Document 14183209
advertisement

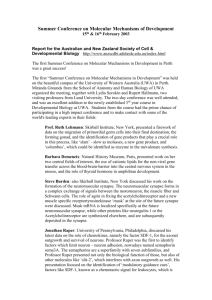
0963-6897/10 $90.00 + .00 DOI: 10.3727/096368909X481782 E-ISSN 1555-3892 www.cognizantcommunication.com Cell Transplantation, Vol. 19, pp. 399–408, 2010 Printed in the USA. All rights reserved. Copyright 2010 Cognizant Comm. Corp. Continuous Delivery of Stromal Cell-Derived Factor-1 From Alginate Scaffolds Accelerates Wound Healing Sina Y. Rabbany,*†1 Joseph Pastore,‡1 Masaya Yamamoto,†§ Tim Miller,‡ Shahin Rafii,†¶ Rahul Aras,‡ and Marc Penn‡# *Bioengineering Program, Hofstra University, Hempstead, NY, USA †Department of Genetic Medicine, Howard Hughes Medical Institute, Weill Cornell Medical College, New York, NY, USA ‡Juventas Therapeutics, Inc., Cleveland, OH, USA §Department of Biomaterials, Institute for Frontier Medical Sciences, Kyoto University, Kyoto, Japan ¶Howard Hughes Medical Institute, Weill Cornell Medical College, New York, NY, USA #Department of Stem Cell Biology and Regenerative Medicine, Cleveland Clinic, Cleveland, OH, USA Proper wound diagnosis and management is an increasingly important clinical challenge and is a large and growing unmet need. Pressure ulcers, hard-to-heal wounds, and problematic surgical incisions are emerging at increasing frequencies. At present, the wound-healing industry is experiencing a paradigm shift towards innovative treatments that exploit nanotechnology, biomaterials, and biologics. Our study utilized an alginate hydrogel patch to deliver stromal cell-derived factor-1 (SDF-1), a naturally occurring chemokine that is rapidly overexpressed in response to tissue injury, to assess the potential effects SDF-1 therapy on wound closure rates and scar formation. Alginate patches were loaded with either purified recombinant human SDF1 protein or plasmid expressing SDF-1 and the kinetics of SDF-1 release were measured both in vitro and in vivo in mice. Our studies demonstrate that although SDF-1 plasmid- and protein-loaded patches were able to release therapeutic product over hours to days, SDF-1 protein was released faster (in vivo Kd 0.55 days) than SDF-1 plasmid (in vivo Kd 3.67 days). We hypothesized that chronic SDF-1 delivery would be more effective in accelerating the rate of dermal wound closure in Yorkshire pigs with acute surgical wounds, a model that closely mimics human wound healing. Wounds treated with SDF-1 protein (n = 10) and plasmid (n = 6) loaded patches healed faster than sham (n = 4) or control (n = 4). At day 9, SDF-1-treated wounds significantly accelerated wound closure (55.0 ± 14.3% healed) compared to nontreated controls (8.2 ± 6.0%, p < 0.05). Furthermore, 38% of SDF-1-treated wounds were fully healed at day 9 (vs. none in controls) with very little evidence of scarring. These data suggest that patch-mediated SDF-1 delivery may ultimately provide a novel therapy for accelerating healing and reducing scarring in clinical wounds. Key words: Dermal delivery; Tissue remodeling; Neovascularization; Tissue scarring; Hydrogels INTRODUCTION the principal cells involved in stimulating blood vessel growth. In response to injury, these cells initiate the angiogenic process, which eventually leads to remodeled tissue and a newly formed vasculature. There are many therapies directed at accelerating wound healing, such as the application of electric currents, living skin equivalents, and pharmacological manipulation of factors that modulate the wound-healing process. However, few treatments are able to combine the ability to improve wound healing with ease of transport and efficacy in a cost-effective manner. Furthermore, there are limited Wound healing is a complex and coordinated series of events involving inflammation, tissue deposition, remodeling, and scarring. In the epidermis, this is a dynamic process involving multiple skin layers, specifically the interaction of infiltrative cells (leukocytes, progenitor cells) with the underlying stroma (keratinocytes, endothelial cells, epithelia, extracellular matrix) (26). Angiogenesis is one of the important events during wound healing, and microvascular endothelial cells are Received April 30, 2009; final acceptance December 2, 2009. Online prepub date: December 8, 2009. 1These two authors contributed equally. Address correspondence to Marc Penn, Department of Stem Cell Biology and Regenerative Medicine, Cleveland Clinic, Cleveland, OH, 44195, USA. Tel: (216) 444-6697; E-mail: pennm@ccf.org or Sina Y. Rabbany, Department of Genetic Medicine, Weill Cornell Medical College, New York, NY 10021, USA. Tel: (212) 746-7014; E-mail: sir2007@med.cornell.edu 399 400 studies that directly compare gene- and protein-based biological delivery in order to define optimal delivery strategies. Dermal Delivery of Biologic Material Alginate hydrogels have proven to be useful scaffolds for tissue engineering and delivery vehicles for drug treatments. Hydrogels can be loaded with a variety of growth factors for controlled release during different wound-healing stages and in light of wound severity. Furthermore, alginate gels and patches are extremely versatile and can be tailored to account for the stiffness, swelling, cell attachment, or degradation of bioreactive polymers (3). Improving the rate of dermal wound healing has been identified as a target for demonstrating the therapeutic potential of growth factor delivery. A number of factors have been identified that mediate wound healing and promote proliferation and differentiation of skin cells, such as platelet-derived growth factor (PDGF) and epidermal growth factor (EGF) (20). Our study focused on stromal cell-derived factor-1 (SDF-1), a naturally occurring chemokine that is rapidly overexpressed in response to tissue injury, particularly during ischemia, to expedite wound closure and decrease scar formation (2,15). SDF-1 plays an important role in the migration, recruitment, and retention of endothelial progenitor cells (EPCs) to the site of injury, hence contributing to neovascularization. Findings from multiple independent studies suggest that inducing SDF-1 expression at a wound site has therapeutic potential to promote rapid repair of hard-to-heal wounds, such as deep incisions, ulcerations, and burns (5,6,10). Therapeutic Applications of SDF-1 A unique aspect of wound healing in adult tissue is that regeneration is generally driven by environmental stimuli and is often initiated by local release of chemokines. SDF-1 treatment has been shown to reduce wound size by recruiting progenitor cells to the site of injury, promoting full reepithelialization of the wound and enhancing revascularization of the damaged tissue. A prominent feature of this treatment is the decreased amount of tissue scarring, a particularly important feature that will increase the health, mobility, and well-being of patients. The beneficial effects of SDF-1 treatment are well characterized in cardiovascular models of ischemia and hypoxic stress (7,30). Similarly, dermal wounds may be a particularly relevant therapeutic target for SDF-1 therapy due to the ability of SDF-1 to recruit EPCs and epithelial cells and thus accelerate natural wound repair. Importantly, SDF-1 treatment has been shown to accelerate wound healing. In two studies, direct injection of SDF-1 protein or lentivirus significantly reduced wound size after 1 week in diabetic mice (5,11). We therefore RABBANY ET AL. hypothesized that slow-release delivery of either SDF-1 protein or plasmid expressing SDF-1 would increase the rate of wound closure in a porcine model of full-thickness dermal wound healing. We employed a clinically relevant delivery system, an alginate scaffold, to deliver SDF-1 plasmid or protein over time to acute surgical wounds. In this article, we characterized SDF-1 plasmid or protein dermal delivery using alginate scaffolds in vitro and demonstrate the potential for therapeutic benefit in vivo by using the scaffolds to deliver the SDF-1 protein and plasmid to acute surgical wounds. MATERIALS AND METHODS Construction of Honeycomb Alginate Patches Chemicals were obtained from Nacalai Tesque. Inc. (Kyoto, Japan), Calbiochem (La Jolla, CA, USA), BD Biosciences (Franklin Lakes, NJ, USA), and Sigma Chemical Co. (St. Louis, MO, USA) and used without further purification. Alginate gels were prepared according to the method described previously (8). Briefly, sodium alginate (MW, 110k, Wako Pure Chemical Industry, Osaka, Japan) was dissolved at different concentrations in distilled water. The inner wall of glass beakers was coated with a thin layer of sodium alginate and dried at 110°C for 0.5 h. An aqueous solution of sodium alginate was poured into the alginate-coated beaker and calcium chloride solution was sprayed until a thin alginate gel layer was formed on the top of the sodium alginate solution. Then, calcium chloride solution was added on the thin gel layer, followed by overnight incubation at room temperature to complete gelation. This ionotropic gelation generated parallel channel-like pores in alginate gels, which were subsequently washed with deionized water to remove free calcium ions. The resulting gels were frozen at −80°C, lyophilized under vacuum at room temperature for 2 days to form a honeycomb structure, cut into 5 mm diameter/2 mm thick disc-shaped units, and subjected to further chemical modifications. Alginate discs were immersed in 2-(N-morpholino) ethanesulfonic acid (MES) buffer (0.2 M, pH 6.0) containing ethylenediamine (ED, 5.17 mM), NHS (114 mM), and 1-ethyl-3-(3-dimethylaminopropyl) carbodiimide (EDC, 305 mM) and centrifuged at 1500 rpm for 5 min to eliminate air bubbles. After 24 h of cross-linking, the resulting gels were washed with phosphatebuffered saline (PBS) three times. Radioiodination of SDF-1 Protein Human recombinant SDF-1 was radioiodinated according to the method of Greenwood et al. (12). Briefly, 10 µl of Na125I solution was added to 40 µl of 0.1 mg/ ml SDF-1 solution, followed by the addition of 0.2 mg/ ml of chloramine-T potassium phosphate-buffered solution (0.5 M, pH 7.5) containing 0.5 M sodium chloride ALGINATE SCAFFOLDS AS DELIVERY VEHICLE FOR SDF-1 IN INJURY (100 µl). After agitation at room temperature for 2 min, 100 µl of PBS solution (pH 7.5) containing 0.4 mg of sodium metabisulfate was added to the reaction solution to stop the radioiodination. The reaction mixture was passed through an anionic-exchange column to remove the uncoupled, free 125I molecules from the 125I-labeled SDF-1 protein. Radioiodination of SDF-1 Plasmid DNA PBS containing 1.5 mg/ml of SDF-1 plasmid DNA (1.33 ml) was added to the 125I-Bolton-Hunter reagent nitrogen dried. The resulting solution was kept at room temperature for 6 h to introduce 125I residue into the amino groups of SDF-1 plasmid DNA. Noncoupled, free 125 I-labeled reagent was separated from 125I-labeled SDF1 plasmid DNA by gel filtration with a PD-10 column (Amersham Pharmacia Biotech K.K, Tokyo, Japan). Preparation of Alginate Patches Incorporating I-Labeled SDF-1 Protein or 125I-Labeled SDF-1 Plasmid DNA Cross-linked alginate patches were immersed into 0.015 M spermine chloride/MES buffer solution containing NHS (114 mM) and EDC (305 mM), and stored at room temperature overnight. Unbound spermine chloride was removed by washing with PBS and distilled water. After lyophilization, the spermine-immobilized patch was sterilized with 70% ethanol and air dried in an aseptic tissue culture hood. An aqueous solution (20 µl) of 125I-labeled SDF-1 protein (1.0 ng/µl) containing sodium heparin (1 U/µl) was dropped onto the sterilized scaffolds and incubated at 4°C overnight to complete protein incorporation. Similarly, 15 µl of an aqueous solution of 125I-labeled SDF-1 plasmid (1.0 mg/ml) was dropped onto the sterilized scaffolds and incubated at 4°C overnight to complete plasmid DNA incorporation. 125 In Vitro Evaluation of SDF-1 Protein and Plasmid DNA Release From Alginate Patches An alginate patch saturated with 125I-labeled SDF-1 protein or plasmid DNA was placed in 1 ml of PBS containing bovine serum albumin fraction V (BSA, 0.1 mg/ml), followed by incubating at 37°C. The supernatant was periodically sampled to measure the radioactivity of released 125I-labeled SDF-1 protein or plasmid DNA by a gamma counter (ARC-380, Aloka Co., Ltd., Japan). Fresh BSA solution of the same volume was added to continue the release test. In Vivo Evaluation of SDF-1 Protein and SDF-1 Plasmid DNA Release From Alginate Patches in Rodents Alginate patches incorporating 125I-labeled SDF-1 protein or plasmid DNA were implanted subcutaneously 401 into the backs of 6-week-old female ddY mice (Shimizu Laboratory Supply Inc., Japan) at the central position 15 mm away from their tail root. At different time intervals, the mouse skin including the implanted site of the sponge (3 × 5 cm) was excised and the corresponding fascia was thoroughly wiped off with a filter paper to absorb 125I-labeled SDF-1 protein or plasmid DNA. The radioactivity of the patch, the excised skin strip, and the filter paper were measured on a gamma counter (ARC380) to assess the time profile of in vivo SDF-1 protein and plasmid DNA release. The experimental group was composed of three mice unless otherwise mentioned. The use of animals in this study was approved by MPI’s Research Institutional Animal Care and Use Committee (IACUC) prior to starting, and was based on current International Conference on Harmonisation (ICH) Tripartite Guidelines. Porcine Surgical Wound Healing Model and Antemortem Follow-up A standard model of acute surgical wound healing was performed in domestic Yorkshire pigs. A cuffed endotracheal tube was placed and general anesthesia was maintained with isoflurane delivered in oxygen through a rebreathing system with ventilator assist. Each animal received 12 full-thickness 5-cm incisions (six on each side of the spine) spaced approximately 7.5 cm apart. Each incision was made perpendicular to the spine, starting 7.5 cm from the spine and cutting toward the abdomen. Gauze was placed in the incision until the bleeding stopped. The gauze was removed, and the incision was sutured closed. Alginate patches (1 × 6 cm) incorporating SDF-1 protein, plasmid DNA, or PBS were applied to wounds. Scaffolds were prepared with a solution of plasmid encoding human SDF-1 in a pcDNA3.1 backbone (Invitrogen Corporation, Carlsbad, CA, USA) by mixing 3.5 mg of the SDF-1 plasmid in 2.33 ml PBS to create a 1.5 mg/ml solution. For the SDF-1 protein scaffolds, a solution was prepared by mixing 10 µg of carrier-free SDF-1 protein (R&D Systems, Minneapolis, MN, USA) with 5 ml PBS and 3 ml of 1000 IU/ml injection heparin (Baxter Healthcare Corporation, Deerfield, IL, USA) to create a 1.5 µg/ml solution. PBS scaffolds served as a negative control and were prepared by mixing 1.35 ml PBS and 0.45 ml of 1000 IU/ml injection heparin. On each scaffold, the loading solution was pipetted under sterile conditions onto the scaffold in six equally spaced 60-µl drops (360 µl total) so that each drop covered a 1-cm2 area of the scaffold. All loaded scaffolds were stored at 4°C for 12 h prior to wound application. Following wound closure, the scaffold was placed next to the wound and photographed. The scaffold placement order was randomized with the following dis- 402 tribution: SDF-1 protein (n = 10), SDF-1 plasmid (n = 6), PBS (n = 4), or sham (no scaffold, n = 4) wounds. The scaffold was placed over the wound (except in the sham group), and each wound was dressed with a Tegaderm patch. To determine the effect of SDF-1 on the rate of wound healing, wound length was measured by the same veterinarian at day 0 (prior to scaffold placement) and prior to sacrifice. Wound length was converted to percent healing by the following equation: (initial wound length − final wound length)/(initial wound length) × 100%. To monitor the time course of the effects of SDF-1 on wound healing, the first pig was sacrificed at 4 days and the second pig was sacrificed at 9 days. RABBANY ET AL. formed using Microsoft Office Excel 2007 (Microsoft, Redmond, WA, USA). RESULTS SDF-1 Protein and Plasmid Release Characteristics Release characteristics of radioiodinated SDF-1 protein and plasmid from alginate scaffolds are shown in Figure 1. SDF-1 protein and plasmid release in vitro was measured at multiple time points over 150 h (Fig. 1A). The scaffolds released approximately 40–60% of plasmid or protein SDF-1 within the first day, with Kd of 24.5 and 15.8 h, respectively. Thereafter, SDF-1 plasmid continued to be released, whereas SDF-1 protein release was minimal after 24 h. Because neither the SDF-1 plas- Postmortem Follow-up Following sacrifice, one section from the middle of each wound site was excised for histopathological and immunohistochemical analysis. Standard hematoxylin and eosin (H&E) stain was used to assess extent of fibroplasia, inflammation, and necrosis at day 4 and necrosis, fibrosis, and granulomatous inflammation at day 9. Each parameter was graded on a qualitative scale by a histopathologist blinded to randomization as either: none (not present), minimal, mild, moderate, or severe. Immunohistochemical staining was performed on the same tissue section. The effect of SDF-1 on fibroblast infiltration into the wound was detected by vimentin staining. Vimentin is a type III intermediate filament often expressed in epithelial cells undergoing mesenchymal transition. The effect of SDF-1 on blood vessel formation was determined by CD31 and the presence of smooth muscle was detected by smooth muscle actin staining. CD31, also known as platelet endothelial cell adhesion molecule 1 (PECAM1), is a type I integral membrane glycoprotein and a member of the immunoglobulin superfamily of cell surface receptors. It is constitutively expressed on the surface of endothelial cells and concentrated at the junction between them. CD31 has been used to measure angiogenesis and can be used as a marker for myeloid progenitor cells. Smooth muscle α-actin is used because it is one of a few genes whose expression is relatively restricted to vascular smooth muscle cells. The amount of each stain per sample was graded by the same pathologist using the same qualitative scale as above. Statistical Analysis All data are presented as mean ± SEM. Comparisons between groups were performed using a Student’s t-test. A value of p < 0.05 was considered statistically significant. For SDF-1 release data, a logarithmic curve was fit to each data set. All statistical analyses were per- Figure 1. Characterization of SDF-1 release from alginate scaffolds in vitro and in vivo. Scaffolds were loaded with radioiodinated protein (squares) or plasmid (diamonds) and release was measured in vitro (A) by quantifying radioactivity from the supernatant at multiple time points or in vivo (B) from filter paper wiped along the fascia of scaffolds implanted subcutaneously at the base of the neck in mice. Dotted lines indicate the time points at which 50% of the plasmid or protein was dissociated (Kd) from the scaffold. ALGINATE SCAFFOLDS AS DELIVERY VEHICLE FOR SDF-1 IN INJURY 403 mid nor protein reached 100% release at 1 week, we ensured the patches retained the originally loaded SDF1 by detaching the remaining protein or plasmid from the patch by soaking in a high salt solution (data not shown), suggesting that release may have reached equilibrium with the supernatant. This indicated that subcutaneous scaffold application in vivo may sustain plasmid and protein release over time, and may be effective release of therapeutic vectors or proteins. To test this hypothesis in vivo, SDF-1 plasmid and protein scaffolds were implanted subcutaneously into the backs of 6-week-old ddY female mice and evaluated for release over 2 weeks (Fig. 1B). The in vivo profile of SDF-1 protein release was similar to the in vitro profile, as the majority of the SDF-1 protein was released within the first day (Kd, 0.55 days) compared to the in vivo release of SDF-1 plasmid, which demonstrated a slower release profile (Kd 3.67 days). Dissociation values are presented in Table 1. The total amount of SDF1 plasmid released initially was significantly lower than that of protein for the first 6 days, while the amount remaining after 2 weeks was similar. Based on these release characteristics, we tested the effects of SDF-1 treatment in a well-characterized porcine model of dermal wound healing. SDF-1-Releasing Scaffold Accelerates Wound Healing Recent work from several laboratories suggests that SDF-1 has therapeutic potential for treating hard-to-heal wounds complicated by diabetes or burns (4,5,10,19,29). We hypothesized that SDF-1 treatment would increase the rate of healing in acute dermal wounds, such as those received after surgery. Therefore, 5-cm-long full-thickness incisions were made on the backs of Yorkshire pigs and covered with Tegaderm alone or scaffolds soaked with PBS, SDF-1 plasmid, or SDF-1 protein to assess the effect of SDF-1 treatment on the rate of dermal wound closure. The impact of SDF-1-releasing scaffolds on wound healing is shown in Figure 2. Wounds treated with either SDF-1 plasmid or protein scaffolds (Fig. 2A, solid markers and lines) trended towards accelerated wound healing by day 4 and demonstrated a significantly higher rate of wound closure compared to control wounds at day 9 post-scaffold application (Fig. 2A, dotted lines). Grouped data (Fig. 2B) demonstrate that SDF-1 treat- Table 1. Kd Values for SDF-1 Patch Release In vitro In vivo Plasmid Protein 24.5 h 3.67 days 15.8 h 0.55 days Figure 2. SDF-1 treatment accelerates healing of acute surgical wounds. (A) Percent wound healing over time shown for SDF-1 plasmid (squares) or protein (diamonds) treated wounds and nontreated saline (triangles) or sham (crosses) in a porcine model of acute dermal wound closure. (B) SDF-1treated groups (n = 8) healed to a much greater extent compared to nontreated controls (n = 4). *p < 0.05. ment significantly accelerated wound closure (55.05 ± 14.36%) compared to controls (8.14 ± 5.96%, p < 0.05). Representative examples of wounds treated with PBS (Fig. 3A, D, G), SDF-1 protein (Fig. 3B, E, H), or SDF1 plasmid (Fig. 3C, F, I) scaffolds at day 0 (top panel) and day 9 (bottom panel) are shown. At day 9, the wound treated with the control scaffold was still apparent, whereas there was no visible evidence of the SDF-1 protein- and SDF-1 plasmid-treated wounds (Fig. 3G–I). Notably, one of three SDF-1 plasmid-treated wounds and two of five SDF-1 protein-treated wounds are 100% healed at 9 days (Fig. 3J). SDF-1 has previously been shown to cause neovascularization (21,30) and promote homing of progenitor cells (11,28). It is recently appreciated that SDF-1 may also be important in regulating the wound-healing response in skin (23,26,27). Interestingly, macroscopic wound evaluation by a pathologist blinded to treatment group indicated that scar formation varied between wounds. Therefore, we investigated the impact of SDF-1 404 RABBANY ET AL. Figure 3. SDF-1 treatment reduces scar formation in dermal wounds and increases wound closure. Representative images of wounds that received scaffolds containing PBS control (A, D), SDF-1 protein (B, E), or plasmid (C, F) at day 0 prior to scaffold placement or on day 9 after scaffold removal. All full-thickness wounds are 5.0 ± 0.1 cm. (G–I, 2×) Wounds that received SDF-1 treatment demonstrated less visible scarring compared to controls and had a higher percentage of fully healed wounds (J). ALGINATE SCAFFOLDS AS DELIVERY VEHICLE FOR SDF-1 IN INJURY on fibroblast infiltration, smooth muscle, and new blood vessel formation, using immunohistochemical staining for vimentin (Fig. 4A–H), smooth muscle actin (Fig. 4I–L), and PECAM-1 (CD31) (Fig. 4K–O), respectively. A slight increase in vimentin staining was observed in PBS-treated compared to SDF-1-treated wounds, which may reflect differences observed in scar formation. There were no substantial differences in the amount of CD31 or smooth muscle actin staining compared between treatment groups. H&E analysis showed a slight decrease in fibrosis in the SDF-1 protein- and plasmid-treated wounds compared to control or sham wounds (Fig. 5A). Similarly, a slight increase in granulotamous inflammation was observed in control groups, 405 but no difference was observed in subacute/chronic inflammation or necrosis between groups (Fig. 5B–D). DISCUSSION Wound dressings capable of delivering proangiogenic factors play a vital role in the early healing process, by leaving wounds from being undisturbed and keeping wounds intact at body temperature, giving the body a chance to heal by recruiting the much needed blood supply. In this study, we demonstrated that a novel wound dressing, an alginate scaffold releasing the proangiogenic molecule SDF-1, accelerated the wound-healing process in a clinically relevant animal model of acute surgical wound healing. Furthermore, we characterized Figure 4. Immunhistochemical analysis of wounds treated with SDF-1 or PBS scaffolds. Representative images of immunohistochemical staining demonstrating that SDF-1 treatment decreased vimentin staining (A–D, 40×; E–H, 2×) in the wound scar. The smooth muscle actin (I–K, 40×) illustrates lower level of remodeling in both SDF-1 protein and plasmid group in comparison with PBS control. CD31 staining (L–P, 40×) also shows less vascularization in the SDF-1 groups compared with the PBS control. 406 RABBANY ET AL. Figure 5. Scaffold application does not adversely affect wound healing. Microscopic evaluation of dermal tissue at wound site 9 days after scaffold application demonstrates no significant difference in fibrosis (A), granulotamous inflammation (B), subacute/chronic inflammation (C), or necrosis (D) between controls (n = 4) and SDF-1-treated wounds (n = 8). SDF-1 release kinetics from the scaffold for both the SDF-1 plasmid and the SDF-1 protein. Interestingly, the time course of the in vivo release kinetics differed between plasmid and protein; however, the SDF-1-induced wound-healing benefit was observed independent of the delivery modality. Several investigators have employed model proteins such as albumin and IgG to examine protein release from carriers. Some used recombinant proteins, but very few have shown in vivo release profiles. As shown in Figures 1 and 2, we found that the difference between the in vivo and in vitro profiles for both the SDF-1 protein and plasmid may be due to the displacement of the SDF-1 protein with other heparin-binding proteins or to the biological responses to the implanted vehicles. We did not check the stability of SDF-1 protein and plasmid, but rather the remaining radioactivity of radiolabeled SDF-1 protein and plasmid. Protein and plasmid can be cleaved by proteinases and DNases in the body, respectively. Thus, some mechanisms that allow SDF-1 protein and plasmid to exhibit their bioactivities by protecting them from enzymatic digestion should be considered to explain the accelerated wound healing observed after therapeutic application of SDF-1 protein and plasmid. It is well known that many growth factors are stored in the body by binding to extracellular matrices, such as heparin sulfate proteogly- cans and growth factor binding proteins, which protect the growth factors from enzymatic digestion and regulate certain in vivo biological activities. In regenerating tissues and organs, the binding of extracellular matrix proteins and proteoglycans to growth factors is mitigated by enzymes secreted by the healing tissue, leading to the release of growth factors in a biologically active form. It has been previously reported that the stability or resistance of growth factor proteins and plasmids against proteinases or DNases is increased in biodegradable gelatin hydrogels due to their binding with gelatin molecules (14,24). Based on this mechanism, we mimicked the naturally occurring release system for growth factor proteins or plasmids and extended their biological activity in vivo by controlling their release from gelatin hydrogels. As shown in Figure 2, we found that the alginate patches prolonged the in vivo retention of both SDF-1 protein and plasmid over 2 weeks. Because heparin and spermine introduced into the presented alginate scaffolds can bind to SDF-1 protein and plasmid, respectively, this result strongly suggests that SDF-1 protein and plasmid binds to patches and consequently achieves the prolonged in vivo retention in a biologically active form. As described above, the release of the plasmid was markedly slower compared to the protein in vivo (Fig. ALGINATE SCAFFOLDS AS DELIVERY VEHICLE FOR SDF-1 IN INJURY 1). However, both provided similar acceleration of the healing of surgical wounds (Figs. 2 and 3). There are a number of potential explanations. SDF-1’s wound-healing benefit may be relatively time independent, and delivery of SDF-1 within a certain number of days following wound creation is sufficient. In contrast to the kinetics of SDF-1 protein, which releases quickly in vivo, only 20% of SDF-1 plasmid is released 1 day following delivery and is likely not significantly expressed until at least 24 h after delivery, but 75% is released after 6 days (Fig. 1). Although the release characteristics differed, both SDF-1 protein and plasmid treatment accelerated wound healing (Fig. 2). A second explanation might be that SDF-1 must be delivered close to the time of wound creation. However, in this study an exceptionally high dose of SDF-1 was delivered, so that even 20% of total plasmid release/60% of protein release after 1 day is sufficient to provide benefit. This is supported by previous work demonstrating that the application of SDF-1 within 2 days postwounding is effective in accelerating the healing of diabetic wounds (11). Furthermore, under different experimental conditions, stem cell homing has been induced with lower concentrations of SDF-1 protein and plasmid than those used in this study (22,25). Histological analysis of the wound measured by PECAM-1 (CD31) on day 9 revealed that the SDF-1 release decreased vascularization of the wound. Similarly, smooth muscle α-actin staining confirms a lower level of remodeling. Staining of the PBS control group is shown for comparison (Fig. 4). The beneficial effect of SDF-1 on wound healing in this large-animal model (Figs. 2 and 3) is novel but consistent with recent reports identifying an important role for SDF-1 in wound healing. Not only has SDF-1 been shown to be preferentially expressed at the wound margin where healing occurs, two independent rodent studies show that administration of SDF-1 protein or lentivirus encoding SDF-1 improved wound healing in hard-to-heal diabetic wounds by increasing homing of endothelial progenitor cells (EPCs) to the wound site (5,6,11,23,26). The same mechanism has been implicated in patients with thermal wounds (i.e., burns) where, following injury, SDF-1 levels are increased proportionally to the extent of EPC mobilization (10). Finally, these findings in wound healing are supported by a large body of literature demonstrating that SDF-1 recruits progenitor cells, induces angiogenesis, and promotes healing when delivered to ischemically damaged cardiac, peripheral vascular, or renal tissue (2,18,28,30). One particularly clinically relevant finding in this study is that SDF-1-treated wounds that fully closed showed no scarring at the wound site (Fig. 3, vimentin 2× images in Fig. 4). Dermal wounds created during fe- 407 tal development heal without remnants of a scar (16,17). One of the important molecular pathways responsible for regulating fetal development in a number of organ systems is the sonic hedgehog–Gli pathway (9), which has been implicated in healing ischemic injury as well. Delivery of a sonic hedgehog (Shh) plasmid to cardiac ischemic tissue has improved cardiac function (9,13). In both this myocardial injury model and in wound-healing models, treatment with Shh has been shown to upregulate SDF-1 and SDF-1’s enhancement of EPC homing to the site of injury (1,13). Therefore, our data suggest that Shh-mediated SDF-1 upregulation may be the mechanism by which there is decreased scarring following fetal surgery. If correct, our data further suggest that SDF-1 overexpression in adult would healing may be a strategy to decrease scar formation in adulthood. Interestingly, our histology does not demonstrate a significant increase in vascular density in those animals that received SDF-1 protein or plasmid. This lack of angiogenesis suggests that the benefits associated with SDF1 treatment in our study may be a mechanism other than EPC homing. In conclusion, continuous delivery of the proangiogenic modulator, SDF-1 plasmid or protein, through an alginate scaffold significantly accelerates wound healing and may reduce scarring in a clinically relevant acute surgical wound model. ACKNOWLEDGMENTS: We thank Matthew Kiedrowski for plasmid production and Amanda Finan for scaffold loading. We thank MPI Research (Kalamazoo, MI) for the execution of this study. REFERENCES 1. Asai, J.; Takenaka, H.; Kusano, K. F.; Ii, M.; Luedemann, C.; Curry, C.; Eaton, E.; Iwakura, A.; Tsutsumi, Y.; Hamada, H.; Kishimoto, S.; Thorne, T.; Kishore, R.; Losordo, D. W. Topical sonic hedgehog gene therapy accelerates wound healing in diabetes by enhancing endothelial progenitor cell-mediated microvascular remodeling. Circulation 113(20):2413–2424; 2006. 2. Askari, A. T.; Unzek, S.; Popovic, Z. B.; Goldman, C. K.; Forudi, F.; Kiedrowski, M.; Rovner, A.; Ellis, S. G.; Thomas, J. D.; DiCorleto, P. E.; Topol, E. J.; Penn, M. S. Effect of stromal-cell-derived factor 1 on stem-cell homing and tissue regeneration in ischaemic cardiomyopathy. Lancet 362(9385):697–703; 2003. 3. Augst, A. D.; Kong, H. J.; Mooney, D. J. Alginate hydrogels as biomaterials. Macromol. Biosci. 6(8):623–633; 2006. 4. Avniel, S.; Arik, Z.; Maly, A.; Sagie, A.; Basst, H. B.; Yahana, M. D.; Weiss, I. D.; Pal, B.; Wald, O.; Ad-El, D.; Fujii, N.; Arenzana-Seisdedos, F.; Jung, S.; Galun, E.; Gur, E.; Peled, A. Involvement of the CXCL12/CXCR4 pathway in the recovery of skin following burns. J. Invest. Dermatol. 126(2):468–476; 2006. 5. Badillo, A. T.; Chung, S.; Zhang, L.; Zoltick, P.; Liechty, K. W. Lentiviral gene transfer of SDF-1alpha to wounds improves diabetic wound healing. J. Surg. Res. 143(1): 35–42; 2007. 408 6. Badillo, A. T.; Zhang, L.; Liechty, K. W. Stromal progenitor cells promote leukocyte migration through production of stromal-derived growth factor 1alpha: A potential mechanism for stromal progenitor cell-mediated enhancement of cellular recruitment to wounds. J. Pediatr. Surg. 43(6):1128–1133; 2008. 7. Deglurkar, I.; Mal, N.; Mills, W. R.; Popovic, Z. B.; McCarthy, P.; Blackstone, E. H.; Laurita, K. R.; Penn, M. S. Mechanical and electrical effects of cell-based gene therapy for ischemic cardiomyopathy are independent. Hum. Gene Ther. 17(11):1144–1151; 2006. 8. Dittrich, R.; Despang, F.; Bernhardt, A.; Mannschatz, A.; Hanke, Th.; Tomandl, G.; Pompe, W.; Gelinsky, M. Mineralized scaffolds for hard tissue engineering by ionotropic gelation of alginate. Adv. Sci. Technol. 49:159– 164; 2006. 9. Drossopoulou, G.; Lewis, K. E.; Sanz-Ezquerro, J. J.; Nikbakht, N.; McMahon, A. P.; Hofmann, C.; Tickle, C. A model for anteroposterior patterning of the vertebrate limb based on sequential long- and short-range Shh signaling and Bmp signaling. Development 127(7):1337– 1348; 2000. 10. Fox, A.; Smythe, J.; Fisher, N.; Tyler, M. P.; McGrouther, D. A.; Watt, S. M.; Harris, A. L. Mobilization of endothelial progenitor cells into the circulation in burned patients. Br. J. Surg. 95(2):244–251; 2008. 11. Gallagher, K. A.; Liu, Z. J.; Xiao, M.; Chen, H.; Goldstein, L. J.; Buerk, D. G.; Nedeau, A.; Thom, S. R.; Velazquez, O. C. Diabetic impairments in NO-mediated endothelial progenitor cell mobilization and homing are reversed by hyperoxia and SDF-1 alpha. J. Clin. Invest. 117(5):1249–1259; 2007. 12. Greenwood, F. C.; Hunter, W. M.; Glover, J. S. The preparation of I-131-labelled human growth hormone of high specific radioactivity. Biochem. J. 89:114–123; 1963. 13. Kusano, K. F.; Pola, R.; Murayama, T.; Curry, C.; Kawamoto, A.; Iwakura, A.; Shintani, S.; Li, M.; Asai, J.; Tkebuchava, T.; Thorne, T.; Takenaka, H.; Aikawa, R.; Goukassian, D.; von Samson, P.; Hamada, H.; Yoon, Y. S.; Silver, M.; Eaton, E.; Ma, H.; Heyd, L.; Kearney, M.; Munger, W.; Porter, J. A.; Kishore, R.; Losordo, D. W. Sonic hedgehog myocardial gene therapy: Tissue repair through transient reconstitution of embryonic signaling. Nat. Med. 11(11):1197–1204; 2005. 14. Kushibiki, T.; Tomoshige, R.; Iwanaga, K.; Kakemi, M.; Tabata, Y. In vitro transfection of plasmid DNA by cationized gelatin prepared from different amine compounds. J. Biomater. Sci. Polym. Ed. 17(6):645–658; 2006. 15. Lapidot, T.; Petit, I. Current understanding of stem cell mobilization: The roles of chemokines, proteolytic enzymes, adhesion molecules, cytokines, and stromal cells. Exp. Hematol. 30(9):973–981; 2002. 16. Longaker, M. T.; Whitby, D. J.; Adzick, N. S.; Crombleholme, T. M.; Langer, J. C.; Duncan, B. W.; Bradley, S. M.; Stern, R.; Ferguson, M. W.; Harrison, M. R. Studies in fetal wound healing, VI. Second and early third trimester fetal wounds demonstrate rapid collagen deposition without scar formation. J. Pediatr. Surg. 25(1):63–69; 1990. 17. Lorenz, H. P.; Whitby, D. J.; Longaker, M. T.; Adzick, N. S. Fetal wound healing. The ontogeny of scar formation in the non-human primate. Ann. Surg. 217(4):391– 396; 1993. 18. Lotan, D.; Sheinberg, N.; Kopolovic, J.; Dekel, B. Expres- RABBANY ET AL. 19. 20. 21. 22. 23. 24. 25. 26. 27. 28. 29. 30. sion of SDF-1/CXCR4 in injured human kidneys. Pediatr. Nephrol. 23(1):71–77; 2008. Michaels, J.; Churgin, S. S.; Blechman, K. M.; Greives, M. R.; Aarabi, S.; Galiano, R. D.; Gurtner, G. C. db/db mice exhibit severe wound-healing impairments compared with other murine diabetic strains in a silicone-splinted excisional wound model. Wound Repair Regen. 15(5): 665–670; 2007. Moulin, V. Growth factors in skin wound healing. Eur. J. Cell Biol. 68(1):1–7; 1995. Petit, I.; Szyper-Kravitz, M.; Nagler, A.; Lahav, M.; Peled, A.; Habler, L.; Ponomaryov, T.; Taichman, R. S.; Arenzana-Seisdedos, F.; Fujii, N.; Sandbank, J.; Zipori, D.; Lapidot, T. G-CSF induces stem cell mobilization by decreasing bone marrow SDF-1 and up-regulating CXCR4. Nat. Immunol. 3(7):687–694; 2002. Plett, P. A.; Frankovitz, S. M.; Wolber, F. M.; Abonour, R.; Orschell-Traycoff, C. M. Treatment of circulating CD34(+) cells with SDF-1alpha or anti-CXCR4 antibody enhances migration and NOD/SCID repopulating potential. Exp. Hematol. 30(9):1061–1069; 2002. Sasaki, T.; Fukazawa, R.; Ogawa, S.; Kanno, S.; Nitta, T.; Ochi, M.; Shimizu, K. Stromal cell-derived factor-1alpha improves infarcted heart function through angiogenesis in mice. Pediatr. Int. 49(6):966–971; 2007. Tabata, Y.; Ishii, T.; Muniruzzaman, M.; Hirano, Y.; Ikada, Y. Influence of gelatin complexation on cell proliferation activity and proteolytic resistance of basic fibroblast growth factor. J. Biomater. Sci. Polym. Ed. 11(6): 571–582; 2000. Tang, Y. L.; Qian, K.; Zhang, Y. C.; Shen, L.; Phillips, M. I. Mobilizing of haematopoietic stem cells to ischemic myocardium by plasmid mediated stromal-cell-derived factor-1alpha (SDF-1alpha) treatment. Regul. Pept. 125(1–3): 1–8; 2005. Toksoy, A.; Muller, V.; Gillitzer, R.; Goebeler, M. Biphasic expression of stromal cell-derived factor-1 during human wound healing. Br. J. Dermatol. 157(6):1148–1154; 2007. van Weel, V.; Seghers, L.; de Vries, M. R.; Kuiper, E. J.; Schlingemann, R. O.; Bajema, I. M.; Lindeman, J. H.; Delis-van Diemen, P. M.; van Hinsbergh, V. W.; van Bockel, J. H.; Quax, P. H. Expression of vascular endothelial growth factor, stromal cell-derived factor-1, and CXCR4 in human limb muscle with acute and chronic ischemia. Arterioscler. Thromb. Vasc. Biol. 27(6):1426– 1432; 2007. Yamaguchi, J.; Kusano, K. F.; Masuo, O.; Kawamoto, A.; Silver, M.; Murasawa, S.; Bosch-Marce, M.; Masuda, H.; Losordo, D. W.; Isner, J. M.; Asahara, T. Stromal cellderived factor-1 effects on ex vivo expanded endothelial progenitor cell recruitment for ischemic neovascularization. Circulation 107(9):1322–1328; 2003. Yano, T.; Liu, Z.; Donovan, J.; Thomas, M. K.; Habener, J. F. Stromal cell derived factor-1 (SDF-1)/CXCL12 attenuates diabetes in mice and promotes pancreatic beta-cell survival by activation of the prosurvival kinase Akt. Diabetes 56(12):2946–2957; 2007. Zhang, M.; Mal, N.; Kiedrowski, M.; Chacko, M.; Askari, A. T.; Popovic, Z. B.; Koc, O. N.; Penn, M. S. SDF-1 expression by mesenchymal stem cells results in trophic support of cardiac myocytes after myocardial infarction. FASEB J. 21(12):3197–3207; 2007.