Rando pelvis phantom. Reference star or markers. Imaging panels In-room monitor X-ray tube 1 TG-142 requirements for IMRT & SBRT: Mechanical and radiation isocenter verification: Siemens linac preparation Gantry rotation (<1mm diameter) Collimator rotation (<1mm diameter) Table rotation (<1mm diameter) MLC system Quality Assurance: Leaf position repeatability (± (±1mm Oncor or ±2mm Primus) Leaf positional accuracy (1mm at cardinal gantry angles) Radiation vs. Light coincidence (1mm). Collimator rotation – radiation isocenter X-Jaws 0.19 mm Gantry rotation – radiation isocenter X-Jaws 1.02 mm Y-Jaws 0.06 mm Y-Jaws 0.04 mm Table rotation – radiation isocenter X-Jaws 0.44 mm Y-Jaws 0.41 mm 2 MLC picket fence test for Siemens Have strong and frequent engineering support ! Scan direction Scan direction 2 cm center-to-center The Technology at CRTC for SBRT • Siemens Primus and Oncor Linacs. • Philips large bore CT simulator (4D-CT capability). • Philips Pinnacle3 Treatment Planning System. • BrainLab ExacTrac 6D-Stereoscopic X-ray Image Guidance System. Move on with SBRT Utilize more accurate patient immobilization devices. Utilized 4D-CT simulation for appropriate sites (e.g., lung, liver, etc), ITV approach. Utilized highly conformal multi-beam treatment planning and intensity modulation. Utilized image guidance for patient daily setup. Utilized on-line patient surveillance and setup correction during treatment. Utilized 5 and 10 mm MLC width for delivery. Small field size measurements Planning System Commissioning Philips Pinnacle3 v8.0m with DMPO in step--andstep and-shoot mode. BEAM MODEL Model fit to the data 3 Small field size measurements Detectors for small field measurements 1.00 OUTPUT FACTORS 0.90 0.80 0.1cc Scanning IC 0.70 Diode Perp. (norm to 5x5) Microchamber 0.60 XV Film Small fields-MLC shaped Pinnacle Hi Res 0.50 0.40 0.00 Pinnacle Lo Res 0.50 1.00 1.50 2.00 2.50 3.00 3.50 4.00 4.50 5.00 Direct Machine Parameter Optimization • DMPO produces final segments at the end of the optimization process. NO conversion is required. Automatically converts the ODM to MLC control points. • The MLC leaf positions and the weights of the segments are optimized at once (equivalent to DAO). • The time to prepare a plan is substantially reduced in DMPO. • You can filter the final control points according to area and monitor units. How important is the MLC system in multi--beam SBRT treatment planning? multi DMPO Dosimetric Comparison of MLC systems Linac MLC system MLC width Siemens Primus (X-jaws) Optifocus double-focused (divergent) - 58 leaves 10 mm Siemens Oncor (X-jaws) Double-focused (divergent)- 82 leaves 10 mm Siemens Artiste (X-jaws) 160MLC (rounded) - 160 leaves 5 mm Varian Trilogy (tertiary) Millennium (rounded) - 120 leaves 5 mm Beam Modulator (rounded) - 80 leaves 4 mm Elekta MLC (rounded) - 80 leaves 10 mm HD micro-MLC – 120 leaves 2.5 mm Elekta Synergy-S BM Elekta Synergy Novalis TX (tertiary) Method of comparison “RING”: A special ring-structure around the TV, 1 cm expansion of the TV – to evaluate the sparing of normal structures adjacent to TV. ________________________________________________________________ Paddick, J. Neurosurg. (Suppl. 3) 93:219-222, 2000 CONFORMITY INDEX: CI = ( PIV / PVTV ) / ( PVTV / TV ) CI = 1, perfect conformity TV = target volume PIV = prescription isodose volume PVTV = is the TV included in PIV Nakamura JL, et al., Int. J. Radiat. Oncol. Biol. Phys. 51, 1313-1319 (2001). The IL was chosen according to the criteria: (1) being the greatest IL that covers 95% of TV while (2) delivering ≥95% of the prescription dose to 99% of the TV. 4 Comparison: Conformity Index Comparisons: 3D conformal vs. Intensity Modulation Oncor (10mm) Artiste (5mm) Varian (5mm) NovalisTX (2.5mm) Synergy (10mm) SynergyBM (4mm) Conformity Index (CI) 2.5 Peri-tunoral Ring Volume 4.64 cc Lung target Oncor (10mm) Artiste (5mm) Varian (5mm) 120 NovalisTX (2.5mm) Synergy (10mm) 2 100 CI V olum e (% ) 1.5 1 0.5 SynergyBM (4mm) 80 60 40 20 0 0 4.64 (Lung-3D) 4.64(Lung-IM) 7.63(Brain-IM) 9.85(Lung-3D) 50%(IM) 25.78(Spine-IM) 80%(IM) 90%(IM) 50%(3D) 80%(3D) 90%(3D) Isodose line Target Volume (cc) 3D-CRT vs. Intensity Modulation Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 Comparison: MLC systems Comparison: Lung IMRTIMRT- all MLC systems LUNG: 3D CRT 100% Rx 90% Rx 10mm 80% Rx 10mm 5mm 50% Rx Oncor: 10 mm Novalis TX: 2.5 mm 4500 cGy 5mm 2.5mm 4mm 4275 cGy 3600 cGy Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 Conclusions of comparisons 5mm Varian 2.5mm Novalis TX SBRT – LUNG Our study is the first to include the majority of today’s MLC systems in a comprehensive way and has shown no apparent indication that smaller MLCs can lead to optimal plans, if multi-field techniques (IMRT or 3D) are utilized in SBRT. However, we believe that small tumor volumes would benefit from small MLC widths and single fraction SRS, instead. Tanyi, JA, Radiation Oncology 4:22 (2009) NO – GATING! WHY ? Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 5 4D CT Simulation for LUNG SBRT Patient Immobilization With arms over the head. Flat lung board with T-bar holder for the arms. CT Scanning procedure for moving target One free breathing scan – 3 mm slices, entire chest. One shorter, time-correlated scan – 3 mm slices, to include the tumor area. Breathing Waveform is acquired along with CT data using a Bellows or RPM device. The CT data acquired in one breath can be binned into 10 equally spaced intervals along the waveform and reconstructed. The 10 intervals are called Phases. Vacuum Bag Maximum Intensity Projection (MIP) CT data is acquired using a Bellows or RPM device that records a breathing wave. Maximum intensity values are assigned to pixels at locations where a tumor moves to over time. Are a derived dataset of images that show a “composite” of the tumor volume over the time period that the CT data was acquired. Moving Target virtual simulation - Fusion MIP dataset Volume propagation from MIP dataset to free breathing dataset GTV ITV Free Breathing dataset 6 Treatment planning Allow for lowlow-level Intensity Modulation Multiple non-coplanar beams Step-and-shoot mode: • 2-3 segments per beam. • 50Gy in 5 fxs. • Optimization objectives -heart -ribs -normal tissues PTV=ITV + 5mm margin Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 www.charlestonradiation.com DMPO - optimization DVH results WE HAVE NOTICED: 2-3 segments allow for dose compensation due to lack of resolution of the 10mm leaf width. PTV50Gy ITV Ipsilateral lung Mihailidis, et al., AAPM 2009, Med. Phys. 36, (2009) 2660 www.charlestonradiation.com ExacTrac setup for lung SBRT Treatment Isocenter Virtual isocenter for IG ET reconstructed views SBRT - LUNG Patient setup verification prior to treatment IMAGE GUIDANCE 7 Fusion preparation Before Fusion - misalignment ET x-ray Excluded from fusion area DRR After fusion – shifts to be implemented Match of x-ray and DRR SBRT - Brain SHIFTS Patient setup and immobilization Fusion MRI – TP CT ExacTrac IR markers TP CT www.charlestonradiation.com MRI Vargo J, Plants B, Welch C, Mihailidis D, et al., ASTRO 2010, IJROBP 78 (No. 3 Suppl), S279 (2010) 8 Sample isodose and DVH SBRT brain positioning and planning Prescription: 40 Gy in 5 fxs 788 MU objectives Multiple non-coplanar beams Vargo J, Plants B, Welch C, Mihailidis D, et al., ASTRO 2010, IJROBP 78 (No. 3 Suppl), S279 (2010) PTV Vargo J, Plants B, Welch C, Mihailidis D, et al., ASTRO 2010, IJROBP 78 (No. 3 Suppl), S279 (2010) Patient setup with IR markers SBRT - BRAIN Patient setup verification prior to treatment IR marker IMAGE GUIDANCE from TPS www.charlestonradiation.com Fusion Continuous IG BEFORE DRR Allow for live patient survaillance with the IR camera and markers. Perform a second IG verification between treatment fields (residual shifts). Compare reference orthogonal treatment ports with orthogonal DRRs. Keep rotations to less than 3° if possible, otherwise…improvise. SHIFTS DRR x-ray x-ray Wood Shims AFTER www.charlestonradiation.com www.charlestonradiation.com 9 6D-corrections and residual setup errors 6D-IGRT accuracy: Infrared vs. stereoscopic x-ray Comply with published recommendations: Conclusions ExacTrac Stereoscopic x-Ray IG system, in combination with other technologies, provides accurate IG that allows the implementation of an SBRT program, IF additional precautions are taken. 10 THANK YOU ! NRAO Green Bank Observatory, West Virginia http://www.gb.nrao.edu/ 11