3 1 2 6
advertisement

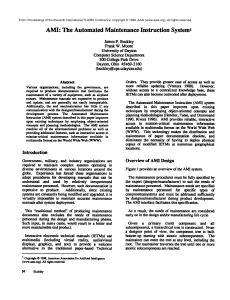
1 2 3 4 5 6 8 9 7 10 THE NURSING CARE STANDARDS FOR PATIENT FOOD IN HOSPITAL Body Mass Index (BMI) Your weight in kilos 40 50 60 70 80 90 100 110 120 130 140 150 1.98 6’5 1.96 6’4 1.94 6’3 1.92 UNDERWEIGHT 6’2 OK OVERWEIGHT OBESE © Crown Copyright 6’6 1.90 VERY OBESE 1.88 6’1 1.86 6’0 1.84 1.82 5’11 1.80 5’10 1.78 1.76 5’9 1.74 5’8 1.72 1.70 5’6 1.68 5’5 1.66 1.64 5’4 1.62 5’3 1.60 5’2 1.58 1.56 5’1 1.54 5’0 1.52 4’11 1.50 1.48 4’10 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 Your weight in stones Underweight – you may need to put on weight by eating more. OK – you are a healthy weight and should aim to stay that way. Overweight – you need to make sure that your weight does not continue to rise and try to lose some weight if you can. Obese or very obese – your health is at risk and you need to lose weight. Your height in metres Your height in feet and inches 5’7 Get your 10 a day! THE NURSING CARE STANDARDS FOR PATIENT FOOD IN HOSPITAL Acknowledgements Many people have contributed to Get your 10 a day! The Nursing Care Standards For The Patient Food In Hospital. These include patient representatives, all members of the multidisciplinary team as well as colleagues from Estates Services and catering. Thanks also to all of those who contributed to both the initial workshop (annex 1) and those who provided critical feedback during the consultation phase. A particular word of thanks to Pauline Mulholland, Nutrition and Diet Therapy Manager at the South Eastern Trust for her ongoing commitment and support, to Margaret O’Hagan, Nursing Officer, DHSSPS, for leading on this important piece of work and Dr Carolyn Mason, Head of Professional Development at the RCN for coordinating the entire effort. Foreword Adequate food and fluids are as essential to good care in hospital as the medicines patients are prescribed and the treatment they receive. Simply put, meeting patients’ nutritional requirements will help them return to health more quickly and prevent a whole range of complications which can delay recovery. Patients rightly expect that during their stay in hospital they will be provided with food that is both nutritious and appetising. As a result the quality of food and beverages are often cited as a benchmark by which patients and relatives judge the quality of care. When patients are ill, there is more risk of them not eating the right balance of nutrients which will help their recovery. The challenge for all healthcare workers is to encourage and support patients in meeting their nutritional needs. Responsibility for the delivery and presentation of meals and fluids should be clearly defined, and those patients who require help with eating or drinking clearly identified. In Get your 10 a day! The Nursing Care Standards for Patient Food in Hospital nurses and midwives have set out ways in which they can improve the nutritional care and food experience of patients in hospital. They have an important role to play in this fundamental area of treatment and care. This initiative is an important part of an overall strategic framework we are developing that will ensure that we can provide nutritional hospital food that supports the delivery of high quality health and social care. I am delighted that nurses and midwives have put food in hospital high on their agenda and are leading the way in improving patient care and the patient experience. MICHAEL MCGIMPSEY Minister for Health, Social Services and Public Safety Introduction Nutrition and the meal experience are of vital importance to the patient in hospital. Not only is food necessary for life and represents a basic human right, but it is also a source of great pleasure, with important social, cultural, and religious functions all of which need consideration within a hospital setting. However as recently highlighted by Age Concern in the Hungry to be Heard campaign we do not always get it right. Nurses and midwives in Northern Ireland are dedicated to providing the best possible treatment and care to their patients. As the health workers who have most direct contact with patients in hospital1, nurses and midwives have huge potential to improve the patient experience in relation to eating and drinking and nutritional care. This potential can be realised by focusing our efforts on improving all aspects of food, fluid and nutritional care and giving nurses2 the practical tools and support they require to make nutrition a priority in the area where they work. Get your 10 a day! The Nursing Care Standards for Patient Food in Hospital has been developed as a collaboration between the DHSSPS Directorate of Nursing and Midwifery and the Royal College of Nursing (RCN) as a Northern Ireland response to the RCN’s national Nutrition Now campaign. The nursing care standards outlined in Get your 10 a day! represent the views and experiences of a broad range of stakeholders and were informed by an extensive evidence-base of knowledge and best practice from throughout the United Kingdom. They are designed to provide a framework within which patients, relatives and carers can participate in shaping the way that food and drink is offered and taken, and to promote 1 The term hospital refers to all in-patient facilities in Health and Social Care Trusts across NI 2 Throughout this document the term Nurses refers both nurses and midwives within the hospital setting. multidisciplinary working with nurses, healthcare assistants, dieticians, catering staff and speech and language therapists and others working towards the common goal of improving the patient experience of food and mealtimes in hospitals. MARTIN BRADLEY Chief Nursing Officer Contents Background 3 The 10 Nursing Care Standards 7 Standard 1 9 Standard 2 13 Standard 3 17 Standard 4 21 Standard 5 25 Standard 6 29 Standard 7 33 Standard 8 37 Standard 9 41 Standard 10 45 What Now? 48 Annex 49 Annex 1 51 PAGE 1 Background The provision of food, fluids and nutritional care in hospital is a multifaceted area of service and is the responsibility of many members of the hospital team. This is a diverse team and includes clinical staff: doctors, nurses, midwives, dieticians, speech and language therapists, occupational therapists and those in support roles: catering, domestic, healthcare assistants and therapy assistants. For patients to get the best possible service and derive maximum benefit from food, all members of the team must work together and “do their bit” in partnership with the patient and their relatives/carers. The nursing service in hospital is 24/7 and as such nurses are the only group staff who have direct contact with the patient at every mealtime and at all times in between. Therefore, nurses play a pivotal role in nutritional care and the meal experience of patients. The nursing responsibility is broad ranging and includes screening, assessment, planning, monitoring, serving, practical help with eating and drinking and on occasion, preparation of food in the ward area. Nurses are accountable for their practice in all aspects of the provision of food, fluid and nutritional care and need to be able to demonstrate that service and care are delivered to the highest standard possible. It is for this reason that Get your 10 a day! The Nursing Care Standards for Patient Food in Hospital have been developed for use across all in-patient facilities in the health and social care Trusts across Northern Ireland. What is a standard? A standard is a level of quality against which performance can be measured. These standards have been written in simple language. They are concise, clear and measurable. Each standard has a standard statement, which explains the level of performance to be achieved. The rationale section provides the reasons why the standard is considered to be important and in the section headed criteria the context of the PAGE 3 standard is explained. Finally all the standards contain examples of how the standard can be demonstrated and monitored. The evidence base for Get your 10 a day! The Nursing Care Standards for Patient Food in Hospital was principally drawn from the following source documents: Age Concern (2006) Hungry to be Heard. The scandal of malnourished older people in hospital. Age Concern, London www.ageconcern.org.uk/AgeConcern/Documents/Hungry_to_be _Heard_August_2006.pdf Allison S. (1999). Hospital Food as Treatment: A Report by a Working Party of BAPEN [British Association for Parenteral and Enteral Nutrition], Maidenhead: BAPEN www.peng.org.uk/food-as-treat.html Kelly L, Tessier S, et al. (2000); Still Hungry in Hospital: Identifying Malnutrition in Acute Hospital Admissions. Quarterly Journal of Medicine 93 (2): 93-98. McWhirter J, Pennington C. Patients (1997); Go Hungry in British Hospitals: Malnutrition is common, unrecognised, and untreatable in hospital patients [Letter]. British Medical Journal 314, (7082): 752. RCN Nutrition Now Campaign: regular articles in Nursing Standard beginning with the campaign launch reported in the issue 18 April, 2007 volume 21 no.32, and subsequent weekly articles in the journal from 30 May, 2007 volume 21 no.38 to 17 October volume 22, no.6. Council of Europe Resolution (2003) Food and Nutritional Care in Hospitals How to Prevent Under-Nutrition: Report and Recommendations of the Committee ff Experts on Nutrition, Food Safety and Consumer Protection, Strasbourg: Council Of Europe Publishing. DoH (2003) Essence of Care – Patient Focused Benchmarks for Clinical Governance - Benchmarks for Food and Nutrition. SF Taylor &Co Ltd, Stockport Edington J, Boorman J, et al. (2000); Prevalence of malnutrition on admission to four hospitals in England. Clinical Nutrition 19 (3): 191-195. European Nutrition for Health Alliance (2005) Malnutrition within an Ageing Population: A Call to Action bmj.com/cgi/content/full/314/7082/752 PAGE 4 PAGE 5 The 10 nursing care standards for provision of patient food in hospital 1 1 4 41 17 47 4 7 7 2 2 5 25 8 2 8 5 10 5 10 8 8 10 1 1 1 1 9 5 9 5 5 9 5 6 9 6 6 6 7 who require nutritional intervention will have a nursing care plan 3 7 3 Patients implemented, evaluated and renewed to reflect the patient’s 7 3 devised, nutritional and physical care needs and which documents both the dietetic 3 plan7 and the nursing care assessment. 4 8 10 5 3 4 8 10 3 5 8 who require 10 food and/or fluid intake to be monitored will have 5 Patients 34 4 8 10out in a way that is informative, accurate and up-to-date. 3 5 that activity carried 3 3 6 36 399 6 6 9 9 10 III III III III 11 11 44 44 77 77 999 9 9 99 9 999 9 All patients admitted 9 to hospital are screened for risk of malnutrition. 9 99 999 999 99 9 9 999 9 9 9 99 9 9 9 9 999 9 9 9 by nurses, patients who are identified as malnourished 9 Following screening 999 9 9 999 9 or at risk of malnutrition are referred for and receive a nutritional 9 9 9 99 9 assessment appropriate to their level of need. III III III III III III III III IIII I IIII IIII IIIII IIIII IIIII IIII IIII 1 1 22 3333 22 55 6666 55 88 999 88 9 10 10 10 10 IIIIII IIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIIII IIIII IIIII IIII IIII III IIII III IIII III III III III III III III III II II III II III II 9 9 99 9 99 9 9 9 9999 99999999 who require support with eating and drinking are clearly identified. 99Patients 99 9 99 9 5 5 6 6 9 99 99 99999999 9 9999999 999 9 9 9 Patients who require support with eating and drinking receive assistance when it is required. Patients will be served their food and allowed to eat their meals without 3 99 99 7 7 3 disruption. 1 9 5 99 9 receive their meals in a physical environment that is conducive 45 8 Patients 10 3 10 5 34 8 to enjoying their food. 6 9 1 4 7 2 5 6 8 9 9 2 9 99 IIIIIIIIIIIIIII II II IIIIIIIIIIIIII I I I I I I I I I I I I I I II II II II II II II II II II I I I I I II II II II II I I I I II I I I I IIIIIIII IIIIIII IIIIIII III II II I IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIIIIII IIIII IIIII IIIIIIIIIIIIIIIIIIIIIIIIIIII IIII IIII IIIIII IIII II IIIII I I II II I I I I I I I I III I I IIII III II III III III I I II I I I III III III III II 31 3 4 5 6 7 8 9 10 9 I IIII IIIII I II II I I II II I III I 10 1 9 9 3 75 III III III IIII IIIII I IIIII 3 IIII IIII III III 9 99 9 9 99 9 9 whatever reason and can access snacks at ward level. 9 86 10 345 IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIIIII 99 9 9 9 Patients are offered a replacement meal if they miss their meal for 9 The patient receives food presented in a way that is appealing and appetising. II 7 PAGE 7 FACT Four out of 10 older people 1 admitted to hospital have malnutrition 4 on arrival. 7 STANDARD 2 3 5 6 8 9 10 1 All patients admitted to hospital are screened for risk of malnutrition 3 5 6 7 NT E M ES E G NA ELIN A M UID G STEP 5 ACUTE DISEASE EFFECT SCORE + WEIGHT LOSS SCORE BMI SCORE 2 3 STE P STEP OVERAL RISK OFL MALNUT RITION STEP 4 1 4 7 2 1 3 All patients admitted to hospital are screened for risk of malnutrition 5 8 10 6 Rationale Screening is a process of identifying patients who are already malnourished or who are at risk of becoming so. All patients, especially those who would be more vulnerable like older people, need to have their nutritional needs identified and met in order to advance their recovery and/or create optimum wellbeing, whatever their condition or level of dependence. 9 Criteria Incorporated in an organisational policy for food and nutrition will be guidelines which clearly identify the process for nutritional screening for all patients on admission to hospital. These guidelines are implemented and monitored within the context that: • All staff understand the fundamental importance of nutritional care and treatment of patients • All staff are fully aware of the screening policy and understand their role and responsibilities within it • A reliable and valid tool is used to screen patients on admission to hospital e.g. Malnutrition Universal Screening Tool (MUST) for adults • All staff that screen patients are trained in the use of the specific tool used in the Trust. 3 345 How this standard can be demonstrated and monitored • Documentation audit against all elements of the screening tool • Audit of staff training records • Benchmarking activity which includes action planning for improvement. II I III III III IIIII IIIIII IIIIIIIIIII STEP 1 PAGE 11 IIIIIIIIIIIIIIIIIIII IIIIII I 1 4 2 3 1 5 6 STANDARD FACT 9 7 Patients over the 8 age of 80 admitted to hospital have a 10 five times higher prevalence of malnutrition than those under the age of 50. 5 6 Following screening by nurses, patients who are identified as malnourished or at risk of malnutrition are referred for and receive a nutritional assessment appropriate to their level of need 3 345 III III III IIII IIII IIIIII IIIIIIIIIII IIIIIIIIIIIIIIIIIIII IIIIII IIIII IIII III III III 7 8 I 4 7 5 6 8 9 Following screening by nurses, patients who are 10 identified as malnourished or at risk of malnutrition are referred for and receive a nutritional assessment appropriate to their level of need 3 Rationale Patients who are malnourished or are at high risk of becoming malnourished will require referral for an in-depth nutritional assessment. Assessment is a more detailed process than screening, in which a range of specific methods can be used to identify and quantify impairment of nutritional status. Assessment is undertaken by registered practitioners who have received the necessary education and training and have been registered as competent to undertake the level of assessment required e.g. dietitian. 345 Criteria An organisational policy for food and nutrition will clearly identify the process for nutritional assessment for patients who are malnourished or at high risk of becoming malnourished patients in the hospital setting. The policy will be implemented and monitored within the context that: • All staff understand the fundamental importance of nutrition in the care and treatment of their patients • Patients are referred appropriately for dietetic assessment if required • A reliable and valid tool is used for assessment • The outcome of the assessment is available to the multidisciplinary team. I I III III III IIII IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII How this standard can be demonstrated and monitored • Documentation audit • Audit of dietetic referrals • Benchmarking activity which includes action planning for improvement. PAGE 15 IIIII I 5 6 8 9 4 7 10 FACT Six out of 10 older people are at risk of becoming malnourished. 6 STANDARD 7 3 Patients who require nutritional intervention will have a nursing care plan devised, implemented, evaluated and renewed to reflect the patient’s nutritional and physical care needs and which documents both the dietetic plan and the nursing care assessment. 345 III III III III III IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII IIII III III III 8 3 Patients who require nutritional intervention will have a nursing care plan devised, implemented, evaluated and renewed to reflect the patient’s nutritional and physical care needs and which documents both the dietetic plan and the nursing care assessment 345 IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII Rationale Patients who require nutritional assessment and subsequent intervention must have a nursing care plan devised, implemented and evaluated to document and communicate the nutritional care and treatment that is required by the patient. I III III II IIII IIIII IIIIII Criteria An organisational policy for food and nutrition will clearly identify documentation to support the planning, provision and evaluation of nursing care provided to patients requiring nutritional intervention. These guidelines are implemented and monitored within the context that: • All staff understand the fundamental importance of care planning • A registered nurse plans and evaluates the nursing care plan • The nursing care plan reflects the dietetic assessment and treatment plan • The patient’s clinical notes reflect the monitoring, decision-making and action/evaluation process with this aspect of nutritional care. How this standard can be demonstrated and monitored • Audit of nursing notes and/or care plan • Benchmarking activity which includes action planning for improvement. PAGE 19 IIIII 10 7 3 STANDARD FACT Patients who are malnourished stay in hospital for a longer time, require more medications, and are more likely to suffer from infections. 345 III III III III III IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII IIII III III III Patients who require food and/or fluid intake to be monitored will have that activity carried out in a way that is informative, accurate and up to date 8 345 II I III III III IIIII IIIIII IIIIIIIIIII Patients who require food and/or fluid intake to be monitored will have that activity carried out in a way that is informative, accurate and up to date Rationale The amount of food and fluid a patient consumes must be known as it is a vital indicator of effective care and treatment. Criteria An organisational policy for food and nutrition will clearly reflect need for recording and monitoring food and fluid intake. The policy will be implemented and monitored within the context that: • All staff understand the fundamental importance of recording and monitoring food and fluid intake, and the requirement to take action when there is cause for concern • Registered nurses take individual responsibility for ensuring that patient’s fluid and food intake is monitored and recorded where applicable • The record is available to the multidisciplinary team • There are clear indicators of when action should be taken, what action and by whom. How this standard can be demonstrated and monitored • Observational audit • Documentation audit e.g. audit of fluid balance and food record charts • Benchmarking activity which includes action planning for improvement. PAGE 23 IIIIIIIIIIIIIIIIIIII IIIIII IIII STANDARD 9 9 9 9 9 FACT 3 1 It is2estimated that 30 - 50% of food 6 4 hospital 5is wasted. 7 8 1 5 Patients who require support with eating and drinking are clearly identified 6 9 10 3 7 99 9 9 9 9 9 9 9 9 9 1 4 7 2 5 8 10 1 3 6 9 5 Patients who require support with eating and drinking are clearly identified 6 Rationale Many staff, some of whom may not be aware of an individual’s needs, interact with patients before, during and after meal times. Therefore there is a requirement for a way in which patients that require assistance/support with eating and drinking are easily identifed. Criteria Highlighted in the organisational policy for food and nutrition will be a Trust–wide approach to identifying patients that require support with eating and drinking. The policy will be implemented and monitored within the context that: • The Trust adopts a clear system of identifying patients who require additional help with eating and drinking e.g. coloured napkin/coloured tray • All staff are aware of the system in place to identify patients who require support • Registered nurses take individual responsibility for ensuring patients who need help are identified • People (including relatives) with appropriate training are available to assist patients with eating and drinking when required. 7 3 345 8 How this standard can be demonstrated and monitored • Observational audits • Documentation audits • Benchmarking activity which includes action planning for improvement • User satisfaction surveys • Evaluation of stories from service users. III III III III IIIII IIIII IIIIIIIII IIIIIIIIIIIIIIIIIIIIIIII IIIIII IIII IIII III III III I PAGE 27 9 9 9 9 9 1 3 FACT 2The toll of on 6 4 malnutrition 5 and health health care costs is 9 7 8 estimated to exceed £7.3 billion 10year (much per more than obesity). Over half of this cost is expended on people aged 65 years and above. 1 5 STANDARD 99 9 9 9 9 9 9 9 9 9 6 All patients who require support with eating and drinking receive assistance when it is required 7 3 345 III III II III IIII IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII IIII III III III 8 10 4 7 5 8 10 6 9 All patients who require support with eating and drinking receive assistance when it is required Rationale Patients may need assistance both prior to and when eating and drinking. This may involve hand hygiene, positioning of the person in preparation for mealtimes, oral hygiene or actual ‘hands on’ assistance, as well as specific equipment such as modified crockery, utensils etc. 7 3 when help is needed! Criteria An organisational policy for food and nutrition will clearly address providing assistance to patients who require additional support with eating and drinking. The policy will be implemented and monitored within the context that: • Registered nurses take individual responsibility for ensuring assistance/support for patients with eating and drinking is provided • People are available to assist patients with eating and drinking when it is required • People assisting patients with eating and drinking will have received training to do so • Patients’ dignity is never compromised • Modified utensils and equipment, including furniture, are available and used appropriately • Independence is promoted. 345 III III III IIII IIII IIIIII IIIIIIIIIII IIIIIIIIIIIIIIIIIIII IIIIII IIIII IIII III III III 8 I How this standard can be demonstrated and monitored • Observational audits • Benchmarking activity which includes action planning for improvement • User satisfaction surveys • Evaluation of stories from service users. PAGE 31 1 4 7 1 2 5 6 8 9 5 99 9 9 9 9 9 9 9 6 10 STANDARD “Nothing shall be done on a ward whilst patients are having their meals” 7 3 Patients will be served their food and allowed to eat their meals without disruption Florence Nightingale in 1859 345 III III III IIII IIII IIIIII IIIIIIIIIII IIIIIIIIIIIIIIIIIIII IIIIII IIIII IIII III III III 8 I 10 7 3 Patients will be served their food and allowed to eat their meals without disruption Rationale Nurses can improve the nutritional care and status of patients by creating a protected environment that allows patients to eat their meals without disruption. 345 8 Criteria Integral to an organisational policy for food and nutrition will be a protected mealtime policy for local implementation. This policy will be implemented and monitored within the context that: • All staff are aware of and adhere to the protected mealtime policy • Non-urgent activities such as cleaning, non-priority treatments, ward rounds, visiting etc. are designed to be operated around and outside of pre-set meal times • Staff and visitors respect the patients’ mealtimes as a time focused on the patient. III III III III III IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII IIII III III III How this standard can be demonstrated and monitored • Multi-professional observational audits • Benchmarking activity which includes action planning for improvement • User satisfaction surveys • Evaluation of stories from service users • Review and monitor lessons learned from complaints. PAGE 35 10 7 3 FACT Of 500 patients admitted to an acute hospital in the UK, 40% were undernourished on admission and 75% by the time of discharge! STANDARD 345 III III II IIII IIIII IIIII IIIIIIIIII IIIIIIIIIIIIIIIIIIIIIII IIIIII IIII IIII III III III 8 I Patients receive their meals in a physical environment that is conducive to enjoying their food 10 345 III III III III III IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII IIII III III 8 III Patients receive their meals in a physical environment that is conducive to enjoying their food Rationale The hospital ward environment, i.e. sights, sounds and smells, and preparedness to eat can have an impact on the individual’s desire and ability to eat and enjoy their food. Criteria Incorporated in an organisational policy for food and nutrition will be an emphasis on process to ensure the ward environment and preparedness of the patient is conducive to eating and drinking. The policy will be implemented and monitored within the context that: • Consideration is given to tables, seating, utensils, adapted utensils and washing/hygiene facilities • Steps are taken to ensure the ward environment is conducive to eating and drinking. How this standard can be demonstrated and monitored • Observational audits • Benchmarking activity which includes action planning for improvement • User satisfaction surveys • Evaluation of stories from service users • Review and monitor lessons learned from complaints. PAGE 39 STANDARD 9 9 9 9 9 “Thousands of patients are 3 2 annually starved in the midst of plenty 6 5 from want of attention to the 9 8 ways which make it possible for them 10 to take food” 1 5 6 Florence Nightingale in 1859 3 7 99 9 9 9 9 9 9 9 9 Patients are 9 offered a replacement meal if they miss their meal for whatever reason and can access snacks at ward level 9 9 9 9 9 1 4 7 2 5 8 1 3 5 99 9 9 9 9 9 9 Patients are offered a replacement meal if they miss their meal for whatever reason and can access snacks at ward level 6 9 9 9 6 Rationale Good nutrition is a cornerstone of effective care and treatment. Access to food and drinks should match the needs of patients and not be constrained by ward or service delivery routines. 9 Criteria Incorporated in an organisational policy for food and nutrition will be protocols regarding the provision of food available outside set meal times. These protocols are implemented and monitored within the context that: • Registered nurses take individual responsibility for ensuring that patients who miss a meal receive a replacement meal or alternative food and beverage • Individual patients are given choice to meet personal preferences • Food and beverage should be appropriate in respect of religious and cultural factors, age related and special needs • Food and beverage is served at the correct temperature for patient preference and meets safety standards at all times • All staff serving food will receive appropriate training to do so • Suitable crockery and utensils are available at ward level • Hot food and snacks are made available outside set mealtimes. 10 7 3 345 III III III IIII IIII IIIIII IIIIIIIIIII 8 How this standard can be demonstrated and monitored • Observational audits • Audit of staff training records • Benchmarking activity which includes action planning for improvement • User satisfaction surveys • Evaluation of stories from service users. IIIIIIIIIIIIIIIIIIII IIIIII IIIII IIII III III III 10 I PAGE 43 10 7 3 FACT Only 18% of patients are satisfied with the overall quality of food served. STANDARD 345 III III II III IIII IIIII IIIIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII IIII III III 8 10 III The patient receives food presented in a way that is appealing and appetising 345 III III III I IIII IIII IIIIII IIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII IIIII IIII III III III 8 10 II The patient receives food presented in a way that is appealing and appetising. Rationale To meet their nutritional needs, patients should have food presented in a way that takes account of what appeals to them as an individual. Food should be tastefully presented and appealing to patients. Criteria Incorporated in an organisational policy for food and nutrition will be an emphasis on the importance of food presentation. The policy will be implemented and monitored within the context that: • All food, regardless of who prepares it or serves it, should be presented to the patient in an appealing way • Food and drink is served at the correct temperature for patient preference and meets safety standards at all times • All staff preparing and serving food will receive appropriate training to do so. How this standard can be demonstrated and monitored • Observational audits • Audit of staff training records • Benchmarking activity which includes action planning for improvement • User satisfaction surveys • Evaluation of stories from service users • Review and monitor lessons learned from complaints. PAGE 47 What Now? Nurses have a real opportunity to improve the nutritional care and meal experience of patients. This document has been specifically designed so that the perforated pages can be used as posters in the ward area to help get the message across that nurses are serious about improving patient care and experience in the area of food and nutrition in hospital. This document will be distributed widely and the Directors of Nursing in the Health & Social Care Trusts will be responsible for implementing the standards and monitoring nursing performance in this area. Progress of this will be kept under review by the Chief Nursing Officer. PAGE 48 Annex Hospital Food Annex 1 The top picture is an example of food patients receive in hospital. The picture below is the same food pureed and moulded and is presented in such a way as to resemble the pre-pureed meal. Participants at Food Standards Workshop Royal College of Nursing Northern Ireland 21 June 2007 NAME ORGANISATION Paddie Blaney NIPEC Ward Sisters will make sure that everyone knows the George Boal South Eastern HSCT importance of their own actions in controlling healthcare June Cairns South Eastern HSCT acquired infections. They will make cleanliness standards Jacqueline‘live’, Clarke Southern HSCT recognising achievements and saying thank you when Pauline Croskery Easternpoor HSCT things are done well, while alsoSouth challenging practice. Changing attitudes will mean developing pride in what Stella Cunningham Southern HSSC people think of as ‘our’ ward environment, Teresa Cushley Belfast HSCTand adopting a ‘clean up as you go’ approach Belfast to work.HSCT Karen Davidson Moira Davren Royal College of Nursing Governance arrangements within the Trust should support Joanne Deery Northern HSCT cultural change by establishing robust accountability Rosie Farrell Belfastand HSCT arrangements. Systems of reporting lines of Anne Harris Southern HSCT communication need to be clear. The commitment to Michelle Hunt Belfast HSCT cleanliness is long term and induction, ongoing training, Liz Konya audit and dealing positively with Northern HSCTare examples of complaints actions that will strengthen theRoyal driveCollege to improve the safety, Carolyn Mason of Nursing orderliness and appearance of hospital wards. Angela McErlane Northern HSCT Ashleagh Millar Belfast HSCT Allison Mowbray South Eastern HSCT Useful Information Edith Neale The 2004 Controls Assurance Northern Standard HSCT on Infection Control Adele Nichol South Eastern HSCTas part of provides a clear framework for control of infection Suzanne O’Boyle Belfast HSCT the standard governance requirements of the HPSS. Margaret Governance O’Hagan DHSSPS in HPSS, Controls Assurance Standards, Anne Marie Scally Control, DHSSPS 2004 South Infection can Eastern be foundHSCT at Barbara Soye Southern HSCT www.dhsspsni.gov.uk/hss/governance/assurance_standards Richard Walker South Eastern HSCT .asp Fiona Watters Belfast HSCT Linda Wray Belfast HSCT PAGE 50 PAGE 51 Notes PAGE 52 Forbidden foods by religious group Muslims: Pork, non-halal meat and chicken, shellfish, alcohol Hindu: Beef, sometimes lamb and chicken, oily fish, sometimes white fish, eggs, alcohol Sikh: Beef, sometimes all meat and fish, alcohol Buddhist: Chicken, lamb, pork, beef, shellfish (sometimes all fish), alcohol Rastafarian: Animal products (except milk), foods that are not Ital (Ital food is organic, not tinned or processed), added salt, alcohol, tea, coffee Jewish: Pork, any meat that has not been koshered, fish without scales and fins, shellfish. Meat and milk products served at the same meal or cooked together. Produced by: Department of Health, Social Services & Public Safety Castle Buildings, Stormont, Belfast BT4 3SQ Telephone: 028 9052 2593 Textphone: 028 9052 7668 www.dhsspsni.gov.uk November 2007