From: AAAI Technical Report WS-97-05. Compilation copyright © 1997, AAAI (www.aaai.org). All rights reserved.
Distributed Medical Evacuation Planning:
What Problem Should Each Agent Solve?
Victor Saks*, GretchenBraidic*, AlexanderKott*, Core), Kirschner+
{saks, braidic, akott}~cgi.com,
Carnegie Group, Inc*
Five PPGPlace
Pittsburgh, PA15211
Abstract
In the applied research being described here, there is a
natural decomposition of a planning problem along
geographiclines, whereeach sub-problemis to be solved
by an agent whoseorganizational authority covers the
geographicsector. However,
the nature of the problemis
such that each agent’s solution has major impacton the
problem to be solved by other agents, and multiple
iterations of definiag the problemsolving process are
required,until a processis agreeduponwhichis acceptable
to the users as well as algorithmicallysound.Weformulate
the conceptof"constraint trespassing", whichoccurs when
agents imposeconstraints on resources ownedby other
agents, and emphasizeand illustrate the importanceof
minimizing
it.
Introduction
In the applied research being described here, there is a
natural decomposition of a planning problem along
geographic lines, where each sub-problem is to be solved
by an agent whose organizational authority covers the
geographic sector. However,the nature of the problem is
such that each agent’s solution has major impact on the
problem to be soiled by other agents. First, during the
problem solving process, demands of one agent become
modified demands of other agents. In addition, the
organizations represented by the planning agents own
certain of the resources to be used to satisfy demands,
including the demandsof other agents. Thus the task of
clef’ruing the overall problemsolving process to be used by
the collection of agents as a whole, and in particular the
problem to be solved by each agent has been an ongoing
challenge.
In this paper, we will begin by discussing the
application problem, namely medical evacuation. Then we
will discuss several different problem solving process
definitions, and in particular, the defmitionsof the problem
that each agent wouldsolve, that we explored at a design
level, together with their advantages and disadvantages,
from both domain requirement
and algorithmic
perspectives. Then we will discuss which of the problem
kirscimc~transcom.safb.af.mil
USTRANSCOM/TCSG+
Bldg #1700, Room1160
203 West Losey Street
Scott AFB,[L 62225-5209
solving processes we implementedtogether with their user
reactions and lessons learned and finally draw some
conclusions.
Weformulate the concept of "constraint trespassing",
which occurs whenagents impose conslraints on resources
owned by other agents. An owner/agent is willing to
accept a dem~dfrom other agents, but not a constraint on
its resources. Thus we formulate the following design
principle: Design your problem solving process and
supporting soitware to minimize constraint trespassing,
that is, implicit or explicit posting of conslraints by agents
on non-ownedresources.
Medical Evacuation Following a twenty year period
during which time the Department of Defense collected
factual and anecdotal accounts of seriously wounded
patients being put at risk by having their care delayed due
to evacuation planning and coordination, the Commanderin-Chief, USTransportation Command,
resolved to correct
this problem. As a result, In early 1993, the DoD- via
Directive 5154.6 and Instruction
6000.11- tasked
USTRAHSCOM
to consolidate the control of medical
regulation and aeromedical evacuation under a single
command. The resulting
initiative,
the TRAC2ES
(TRANSCOMRegulating
and Command and Control
Evacuation System) enterprise,
codifies policies,
procedures, doctrine, execution decision support, end
advanced automated information technologies that permit
resource constrained and unconstrained patient movement
actions.
From its inception, TRAC~ES
has involved users in
shaping its "to be" vision via national award winning
business process re-engineering and the incorporation of
multi-disciplinary
user feedback.
USTRAHSCOM
sponsored numerous Corporate Information Management
(CIM) workshops, each of which focused on reengineering a portion of the patient regulating and
evacuation process into a seamless whole. Medical
regulating is the process that selects and reserves a
destination hospital bed, and the care associated with it, for
a patient being moved from one Medical Treatment
Facility (MTF)to another. Medical evacuation is the
129
been entered at numerousoriginating MTFs.SomePMRs
process of actually movinga patient once the patient is
canbe satisfied withinthe theater, throughan intra-theater
regulated.
Regulation/evacuation had been a two-step process
move,and somemust be sent to another theater. Most
wherea regulator considers each patient and attempts to
patients with serious injuries are sent to the U.S., perhaps
after short stays in MTFs
in supportingtheaters until they
locate an available MTFbed. Once this is found, the
patient is handedoff to an evacuation planner whofinds
are stabilized.
The following requirements are levied on the
suitable airlift resources to movethe patient to the MTF
TRAC=ES
planning algorithm in addition to the standard
bed. Oneof the major changesin the "to-be" process is
requirementsof quickly producingacceptably goodplans
that the regulation and evacuation solutions should be
integrated into one seamless decision process. TRAC2ES andensuringthe highestquality medicalcare for patients:
providesautomatedsupport for this newbusiness practice
Respect organizational authority, do not make
by proposinga lift-bed solution for movingthe patients.
.
organizations request or give up use of resources
Rather than seeking a bed first, and then looking for the
(airlift andbed) theyown.
lib the TRAC2ES
planning algorithms consider lift and
bedtogether.
TheTRAC2ES
system will support medical regulation
2. Minimizeconflicts for sharedresources, or resources
whichare potentially shared.
and evacuation on a global distributed networkaccessed
by hundredsof users. The current release of TRAC2ES
is
The end result of the process must produce a full
in use at exercises and sites around the world for
.
itinerary for patients including assignmentsto the
evaluation purposes. It will replace the legacy systems
destination MTFand the air mission or missions to
usedfor regulation/evacuationin 1998.
deliver themthere.
Problem Statement
Theworld is divided into theaters, whichare geographic
areas of responsibility. Eachtheater is assigned to a
Commander-in-Chief(CINC)whois allocated military
resources and organizationslocated within his geographic
area in support of a broad continuing military mission
(e.g., PACOM,
the Pacific theater). A Supported
CombatantTheater CINCproduces patients that require
medical support outside of the theater. A Supporting
Theater CINCis designatedto receive and treat patients
fromone or moresupportedtheaters.
Each operational theater has a Theater Patient
MovementRequirements Center (TPMRC).The TPMRC
is the organization/local agent responsible for movement
of patients both within and out of the theater that it
supports. The organization/global agent that monitors
world-wide patient movementand addresses resource
conflicts betweentheaters is called the Global Patient
MovementRequirements Center (GPMRC).
Apatient begins movement
at an OriginatingMilitary
TreatmentFacility (MTF).This is wherepatients receive
their initial treatment and are preparedfor transit. The
DestinationMTFis the hospital that the patient will be
movedto. This hospital must support the medical
specialty(e.g., cardiaccare) requiredbythe patient.
Patients are movedbetweenMTFswithin a theater.
This is called an Intra-Theater move.Theyalso can be
movedfrom an MTFin one theater to an MTFin another
theater. This is called an Inter-Theatermove.
Each TPMRC
has the responsibility to satisfy a
collection of Patient Movement
Requests(PMRs)that have
4.
Onesystemin peace and war.
Resource Ownership, Managementand
Contention
Each MTFcan report the number of beds that it has
available to handle incoming patients. The beds are
managedby the theater in whichthe MTF
is located. If
different TPMRCs
can assign patients to MTFs
in the same
theater, for exampleCONUS
(the U.S.), then they will
contendfor the samebeds
TPMRCs
mayassign patients to both dedicatedairlift,
whichis solely used for the movementof patients and
opportune airli~ which may be moving cargo or
passengers.
All inCa-theaterairlif~ is ownedby the theaters, for
example, EUCOM,
the Europeantheater has a dedicated
fleet of C-9 airplanes for flying patients within Europe.
The TPMRC
in Europecontrols the stops, medical crew
andpatient manifestfor these missions..
In practice, the division of the worldinto theaters is
not a strict partition, andtheaters can havedual roles and
hierarchical relationships with each other. The most
important theater is CONUS.In CONUS,the GPMRC
serves tworoles: GlobalArbiterfor inter-theater lift and
CONUS
TPMRC.Inter-theater
lift is owned by the
TRANSCOM
CINC and aero-medical missions are
planned and managedby the GPMRC.
Dependingon the
problemsolving process, different TPMRCs
can contend
for the sameinter-theaterlift.
130
In addition, the large theaters commands,
EUCOM
in
Europe and PACOM
in the Pacific, really contain the
smaller theaters near them. Thus, EUCOM
can be said to
contain the Bosnia theater, as well as CENTCOM,
and
PACOM
includes Korea. Perhaps the main point to be
madehere is it that has been extremely difficult to
precisely identify resource ownershipby the different
theaters, which has severely complicated the task of
defining problemsolving process and obtaining user buyin.
Problem Formulated as CSP
Wenowformulate the planning problemas a Constraint
Satisfaction Problem,emphasizing
the capacity constraints
whichare the keyconstraintsaffectingagentinteraction:
GIVEN:
¯ a list of patients to moveto an MTF
whichcan treat
them
¯ a list of airports
¯ a list of missionsconnectingthe airports
¯ a list of MTFs,each of whichis co-locatedwith at
least oneairport
¯ a list of ASFs,Aeromedical
StagingFacilities, which
are temporary
holdingfacilities at airports for patients
changingmissions
TheSOLUTION
consists of specifying, for each patient,
an acceptable destination MTF
and a sequenceof missions
whichwill take the patient fromtheir currentlocationto
the destination MTF.
TheSOLUTION
is subject to the followingconstraints:
¯ mission aircraft capacity cannot be exceeded
¯ MTFbed capacity cannot be exceeded
¯ ASFbed capacity cannot be exceeded
This formulationignores manyof the constraints that make
the medicalevacuation problemso complex,for example,
patient medicalconditions that must be treatable by the
destinationMTF,restrictions on patient itineraries suchas
a maximum
numberof stops the patient can tolerate and
maximum
altitude at whichthe patient can fly. Hereweare
interested in listing the capacityconstraints whichare the
key constraints affecting agent interaction, and will
discuss eachof the problemsolving definitions in terms of
capacityconstraint.
The TPMRCPlanning Algorithm
Our basic planning and scheduling technology is
Constrained Heuristic Search (Fox, Sadeh & Baykan,
1989) using the texture measures of contention and
reliance (Sadeh1991)whichwereoriginally definedin the
Micro-Boss system to solve the job-shop scheduling
problem.. Wefirst adapted this approachto solve the
military logistics distribution problemin the KBLPS
Distribution Planner (Saks, Kepner&Johnson1992; Seks,
Johnson&Fox 1993). Our approachis based on Sadehin
which resources maintain demandprofiles whichallow
contention over time to be measured.The algorithmfirst
selects the resourcewhichis mostheavily contendedfor at
a specific time within the planning horizon, and assigns
those resources to the demandswhichrely on themmost
critically, takingdemand
priority into account.
The logistics distribution problemincludes many
complexresource constraints not normallydealt with in
job-shop scheduling, such as product inventory, and
complexdemandconstraints such as splittable orders. To
reasoneffectively on these kinds of constraints, wehadto
significantly generalize Sadeh’searlier research. See
(Beck et. al. 1997) for somedifferent approaches
reinterpreting contentiontexture measurements.
Later, in solving the medicalevacuation problemin
the TRAC2ES
(Kott and Saks 1996) system, we took the
KBLPS
Distribution Planneras a starting point, since both
problems focus on transporting commoditiesthrough a
distribution network.However,patient evacuation again
requires reasoning on a new collection of complex
constraints. For example, in the KBLPS
problem, the
distribution network could be represented as a tree,
whereas for TRAC2ES,mission routing is fairly
unconstrained. Thusin the KBLPS
Distribution Planner,
wepre-calculated all routes, whereasin TRACES,
mission
routes and patient path/itineraries are dynamically
calculated.
In the TRACZES
planning algorithm, each patient has
a "Path Preference Manager(PPM)",whichfunctions like
a travel agent, searchingthe lift-bed networkto construct
goodcandidatepath/itineraries for the patient. EachPPM
has knowledgeof howto take into account the patieafs
constraints andpreferencesin its pathsearch, as wellas in
computingthe contention and reliance measures. For
example,in case the patient is Urgent,the PPM
adjusts the
reliance for the patient to guaranteethat the Urgentpatient
will be scheduledahead of all Routinepatients whoare
contendingfor the sameresources. In addition, the PPM
has the authority to bumpalready scheduled routine
patients fromtheir assigneditinerary. Forroutine patients,
in case the patient is runningout of acceptablepaths, the
PPM
raises the patient’s reliance, increasingthe likelihood
that the patient will be chosenfor assignmentsooner.
Distributed Planning Process
As part of developing TRAC2ES,
Carnegie Group and
TRANSCOM
personnel explored many different
approaches for defining the overall problem solving
131
process and defining the roles of the TPMRCsand
GPMRC
and their interactions.
Very little attention was given to negotiation schemes
between the TPMRCs,
since, in the military, peer-to-peer
negotiation to resolve conflicts is simply not the normal
way of doing business. Thus we were most interested in
approaches which would minimize, and if possible,
eliminate conflicts between different TPMRC
plans. In
case of conflicts and/or suboptimalities, the GPMRC
must
get involved and arbitrate a solution or negotiate with the
TPMRCs.
Decomposition with truly limited interaction is
impossible because theaters send patients to each other:
one theater’s patients end up in another theater, consuming
resources,
and possibly
becoming new movement
requirements, according to several, but not all, of the
processes we explored.
Wealso were required to work within the constraints
of resource ownership in order to reduce the amount of
authorization
(e.g., CONUS
granting permission for
EUCOM
patients to occupy CONUSMTFbeds) necessary
to implement a plan that is created by our algorithms.
Understanding and accommodatingthe ownership of beds
and lift is not a trivial problem.
in addition, as discussed before, TRANSCOM
has
been and still is re-engineering the business practice of
patient regulation and evacuation. Thus we have been
attempting to design a system to solve a problem for a
process whichis itself incompletelydefined, and is still a
movingtarget. To say the least, that has madeour task that
muchmore difficult.
An important simplification is the Hub and Spoke
concept. This is similar to the hub concept used by
commercialairlines in the U.S (see, for example, Aykin,
1995). Each theater designates certain airfields as hubs,
and inter-theater flights into the theater wouldenter the
theater through a hub. Interaction between the TPMRCs
is
substantially simplified by the use of hubs. In particular,
the impact of incomingpatients to a theater, usually the
U.S., for subsequent redistribution to a destination MTF,
would be unmanageableif those patients could fly in to
any airport, as opposed to a relatively small number of
hubs from which they will be redistributed as required. See
(Steppe et al., 1997)for an in depth modelof redistribution
of patients arriving into hubs in the CONUS,.
Numerous paradigms were explored for structured
problem solving approach for TRAC2ES and the
GPMRC/TPMRCinteraction.
Together with each
paradigm, we will discuss
its advantages
and
disadvantages, as well as the extent of its constraint
trespassing.
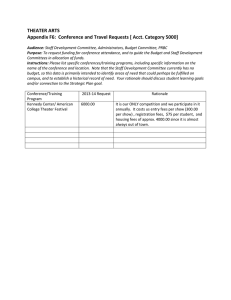
Different Problem Definitions
In order to clarify the distinctions between the different
problem definitions,
each will be accompanied by a
diagram, which shows the movementof a patient from
CENTCOM
to CONUSthrough EUCOM.Each movement
leg is highlighted,
showing which TPMRCor GPMRC
madethe decision to movethe patient along that leg. As
mentioned before, CENTCOM
functions like a sub-thester
of EUCOM,and thus the CENTCOM
to EUCOM
leg is
considered to be inrra-theater, with EUCOM
owning the
lift.
The identification
of the GPMRC
and CONUS
TPMRCmeans that either of them can plan resources
ownedby CONUS
without constraint trespassing.
I. Global Solve
~dgin
Q,,_...C.-"
(
Des~
.....
GPMRC
creates all patient itineraries for patients needing
movement.In manydistributed planning contexts, global
solve is not an option, because each agent may have
sPecialized knowledge which is not, and should not be,
accessible to other agents. Also, certain agents mayhave
access to private data which maynot be revealed to other
agents. In the current context,
none of these
disqualifications apply, and so global solve could be a
viable option. Global solve is how a non-distributed
planner wouldproduce a plan.
Advantages:
¯
This ensures an integrated conflict-free solution.
Disadvantages:
¯
¯
It could potentially become an unmanageable data
problem and risk of computational explosion.
However,recent contingencies (e.g., Operation Desert
Storm) have generated a patient load that could
reasonably be planned by a single process at the
GPMRC.
TPMRCs
do not control their ownassets.
Constraint Trespassing:
¯
132
Maximumconstraint trespassing on all TPMRCs,on
the missions into CENTCOM
and EUCOM,and on
the ASFsat the hubs in those theaters.
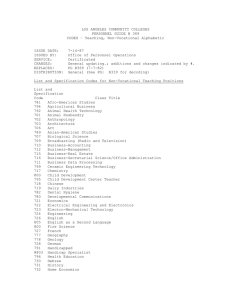
II, TPMRC
plans end-to-end.
~rigin
MT~
The originating TPMRC
plans its patients all the way
throughto their destination MTF.
Advantage
Simplesolution process that allows one organization
to be responsible for the creation of a full patient
itinerary.
Disadvantages
¯
¯
Conflicts for lift and beds can occur anywherealong
the way,and especially in CONUS.
This approachdoes not respect the resourceownership
of eachtheater.
ConstraintTrespassing:
CENTCOM
is trespassing on missions in EUCOM
and CONUS,
on the MTFbeds in CONUS
and on the
ASFbeds in the hubs
Weexplored several variations here to reduce conflicts.
First, that the TPMRCs
share data so that the TPMRC
internal algorithm can take a global view. The TPMRC
wouldproduceits portionof a plan, taking into accountthe
global situation (current andforecasted)so that it can
integrated with other theater plans withoutmajorrework.
Thefoundationof this approachis basedon the ideas
of Distributed Micro-Boss(Sycara et al. 1991) which
expandsthe concepts of Micro-Bossso that they can be
applied to a distributed schedulingproblem.Distributed
Micro-Bosshas focused on the manufacturingdomainand
this effort wouldbe the first application of its demandbasedcoordinationprotocols techniquesto transportation
anddistribution problems.
The key concept here is to improveoverall system
performance by developing protocols through which
agents exchange information about their demandsand
available capacities. In (Sycaraet al. 1991)it has been
shownthat by exchangingdemandprofiles, agents can
focus on the most critical decisions within the overall
systemrather thanfocusonlocally critical decisions.
In this earlier work,eachagentm~kesone requestat a
time, and as manyas possible of the requests are grantecL
However,this mechanism
is too simplistic, since TPMRC
users require as completea solution as possible fromone
run, and this type of extended collaborative solve is
unacceptable. In addition, in our problem where the
agents have different
priorities
based on
supported/supporting
relationships,it is crucial that agents
with higher priority have their requests honoredas fits
their priority. Moreover,
patients themselveshavedifferent
priorities whichmustbe respected. Thusthis approachis
technically risky, requiring major newideas whichtake
priority and other domainspecific conceptsinto account,
and wasnever fully designed.
Wealso explored imposingan ordering on different
TPMRCs
planning, so each sees what the others before it
have planned. The ordering could be based primarily on
supportedTPMRCs
planningfirst, becausethey have first
priority for using shared resources. However,TPMRC
users wouldnot accept being forced to plan at specific
times. Moreover,if a TPM_RC
user needsextra time to edit
a plan and/orexplorewhat-ifpossibilities, the scheduleis
thrownoff.
This paradigmwouldcertainly introduceconflicts for
beds any time more than one TPMRC
is sending patients
to CON-US,
and for lift any time morethan one TPMRC
is
sending patients to CONUS
from the samedirection. This
paradigmis the simplest for TPMRC
users, since they can
plan a full ticket for patients on their own.However,
even
with explicit GPMRC
deconfliction, it mayrequire many
iterations to reacha feasibleplan, let alonean optimalone.
Theflaws accompanying
the previous approaches,and
in particular the extensive constraint trespassing,
convincedall the involvedparties to worktogether to fred
better approacheswhichnowfollow.
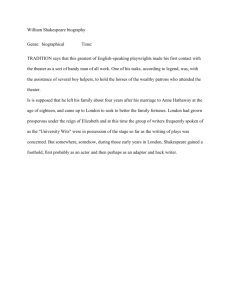
III. Hub-and-Spoke
1.
~rigin
.......
CEC~OM
MTF
Each TPMRC
plans patients only to a hub in the
destination theater. The destination TPMRC,
usually
CONUS,
is then responsiblefor incorporatingthe patients
whorequire onwardmovement
from the reception point in
with their organic theater requirements, developing a
compositelift-bed plan, and notifying the sendingTPMRC
133
of a completeditinerary for their patients prior to their
departurefromthe sendingtheater.
Advantages
Advantage
¯
¯
Eliminates conflicts for beds and intra lift
destinationtheater.
in
¯
Disadvantages
¯
¯
If each TPMRC
selects destination hubs without
coordination
among the TPMRCs,the CONUS
redistribution problemmaybe undulydifficult andthe
fmal solution may be suboptimal, because extra
missions maybe required due to patients being
scattered at different hubs. Alternatively, one hub
maybe clogged with too manypatients to handle
while other hubs have excess available patient
handlingcapability.
TwoTPMRCs
must be involved in the creation of a
singleinter-theateritinerary.
A TPMRC
has total control for planning patients on
the lift andbedresourcesthat theyown.
Therewill be no conflicts for resources becauseeach
TPMRC
plans all patients (regardless of their
originating theater) who need access to their
resources.
Disadvantages
Fragmentedsolve - multiple TPMRCs
must work to
completea single itinerary
A bad decision maybe madewhenstaging a patient to
a hub, since the originating theater does not have
visibility into the remaining
legsof the patient’strip.
ConstraintTrespassing:
¯
ConstraintTrespassing:
Constrainttrespassinghas beeneliminated.
Experience To Date
A significant
improvement over the previous
approaches. Destination theater no longer has
trespassing on its MTFbeds and intra-lift. But the
sending TPMRC
is still trespassing on the inter-lift
into the other theaters andtheir ASFbeds.
IV. Hub-and-Spoke2.
~dgin
cE. MMTF
oN--co.u
Each TPMRC
plans patients only to a hub in its own
theater. Each TPMRC
is responsible for planning the
patient movesinto its owntheater on its ownlift. The
destination TPMRC
is responsiblefor developinga lift-bed
plan from its ownhub to final destination MTFin its
theater. Since most patients go to CONUS,
most intertheater planning is done by the CONUS
TPMRC.
Thus this
paradigmis very similar to a paradigmfor whicheach
TPMRC
performsits ownintra-theater planning, and all
inter-theater planningis doneby a single agent
An operational prototype of the planning algorithm was
presented to the users for evaluation in 1995. This
algorithm utilized the concept described in Hub-andSpokel (paradigm Ill). The software wouldnot present
the itinerary for viewinguntil all legs of the patient’s
itinerary hadbeen planned.This meantthat the itinerary
wasnot available until both theaters had completedtheir
planning. This is different than the current manual
process, becausethey can currently vieweach half of the
itinerary as soonas it is created. Theusers stated that this
wasnot acceptable.
The next version of TRAC~ES
software was built to
support contingency operations like Operation Desert
Storm and Operation Joint Endeavor. This version
employedthe TPMRC
Plans End-To-End(paradigm II).
Althoughin this version, TPMRC
users wereable to plan a
full ticket itinerary for a patient without waiting for
another TPMRC
to complete the itinerary, TPMRCs
did
not acceptit, primarilybecausethey couldnot control the
assets that they own.
The version of TRAC2ES
that is currently in
developmentwill utilize the Hub-and-Spoke2
(paradigm
IV). It will be deployed world-widein 1998 and will
become the definitive system for planning patient
movement.Current users are supporting this paradigm
because it most allows the theater that "owns" the
resourcesto allocate themto patients.
This is also the preferred algorithmicparadigm,since it
eliminates resource conflicts betweendifferent TPMRCs.
134
Theuser interface will be improvedso that TPMRC
users
canvieweachpart of the itinerary as soonas it is created.
Conclusions
In complexreal-world dis~buted planning problems,
defining a structured problemsolving approachand agent
interaction is a challenging task and a critical key to
successful system development.Whenthe relationships
betweenthe different agents are not well defined by an
already existing business practice, then requirementsto
respect agent authority and other agent needs whichmay
not be well specified can be the drivers of the system
architecturedefinitionprocess,overridingpure algorithmic
considerations.
In particular, whenthe nature of the problemsis such
that during the planning process, demandsof one agent
becometransformed into demandsof other agents, then
great care mustbe given to defining agent interactions
whichare acceptable to the different organizations, and
whichalso support a workableplanning process in which
agent conflicts are minimized.It shouldbe expectedthat
multipleiterations of defining the problemsolving process
will be required, until a process is defined whichis
acceptableto the users as well as algnrithmicallysound.
Weformulatethe conceptof "constraint trespassing",
whichoccurs whenagents imposeconstraints on resources
ownedby other agents. Weillustrate the concept of
"constraint trespassing" by showinghowit applies to
several problem solving process definitions. Our
experiencehas shownus that an owner/agentis willing to
accept a demand
fromother agents, but not a constraint on
its resources. Thuswe formulate the following design
principle: Design your problem solving process and
supporting software to minimizeconstraint trespassing,
that is, implicit or explicit postingof constraints on nonownedresources. Weillustrate this design principle by
finally defining a problem solving process which
incorporates it and whichusers haveindicated they will
accept.
Theviews expressesin this article are those of the
authorsanddonot reflect the official policy or position of
the United States Transportation Command,the
Departmentof Defense,or the UnitedStates Government.
AndyHollencamp,Rick Ragsdale, and especially to Phil
Mahlumfor helping to clarify and write someof the
domaininformation.
References
Aykin,T. 1995. Networking
Policies for Hub-and-Spoke
Systemswith Applicationto the Air Transportation
System.In TransportationScience290).
Beck, J.C., Davenport,A.J., Sitarski, E., and Fox, M.S.
1997. Beyond Contention: Extending Texture-Based
SchedulingHeuristics. In ProceedingsAAAI-97.
Fox, M.S., Sadeh, N. and Baykan,C. 1989. Constrained
Heuristic Search. In Proceedings of the Eleventh
InternationalJoint Conference
on Artificial Intelligence.
Kott, A. and Saks, V. 1996 Continuity-Guided
Regeneration: An Approachto Reactive Replanningand
Rescheduling,In Proceedingsof the Florida Artificial
Intelligence Research Symposium,
FLAIRS-96,KeyWest,
Florida.
Sadeh, lq. 1991. Look-ahead Techniques for MicroopportunisticJob ShopScheduling.Ph.D.thesis, Schoolof
ComputerScience, CarnegieMellonUniversity.
Saks, V., Kepner, A. and Johnson, I. 1992. Knowledge
Based Distribution Planning, In Proceedings of the
American Defense Preparedness Association AI
conference.
Saks, V., Johnson, I. Fox, M. S. 1993. Distribution
Planning: A Constrained Heuristic Search Approach,In
Proceedings of the Canadian DNDWorkshop on
AdvancedTechnologiesin Knowledge-Based
Systems.
Steppe, J., Lorraine, J., Saks, V., and Mahlum,P. CONUS
ModelDesignDocument,in preparation.
Sycara, K., Roth, S., Sadeh, N., and Fox, M, 1991.
Distributed Constrained Heuristic Search, In IEEE
Transactions
on
Systems,
Man,
and
Cybernetics.21(6):1446-1461
Acknowledgments. We thank the United States
Transportation Command
for the support to develop
TRAC2ES
and for permission to publish this paper. The
first three authors thank Lt. Col. CoreyKirsclmerfor his
dedication to the medicalevacuationprocess and for his
leadership in managing the TRAC2ES
project. Many
thanks also to all of our colleagues whowehave enjoyed
workingwith, including Bill Elm, Ivan Johnson,Michael
Bett, BobErhard, RonBall, Jeff Stonebrook,Jerry Agin,
135