Date: From: Subject: November 12, 2007
advertisement

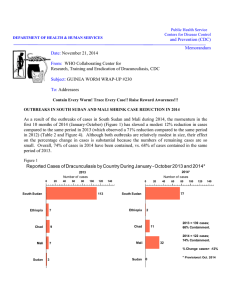
Public Health Service Centers for Disease Control and Prevention (CDC) Memorandum DEPARTMENT OF HEALTH & HUMAN SERVICES Date: November 12, 2007 From: WHO Collaborating Center for Research, Training and Eradication of Dracunculiasis Subject: GUINEA WORM WRAP-UP #177 To: Addressees “GUINEA WORM ANYWHERE IS GUINEA WORM EVERYWHERE” Alhaji Dr. Mohammed Bin Ibrahim, Regional Director of Health Services, Brong Ahafo Region, Ghana ETHIOPIA & COTE D’IVOIRE STOP GWD, BEGIN PRE-CERTIFICATION!! After months of suspense, there is increasing evidence and confidence that both Ethiopia and Cote d’Ivoire have interrupted indigenous transmission of dracunculiasis (Guinea worm disease). As of end October 2007, Ethiopia had reported no indigenous cases for 16 consecutive months and Cote d’Ivoire for 13 consecutive months (Figure 1). Thus thirteen of the original twenty endemic countries are now free of indigenous dracunculiasis, (Figure 2) and it is possible that Burkina Faso and Togo, with 11 and 10 consecutive zero case months respectively, may also have already recorded their last cases of Guinea worm disease. The 348 cases reported from all endemic countries during September 2007 (Table 1, Figure 4) represents the lowest number of cases of dracunculiasis reported during any month since the global program began. Figure 1 Number of Consecutive Months with Zero Indigenous Cases of Dracunculiasis: Jan. - Oct. 2007* Number of Months 0 5 10 15 Ethiopia 16 13 Cote d'Ivoire Burkina Faso Togo 20 11 10 * Provisional The national Guinea Worm Eradication Programs of Cote d’Ivoire and Ethiopia both had to work hard to stop transmission of dracunculiasis despite significant insecurity in their most recent endemic areas: ethnic clashes in parts of Gambella Region, Ethiopia, and civil war in Cote d’Ivoire. Fortunately, in Cote d’Ivoire, a strong push by MAP International, UNICEF, Health and Development International and The Carter Center to intensify interventions in the remaining endemic area just months before the civil war erupted in September 2002 helped prevent a potentially disastrous setback. By focusing its efforts to repair existing hand pumps, drill and equip new borehole wells, and help villagers construct bio-sand filters using local materials in the endemic districts of M’bahiakro, Tanda, Bondoukou and Bouna, MAP International helped improve access to safe water and reduce the rate of broken hand pumps in endemic and at-risk villages from 72% to 15%. Both bio-sand filters and hand pump sources were used in Dodoassue’ village (Tanda District), which reported 80% of all cases in the country in 2001, because the local population continued to use water from the river due to their strong relationship with the spirit of the river. Lendoukro village in M’bahiakro District recorded all 5 of Cote d’Ivoire’s final indigenous cases in 2006. Earlier uncertainty about whether Ethiopia had eliminated indigenous transmission derived from questions about the provenance of 3 cases recorded along Ethiopia’s border with southern Sudan, which is still highly endemic (see Guinea Worm Wrap-Up #175). Cote d’Ivoire hosted a WHO-sponsored meeting of Francophone countries (Benin, Chad, Cote d’Ivoire, Mauritania, Guinea) in the pre-certification phase of dracunculiasis eradication at Abidjan on September 4-5, 2007. Ethiopia hosted a WHO-sponsored meeting for Anglophone countries and areas (Ethiopia, Kenya, northern Sudan, Uganda) in the precertification phase at Addis Ababa on October 30-31, 2007. Figure 2 Distribution by Country of 9,589 Indigenous Cases of Dracunculiasis Reported during 2007* Number of cases 0 1,000 2,000 3,000 4,000 Niger (10) 7,000 3,218 223 Mali (10) Burkina Faso (10) 6,000 6,094 Sudan (9) Ghana (10) Nigeria (10) 5,000 43 11 0 Togo (10) 0 Cote d'Ivoire (10) 0 2006^ 0 2006^ Ethiopia (10) Benin 0 2004^ Mauritania 0 2004^ Uganda 0 2003^ Cent. African Rep. 0 2001^ Chad 0 1998^ Cameroon 0 1997^ * Provisional. Numbers in parentheses indicate months for which reports have been received, e.g., (10) = January - October. excludes 14 cases exported from one country to another. ^ Year last indigenous case reported. Yemen 0 1997^ Senegal 0 1997^ India 0 1996^ Kenya 0 1994^ Pakistan 0 1993^ Pakistan and India were certified free of the disease in 1996 and 2000, respectively. Senegal and Yemen were certified free of the disease in 2004, and Cameroon and Central African Republic in 2007. NIGER REDUCES CASES BY -87%, ESTABLISHES NATIONAL CERTIFICATION COMMITTEE On October 5, Niger’s Minister of Public Health, Mr. Issa LAMINE, issued a decree establishing the National Commission for Certification of Dracunculiasis Eradication in Niger (Commission Nationale de la Certification de l’Eradication de la Dracunculose au Niger-CNCED). The commission will help mobilize resources, strengthen activities of the national Guinea Worm Eradication Program (GWEP), and submit reports to the International Commission for the Certification of Dracunculiasis Eradication (ICCDE). Commission members include the head of the department of public health in the Faculty of Health Sciences at Abdou Moumouni Dioffo University of Niamey (president), the director general in the ministry of public health (vice-president), the national coordinator of the GWEP, as well as five other members of the government, plus local representatives of WHO, UNICEF, and The Carter Center. This welcome step comes as Niger has recorded only 12 cases of Dracunculiasis in January-October 2007 (11 contained)(Table 1), including one imported case, compared to 91 cases during the same period of 2006, a reduction of –87% (Figures 3 and 5). The Niger GWEP also held a Worm Week in Niger’s last remaining endemic region (Tillaberi) on October 24-30. Table 1 Number of Cases Contained and Number Reported by Month during 2007* (Countries arranged in descending order of cases in 2006) COUNTRIES REPORTING CASES NUMBER OF CASES CONTAINED / NUMBER OF CASES REPORTED % JANUARY 38 SUDAN 812 GHANA 0 MALI 3 NIGER 7 NIGERIA 0 TOGO 2 BURKINA FASO 0 COTE D'IVOIRE 0 ETHIOPIA 0 UGANDA 862 TOTAL* / / / / / / / / / / / FEBRUARY 49 161 631 1005 0 0 0 3 9 32 1 0 0 2 0 0 0 0 0 0 690 1203 / / / / / / / / / / / MARCH 102 190 442 732 1 0 0 0 1 9 0 1 0 0 0 0 0 0 1 0 547 932 / / / / / / / / / / / APRIL 304 271 248 478 0 1 0 0 0 1 0 0 0 0 0 0 0 0 0 1 552 752 / / / 586 233 293 0 0 1 / / / / / / / / MAY 673 0 0 0 0 1 0 0 0 0 0 0 1 0 908 880 / / / 1339 185 272 1 0 0 / / / / / / / / JUNE 661 1 0 0 0 0 0 0 0 0 3 0 0 1 850 1613 / / / / / / / / 1473 91 241 5 1 1 0 0 0 0 0 0 0 0 0 0 / / / JULY 497 3 0 0 594 1718 / / / / / / / / / / / AUGUST 348 1206 38 111 29 7 0 1 0 0 0 0 0 0 0 0 0 0 1 0 416 1325 / / / / / 158 612 15 41 35 120 2 0 0 0 0 / / / 0 0 0 0 0 0 / / / SEPTEMBER 0 0 1 210 774 / / / / / / / / / / / OCTOBER / 258 / 19 15 68 4 3 0 0 0 0 0 0 0 0 0 0 0 0 19 348 NOVEMBER / 27 / / / / / / / / / DECEMBER 26 4 1 0 0 0 0 0 0 58 / / / / / / / / / / / / / / / / / / / / 0 0 / TOTAL* 2830 2695 86 11 17 1 2 0 3 3 5648 0 / / / / / / / / / / / 6096 46 3219 84 223 39 12 92 43 40 2 50 2 100 0 0 3 0 3 100 9603 59 % CONTAINED 72 74 73 63 56 49 45 54 60 33 #DIV/0! #DIV/0! 59 % CONT. OUTSIDE SUDAN 79 86 93 84 86 77 82 42 58 33 #DIV/0! #DIV/0! 80 * provisional Shaded cells denote months when zero indigenous cases were reported. Numbers indicate how many imported cases were reported and contained that month. CONT. #DIV/0! #DIV/0! Figure 3 Number of Indigenous Cases Reported During the Specified Period in 2006 and 2007*, and Percent Change in Cases Reported Country Indigenous Cases Reported 2006 Togo (10) % CHANGE 2006 - 2007 2007 -100% 15 0 -100% Cote d'Ivoire (10) 5 0 -100% Ethiopia (10) 1 0 -100% Burkina Faso (10) 1 0 -100% Niger (10) 90 11 Sudan (9) 18508 6094 275 223 Ghana (10) 3115 3218 Nigeria (10) 15 43 22025 9589 402 277 Mali (10) -50% 0% 50% 100% -88% -67% -19% 3% 180% Total All countries, excluding Sudan and Ghana Overall % change outside of Sudan = 1% (10) Indicates months for which reports were received, i.e., Jan. -Oct. * Provisional -56% -31% 129 Figure 4 Total Number of Dracunculiasis Cases Reported by Month, January 2000 - September 2007* 12000 Number of Cases 10000 8000 6000 4000 2000 0 Jan 00 Jul 00 Jan 01 Jul 01 Jan 02 Jul 02 Jan 03 Jul 03 Jan 04 Jul 04 Jan 05 Jul 05 Jan 06 Jul 06 Jan 07 Jul 07 Months * September 2007 recorded the few est monthly total of cases since the global GWEP began. Jan 08 Figure 5 NUMBER OF REPORTED CASES OF DRACUNCULIASIS: 2006 AND 2007* GHANA SUDAN 2006 = 20,582 cases 1,200 2006 -= 4,132 cases 2007* = 6,096 cases 5,000 2007* = 3,219 4,367 1,000 1,003 4,000 3,734 3,349 732 621 600 609 606 433 478 400 412 403 Number of cases Number of cases 800 63% Reporting rate: 3,137endemic villages 3,000 2,613 2,214 337 1,339 293 293 272 200 241 162 0 Feb Mar Apr May Jun 1,473 1,252 1,206 1,000 111 Jan 2,141 2,000 Jul 144 41 39 19 25 Aug Sept Oct 612 586 77 0 Nov Dec 161 1 190 12 271 77 Jan Feb Mar 64% Reporting rate: 3,776 endemic villages Apr May Jun 608 258 Jul Aug Sept 214 Oct Nov * Provisional Dec *provisional MALI NIGER 140 25 2006 = 329 cases 2007* = 223 cases 120 120 2006 = 110 cases 2007* = 12 cases 21 21 20 20 100 17 91 15 Number of cases Number of cases 81 80 72 68 60 12 10 41 7 40 6 26 5 20 14 8 7 0 3 0 1 0 01 1 0 3 0 1 Jan Feb Mar Apr May Jun 4 3 2 14 Aug Sept Oct Nov Dec * Provisional 2 2 1 0 Jul 3 Jan 0 0 0 Feb Mar Apr 1 0 May Jun 0 Jul Aug Sept Oct Nov Dec * Provisional GHANA REPORTS SIXTH CONSECUTIVE MONTH OF FEWER CASES Ghana has reported a total of 27 cases in October, for a cumulative total of 3,219 cases(Table 1, Figures 2 and 5), of which 84% were reportedly contained, so far in 2007. This is an increase of 3% in cases from the same period of 2006 (Figure 3). The monthly rate of reduction in cases has increased from –27% in April to –81% in October. The number of cases reported in September and October 2007 are the lowest ever reported for those months since the program began. Outside of Savelugu-Nanton District, Ghana’s other remaining endemic districts have reduced cases by –52% in January-September 2007. Intervention indices as of September 2007 were: 98% of endemic villages with health education, 84% with cloth filters in all households, 55% of endemic villages received pipe filters since January 2006, 47% had at least one safe source of drinking water, and 6% of endemic villages treated with ABATE® Larvicide in September. Five regions of Ghana are free of endemic transmission of dracunculiasis, three reported less than 100 cases, and two more than 100 cases in 2006 (Table 2). National coordinator Dr. Andrew Seidu-Korkor briefed key majority and minority parliamentary committee members on the status of Ghana’s GWEP on October 27. Table 2 Ghana Guinea Worm Eradication Program Years with no indigenous cases and remaining indigenous cases in 2006, by region Year Greater Accra Upper East Western X X 1995 1996 X X 1997 X X 1998 X X X 1999 X 2000 X X X 2001 X X X 2002 X X X X X 2003 2004 X X X 2005 X X X 2006 X X X X = zero indegenous cases reported Central Eastern Ashanti Upper West Volta Brong Ahafo Northern 66 84 204 3679 X X X X X X X X X X 31 MALI: INSECURITY IMPEDES OUTBREAK CONTROL IN KIDAL Mali has reported 223 cases of dracunculiasis, 86 (39%) of them contained, in 47 villages in JanuaryOctober 2007 (Figure 5). This is a decrease of -19% from the 275 cases reported during the same period of 2006. 86 of this year’s cases are from two villages experiencing the recent outbreak imported in Kidal Region from Gao Region (Figure 6). None of the cases of GWD confirmed in Kidal were contained. After the initial visit to this remote area by GWEP staff, insecurity ensued in Kidal and it has precluded the GWEP from implementing additional interventions. Four of Mali’s eight regions (Kayes, Koulikoro, Segou, Sikasso) have eliminated dracunculiasis. Case containment rates so far this year for the other three endemic regions outside Kidal range from 60% (67/112) in Gao; 67% (8/12) in Timbuktu; to 85% (11/13) in Mopti. Mali Guinea Worm Eradication Program Area of Interest Algeria Tessalit Town Mali ABEIBARA TESSALIT KIDAL Outbreak 5 TOMBOUCTOU TIN-ESSAKO KIDAL REGION Cercle / District Kidal Town Cases 2007 BOUREM 1-2 3-5 GOUNDAM 6-9 10 - 40 40+ MENAKA GAO DIRE GOURMA-RHAROUS TOMBOUCTOU NIAFUNKE GAO Gao Town ANSONGO YOUVAROU MOPTI ! ( TENENKOU DOUENTZA MOPTI BANDIAGARA Burkina Faso KORO 0 25 50 Niger 100 150 Kilometers 200 This map is provisional and is not an authority on boundaries or roads or exact locations. This map was created for the purpose of the Guinea Worm Eradication Program. WHO & CARTER CENTER REVIEW NIGERIAN ACTIVITIES From September 17-28, 2007, a team from the World Health Organization visited 16 states, 32 Local Government Areas (LGAs), 48 villages, and 353 households as part of a review of Guinea worm surveillance, management and supervision in Nigeria. As reported by Dr. Cephas Ityonzughul of WHO’s Nigeria office, the team concluded that although field activities have improved since the previous external evaluation in June 2004, there was still insufficient training, motivation, and transportation for field staff and village volunteers, lack of written guidelines for pre-certification, inadequate integration of surveillance for dracunculiasis into the Integrated Disease Surveillance and Reporting (IDSR) system, and inadequate funding for program activities by government at all levels. The overall monthly reporting rates for 696 recently endemic villages in 88 LGAs and 17 states (including 12 still officially endemic villages which have reporting rates of 100%), were 30%, 37%, 34%, 34%, 52%, 56%, 49%, and 39% for the first eight months of 2007. On October 22-24, The Carter Center held a Program Review for all Carter Centerassisted health programs in Nigeria, at the Sheraton Hotel in Abuja. The Opening Ceremony, which was chaired by former Nigerian Head of State General (Dr) Yakubu Gowon, included a passionate “farewell” address by the outgoing ambassador of Japan to Nigeria. Participants at the Review, which covered activities related to dracunculiasis eradication, lymphatic filariasis elimination, and control of schistosomiasis, onchocerciasis and trachoma, included representatives of WHO, UNICEF, CDC, the Bill & Melinda Gates Foundation, the Yakubu Gowon Center, the Nigerian Federal Ministry of Health and several state ministries of health, as well as The Carter Center. The new national coordinator of Nigeria’s GWEP, Mrs. Ifeoma Anagbogu, summarized the current state of the national program. ASSESSMENT OF POSSIBLE LOCAL TRANSMISSION IN TURKANA NORTH DISTRICT, KENYA, ON THE BORDER WITH SUDAN AND ETHIOPIA A team comprised of 8 officials, 3 from WHO and 5 from the Kenyan Ministry of Health visited Turkana North District from 11 to 15 October, in particular Kibbish area, 5km from the Ethiopian border in the northwest and 60km from the Sudanese border in the northeast. The mission was led by Michelle Gayer, Medical Officer, Disease Control in Humanitarian Emergency in Geneva and Dr. Eric Muchiri, Programme manager, Division of Vector Borne Diseases, Ministry of Health in Kenya. There is frequent cross-border movement between the three countries, thereby maintaining a risk of cross border transmission of Guinea Worm. The team surveyed the area to investigate rumors of active guinea worm cases. The team concluded that it is unlikely the indigenous transmission of Guinea Worm is occurring or has occurred in that part of Kenya for the last 12 years. Given the nomadic populations and cross border movements, the water situation, the poor surveillance system and lack of knowledge on GW disease prevention among the community, there is a risk of reintroduction of this disease into Kenya from Sudan. Kenya could thus be certified as a GW free country; however, adequate measures must be put into place by June 2008 to achieve certification after which it can apply to the International Certification Committee for Guinea Worm Eradication. IN BRIEF: Burkina Faso has appointed another new coordinator for the national Guinea Worm Eradication Program, following the departure of his recent predecessor for study abroad. He is Dr. Laurent NIKIEMA, previously of the Dedougou Sanitary District. Welcome, Dr. Nikiema, and may you have no cases to report during your service! Table 3 Reported Importations and Exportations of Cases of Dracunculiasis: 2007* From To Ghana Burkina Faso Jan. 2 Togo Sudan Feb. Mar. 1 Apr. Month and number of cases imported May June July Aug. Sept Dec. 1 3 1 1 Mali Niger 2 1 4 2 1 1 Number of caes exported 4 1 3 0 1 6 3 1 Togo Ghana Total 2 2 3 Uganda Total Nov. 1 Ethiopia Ethiopia Sudan Oct. 1 0 0 0 1 1 2 2 1 1 14 * Provisional MEETINGS Executive Board of the World Health Organization, week of January 21, 2008; Geneva (Guinea worm eradication to be discussed). Program Review for Southern Sudan GWEP January 30-31, 2008, Juba. African Regional Conference on Dracunculiasis Eradication, April 2-4, 2008. World Health Assembly, week of May 19, 2008; Geneva. (to receive report on Guinea worm eradication). SCHEDULE FOR LAST GUINEA WORM CASES* • 2006 - 2007 Burkina Faso, Cote d’Ivoire, Ethiopia, Mali, Niger, Nigeria, Togo • 2007 – 2008 Ghana • 2009 Sudan *as indicated at May 2004 World Health Assembly RECENT PUBLICATIONS Voelker, R, 2007, Persistence pays off in Guinea worm fight. JAMA vol:298 iss:16 pg:1856 -7 . IN MEMORIUM Dr. Ralph Muller died in England on October 11 after being ill for several months. Most recently an Honorary Senior Lecturer at the London School of Hygiene and Tropical Medicine (LSTMH), he began his long and distinguished career in helminthology at Nigeria’s University of Ibadan, and served for many years as the director of the Commonwealth Institute of Parasitology in England as well as a Lecturer and Senior Lecturer at the LSTMH. He was the world’s foremost authority on the biology of Dracunculus species. One of the earliest advocates of dracunculiasis eradication, he was a prominent participant in the first international meeting on dracunculiasis, the Workshop on Opportunities for Control of Dracunculiasis, which was held in Washington, D.C. in June 1982. He compiled an exhaustive, invaluable 177-page long Bibliography of Dracunculiasis (with nearly two thousand citations) as part of the published report of that historic meeting. We extend our profound condolences to his family. Dr. K. A. Ojodu passed away in Nigeria on September 10, less than two weeks before his 60th birthday, and less than three months after his retirement from public service, following a motor accident while en route from Lagos to Abuja ten days earlier. He received his PhD and MPH degrees from Johns Hopkins University, and was a Lecturer at the University of Lagos from 1981 until 1984, when he was posted to the Federal Ministry of Health as assistant chief scientific officer. He served as national coordinator for Nigeria’s Onchocerciasis Control Program from 1989 to 1992, and as national coordinator of the Guinea Worm Eradication Program from 1995 to June 2007. We extend our profound condolences to his family. Inclusion of information in the Guinea Worm Wrap-Up does not constitute “publication” of that information. In memory of BOB KAISER For information about the GW Wrap-Up, contact the WHO Collaborating Center for Research, Training, and Eradication of Dracunculiasis, NCZVED, Centers for Disease Control and Prevention, F-22, 4770 Buford Highway, NE, Atlanta, GA 30341-3724, U.S.A. FAX: 770-488-7761. The GW Wrap-Up web location is http://www.cdc.gov/ncidod/dpd/parasites/guineaworm/default.htm. CDC is the WHO Collaborating Center for Research, Training, and Eradication of Dracunculiasis.